ABSTRACT
http://dx.doi.org/10.1590/1678-775720150203
The presence of Helicobact er pylori in oral cavit ies
of pat ient s wit h leukoplakia and oral lichen planus
0DJGDOHQD.$=$12:6.$'<*'$à$,UHQD'8ĝ0DáJRU]DWD5$':$12&=.2
:URFODZ0HGLFDO8QLYHUVLW\'HSDUWPHQWRI3HULRGRQWRORJ\8QLWRI2UDO3DWKRORJ\:URFáDZ3RODQG
&RUUHVSRQGLQJDGGUHVV,UHQD'XĞ'HSDUWPHQWRI3HULRGRQWRORJ\8QLWRI2UDO3DWKRORJ\:URFODZ0HGLFDO8QLYHUVLW\.UDNRZVNDVWUHHW
Wroclaw - Poland - Phone: +71-784-03-81 - Fax: +71-784-03-80 - e-mail: [email protected]
6XEPLWWHG0D\0RGL¿FDWLRQ6HSWHPEHU$FFHSWHG6HSWHPEHU
O
bj ect ive: Helicobact er pylori infect ion is one of t he m ost com m on bact erial infect ions in m en. This gast roint est inal pat hogen is closely relat ed t o gast rit is, pept ic ulcers, and t he incr eased r isk of gast r ic cancer. Num er ous st udies have indicat ed oral cavit ies as possibleHelicobact er pylor i r eser voir s. Helicobact er pylor i has been det ect ed bot h in supragingival
and subgingival plaques, and also in saliva. I n addit ion, t he r elat ionship bet w een lesions of oral m ucosa and t he pr esence of H. pylor i has been evaluat ed and descr ibed in som e st udies. The aim of t his st udy was t o assess t he pr esence of Helicobact er pylor i DNA in t he oral cavit y of pat ient s w it h oral leukoplakia and oral lichen planus. Mat er ial and Met hods: The st udy included 54 pat ient s w it h oral leukoplakia, 72 w it h oral lichen planus lesions, and 40 healt hy cont rols. The presence of Helicobact er pylori in oral cavit y sam ples was analyzed using a single- st ep Polym erase Chain React ion ( PCR) m et hod. All pat ient s under w ent a periodont al exam inat ion and t he following clinical param et ers were collect ed: pocket dept h, bleeding, and plaque indexes. The per iodont al st at us was assessed using t he Offenbacher FODVVL¿FDWLRQ5HVXOWV,QPRVWSDWLHQWVSDWKRORJLFDOOHVLRQVZHUHLQW\SLFDOVLWHVRQWKH buccal m ucosa ( leukoplakia in 88% , and oral lichen planus in 93% of pat ient s) . The DNA of t he Helicobact er pylor i was pr esent in 20% of pat ient s w it h leukoplakia and 23% of SDWLHQWVZLWKOLFKHQSODQXV:HGLGQRW¿QGWKH'1$RIH. pylor i in healt hy cont r ols. The
per iodont al st at us descr ibed by per iodont al indices was w or se in t he invest igat ed gr oup WKDQLQWKHFRQWUROJURXS&RQFOXVLRQ7KHVH¿QGLQJVVXJJHVWWKDWWKHH. pylor i pr esence
in oral cavit ies m ay be r elat ed w it h leukoplakia and lichen planus oral lesions.
Ke y w or ds: Helicobact er pylor i. Leukoplakia. Lichen planus.
I N TROD UCTI ON
The Helicobact er pylori ( H. pylori) is one of t he m ost com m on and w ell- k now n bact er ium in t he w or ld. I t colonizes t he hum an st om ach and it is responsible for chronic gast rit is, pept ic ulcer disease and, recent ly, has been recognized as a risk fact or for gast ric adenocarcinom a. The H. pylori infect ion is considered a serious t ransm issible disease. The exact way of t ransm ission of t hese bact eria is st ill debat ed, alt hough som e ev idence suggest s t hat it is m ost likely t o happen during a direct person-t o- person conperson-t acperson-t6. Apart from it s presence in t he
st om ach, t he H. pylori has also been found in dent al plaque and feces. Hence, it is t hought t hat t he rout e of infect ion can be oral- oral or fecal- oral6. The role
of dent al plaque as a reservoir of H. pylori and a
possible source of infect ion or reinfect ion of gast ric m ucosa has been discussed for a long t im e. Som e st udies indicat e a relat ion bet ween t he infect ion of H.
pylori in oral cavit ies and st om achs, but observat ions
concerning t he role of oral cavit y as anot her niche for H. pylori are cont roversial27. I n about 40% of
pat ient s w it h gast rit is, t he bact erium is also present in t he oral cavit y, w hich m ay indicat e t he t ransient charact er of t he infect ion. Nevert heless, it is also suggest ed t hat H. pylori m ay be present in t he oral
HQYLURQPHQWDVQRUPDOEDFWHULDOÀRUD22. H. pylori has
been det ect ed bot h in supragingival and subgingival plaques, and in saliva wit h and wit hout a concom it ant st om ach infect ion11,14.
Oral Lichen Planus ( OLP) is a com m on T-
cell-PHGLDWHGFKURQLFLQÀDPPDWRU\RUDOPXFRVDGLVHDVH
DQWLJHQVSHFL¿F DQG QRQVSHFL¿F PHFKDQLVPV DUH
involved19,23. Possible et iological fact or s ar e: v iral
i n f ect i o n s, m en t al st r ess, m ech an i cal t r au m a, an d in div idu al su scept ibilit y pr obably r elat ed t o genet ic predisposit ions20,26. I t has t ypical bilat eral
localizat ion m ainly on t he post erior buccal m ucosa and on t he lat eral m argins of t he t ongue, and it s clinical present at ions range from a w hit e ret icular plaque t o an at rophic, erosive and rarely of bullous for m . I n t he r et icular for m , t his lesion can oft en be asym pt om at ic. How ever, red form s are painful and spicy or acidic food and m echanical irrit at ions exacerbat e unpleasant sensat ions7,24.
Or al leu k op lak ia is a w ell- k n ow n p ot en t ially m alignant lesion. Based on it s et iopat hogenesis, t here are t w o different form s of t his w hit e lesion – one idiopat hic and t he ot her one associat ed w it h t ob acco u se. Clin ically, t w o t y p es ar e p r esen t : hom ogeneous and non- hom ogeneous leukoplakia. Alt hough leukoplakia can vary hist opat hologically, it s feat ures include hyperkerat osis, ort hokerat ozis or parakerat ozis, acant hosis of t he epit helium , and
FKURQLF LQÀDPPDWRU\ LQ¿OWUDWLRQV LQWR WKH ODPLQD
propria. Also, various degrees of epit helial dysplasia m ay be seen but only in t he m inorit y of lesions9,25
.
Leukoplakia and oral lichen planus are frequent or al m u cou s lesion s. Alt h ou gh bot h pat h ologies have been deeply r esear ched, t her e is a lack of unequivocal observat ions concerning t he relat ion of t hese diseases w it h a Helicobact er pylori infect ion.
The aim of t he present st udy was t o assess t he pr esence of t he H. py lor i DNA in t he oral cav it y of p at ien t s w it h m u cosal p at h olog ies, su ch as leukoplakia and oral lichen planus, and t o exam ine t he hy pot hesis of coex ist ence of bact er ia in t he invest igat ed oral lesions.
M ATERI AL AN D M ETH OD S
All pat ient s provided inform ed consent s before t aking part in t he st udy. There w ere t hree groups: w it h oral leuk oplak ia ( gr oup L) , w it h oral lichen planus ( group OLP) , and t he cont rol group. About 54 subj ect s ( 30 fem ales and 24 m ales) com prised t he group L and 72 ( 55 fem ales and 17 m ales) t he OLP group w it hout any gast roint est inal problem s. The cont rol group consist ed of 40 generally healt hy pat ient s wit hout lesions in t he oral cavit y. All pat ient s w it h leu k oplak ia w er e cu r r en t sm ok er s w it h n o cell dy splasia in t he hist ological ex am inat ion. I n t he group w it h OLP, only t he ret icular or ret icular-erosive form s w ere present . The diagnosis of oral
OLFKHQSODQXVZDVPDGHDFFRUGLQJWRWKHPRGL¿HG
Word Healt h Organizat ions ( WHO) diagnost ic clinical crit eria24.
Exclusion cr it er ia for t he st udy w er e: general ant ibiot ic t reat m ent wit hin t hree m ont hs prior t o t he exam inat ion, pat ient s w it h severe P3 periodont it is
3'PP%23H[WHQWVFRUHDFFRUGLQJWR WKH2IIHQEDFKHUFODVVL¿FDWLRQ15.
The age, t he num ber of t eet h, sm oking habit , and t he sit e of t he oral lesions w ere collect ed from all pat ient s. A com plet e oral/ periodont al exam inat ion was perform ed by a single dent ist ; Pocket Dept h ( PD) was m easured w it h a periprobe at 4 sit es per t oot h; oral hygiene was evaluat ed according t o t he Approxim al Plaque I ndex ( API )12, and t he bleeding
was according t o t he Bleeding on Probing ( BOP)2;
t h e p er iod on t al st at u s w as assessed accor d in g
WR D VLPSOL¿HG SHULRGRQWDO GLVHDVH FODVVL¿FDWLRQ
of Offen bach er, et al.1 5 ( 2 0 0 8 ) . To evalu at e t h e
presence of H. pylori DNA, t w o sam ples w ere t aken from t he prem olar/ m olar int erdent al spaces or from t he per iodont al pocket s, depending on t he st age of periodont ium . The area around t he chosen sit es was dried and isolat ed from saliva. Then, a st erile m icr obr u sh w as in ser t ed in t o t h e space/ pock et , t ransferred t o a st erile Eppendorf t ube, and frozen at - 20°C.
D N A e x t r a ct ion pr ot ocol
Laborat ory t est s w ere carried out ent irely at t he
'HSDUWPHQWRI0ROHFXODU7HFKQLTXHVRIWKH:URFáDZ
Medical Universit y. Each of t he m icro brushes wit h t he collect ed m at erial was placed in a 1.5 m l Eppendorf t ube. Four hundred m illilit ers of st erile wat er ( Sigm a Aldrich Reagent Wat er Molecular Biology) was t hen added t o t he t ubes and vort exed. DNA was isolat ed
XVLQJWKHPRGL¿HG+H[DGHF\O7U\PHW\ORDPPRQLXP
Brom ide ( CTAB) m et hod.
PCR m e t h od
7RFRQ¿UPWKHDFFXUDF\RIWKHVDPSOHFROOHFWLRQ
and t he effect iveness of t he DNA isolat ion m et hod, t he int er nal cont r ol r eact ion for t he pr esence of h u m an b et a- act i n g en es w as car r i ed ou t . Th e react ion was conduct ed w it h t he use of a single-st ep PCR ( GeneAm p® PCR Sy st em 9700, Applied
Biosyst em s, Walt ham , Massachuset t s, USA) . The H. pylori'1$DPSOL¿FDWLRQWHFKQLTXHZDV perform ed properly w it h t he use of locat ed ( nest ed) PCR. I t consist s in t he carrying out of t w o, one aft er anot her, PCR react ions using t w o different pairs of
VXLWDEOHDQGVSHFL¿FSULPHUVWRWKHJHQRPLF'1$RI
bact eria. The described t ype of nest ed PCR react ion is based on t wo st ages. Next , we show t he com posit ion of t he react ion m ixt ure for t w o successive PCR for a
'1$VDPSOH,QWKH¿UVWUHDFWLRQPL[WXUHWRPO
of H2O wat er ( Gibco, I nvit rogen, Paisley, Scot land, UK) w e added 1.0 m l of PCR developing buffer, 0.5
P/RIG173DWDFRQFHQWUDWLRQRINj0PORI
a m ixt ure of prim ers EHC at a concent rat ion of 10
Nj0DQGPORI7DTSRO\PHUDVHUHDFWLRQEXIIHU
for DSF-Taq-Taq pol.Top, Bioron, Ludw igshafen am
5KHLQ *HUPDQ\ ,Q WKLV UHDFWLRQ NjO RI '1$
XVHG LQ WKH ¿UVW UHDFWLRQ (+&8/ ZDV FKRVHQ
for t he 860 bp fragm ent of H. pylori genom ic DNA ( 80 076- 80 492 bp) . I n t he second react ion, 7.65 m l of DNase- free wat er was added, 1.0 m l of PCR
EXIIHUNjORI'73ZLWKDFRQFHQWUDWLRQRINj0 NjOVWDUWHUVWKDWZDVQDPHG(7DIWHUQRPLQDWLRQ
given by Song, et al.22 ( 2000) w it h a concent rat ion RINj0DQGRI7DTSRO\PHUDVH8PO ,QWKHVHFRQGUHDFWLRQZHDGGHGNjORIWKH'1$ DPSOL¿HG LQ WKH ¿UVW UHDFWLRQ 7KH VHFRQG VHW RI
prim ers ( ET- 5U/ ET- 5L) was int ernally direct ed t ot he sequence of 860 bp fragm ent of H. pylori genom ic DNA am p lif ied b y t h e p r ev iou sly u sed p r im er s ( EHC- U/ EHC- L)22.
To v isualize t he PCR pr oduct s, elect r ophor esis was car r ied out in a 1% agar ose gel in t he TAE m ixt ure ( Tris 242 g, 100 m l of 0.5 M EDTA pH 8; 57.2 m l CH3COOH per 1000 m l) in t he pr esence of et hidium br om ide ( a concent rat ion of 10 m g/ m l) . For t he num ber of base pairs, w e used a DNA GeneRuler 100 bp DNA Ladder ( Ferm ent as, Therm o
)LVKHU 6FLHQWL¿F :DOWKDP 86$ DV D '1$ VL]H
st andard. Visualizat ion of elect rophoresis result s was perform ed under UV light w it h t he use of t he Kodak Gel Logic 1 0 0 I m aging Sy st em ( East m an Kodak Com pany) . Exam ples of bot h H. pylori and bet a act in react ions are present ed in Figures 1 and 2.
St a t ist ica l a n a ly sis
The r esult s of t he r esear ch w er e st at ist ically analyzed. The follow ing param et ers w ere calculat ed for all groups: t he num ber of cases ( N) , average values ( X) , t he m edian ( M) , t he range ( m in- m ax) , t h e u p p er an d l o w er q u ar t i l e ( 2 5 Q- 7 5 Q) , an d st andard deviat ions ( SD) .
9HUL¿FDWLRQRIWKHK\SRWKHVLVRIWKHHTXDOLW\RI
each average t rial was conduct ed using t he ANOVA m et hod ( variance analysis) . The Kruskal- Wallis rank sum t est for nonparam et r ic dat a was car r ied out in t he gr oups in w hich t her e was het er ogeneous v ar ian ce. We r ecog n ized Pd0 . 0 5 as st at ist ically
VLJQL¿FDQW 7KH DQDO\VLV ZDV FRQGXFWHG XVLQJ WKH
EPI I NFO 7.1.1.14 st at ist ical soft ware ( dat ed 2- 07-2013) .
RESULTS
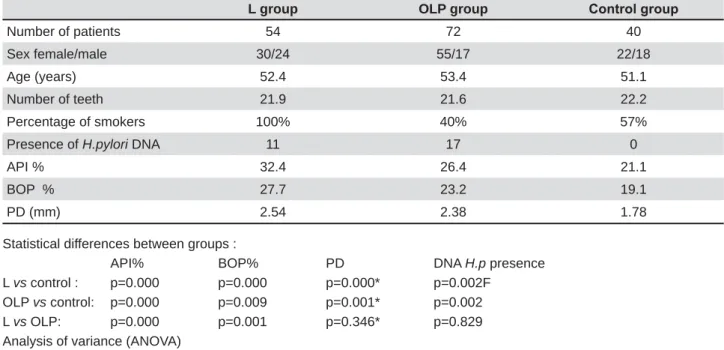
We sum m arized t he clinical charact erist ics of t he invest igat ed and cont rol groups in Table 1.
We found no differences about t he average age and t he num ber of t eet h bet w een t he gr oups of pat ient s w it h leukoplak ia and lichen planus, and t h e con t r ol g r ou p. Fif t y - f ou r p at ien t s f r om t h e leukoplakia group, 29 pat ient s from t he OLP group, and 23 from t he cont rol group w ere sm okers.
Pat hological lesions w ere m ainly present in t he
Figure 1- Results of positive control reactions for the
correct DNA isolation from oral caves - beta actin gene. Description of results: 1- Gene Ruler 100 bp Ladder (Fermentas); 2- Probe n. 9; 3- Probe n. 10; 4- Probe n. 11; 5- Probe n. 12; 6- Probe n. 13; 7- Probe n. 14; 8- Negative control (H2O instead of DNA)
Figure 2- Detection of Helicobacter pylori with nested
t ypical sit es of t he buccal m ucosa ( in 89% of pat ient s w it h leukoplakia and in 93% of pat ient s w it h oral lichen planus) . Ther e w er e no differ ences in t he presence of H. pylori DNA bet w een t he invest igat ed groups. We found t his pat hogen in 20% of pat ient s wit h leukoplakia and in 23.6% of pat ient s wit h lichen
SODQXV:HIRXQGDVLJQL¿FDQWO\KLJKHULQFLGHQFHRI H. pylori DNA in bot h groups w it h oral pat hologies
in com parison t o t he cont rol group ( p= 0.002) , in w hich w e did not det ect t he DNA of such pat hogen ( Table 1) .
The average value of t he API index was st at ist ically higher bot h in t he leukoplakia group in com parison
t o t he lichen planus group ( p= 0.000) and t he cont rol group ( p= 0.000) , and in t he OLP group versus t he cont rol group ( p= 0.000) .
Sim ilarly, t he average value of t he BOP index was st at ist ically higher bot h in t he leukoplakia group in com parison t o t he cont rol group ( p= 0.000) and t he OLP group ( p= 0.001) , and in t he OLP group and t he in com parison t o cont rol group ( p= 0.009) .
The average pocket dept h was st at ist ically deeper in t he leukoplakia group as w ell as in t he OLP group in com parison t o t he cont rol group.
By o n l y co m p a r i n g t h e t w o st u d y g r o u p s according t o t he periodont al st at us, w e found t he
L group OLP group &RQWUROJURXS
Number of patients 54 72 40
Sex female/male 30/24 55/17 22/18
Age (years) 52.4 53.4 51.1
Number of teeth 21.9 21.6 22.2
Percentage of smokers 100% 40% 57%
Presence of H.pylori DNA 11 17 0
API % 32.4 26.4 21.1
BOP % 27.7 23.2 19.1
PD (mm) 2.54 2.38 1.78
Statistical differences between groups :
API% BOP% PD DNA H.p presence
L vs control : p=0.000 p=0.000 p=0.000* p=0.002F OLP vs control: p=0.000 p=0.009 p=0.001* p=0.002
L vs OLP: p=0.000 p=0.001 p=0.346* p=0.829
Analysis of variance (ANOVA) F-Fisher exact test
* Chi-Square test (Yate's correction)
Table 1- Characteristics of patients
H. pylori + H. pylori - Statistical importance
GROUP OLP N=17 N=55
API 26.4% 26.5% p=0.947
BOP 25.5% 22.5% p=0.139
PD 2.88 mm 2.22 mm p=0.003
GROUP L N=11 N=43
API 35.5% 31.7% p=0.030
BOP 32.4% 26.5% p=0.024
PD 3.36 mm 2.33 mm p=0.000
Non-parametrical Kruskal-Wallis test API=Approximal Plaque Index BOP=Bleeding on Probing PD=Pocket Depth
Table 2- Comparison of periodontal indices average values in OLP and L groups in patients with (+) and without (-) the
oral hy giene w as st at ist ically w or se and gingival bleeding was great er in pat ient s w it h leukoplakia. How ever, t here was no difference in t he dept h of t he periodont al pocket ( p= 0.346) .
On t h e o t h er h a n d , t h e p er i o d o n t a l st a t u s described by t he API , BOP, and PD indexes, in bot h of t he invest igat ed groups, was st at ist ically w orse in com parison w it h t he cont rol group, in w hich w e did not det ect t he DNA of H. pylori ( Table 1) .
Furt herm ore, in t he group wit h leukoplakia, t here w er e st at ist ically higher values for t he API , BOP, and per iodont al PD indexes in t hese pat ient s, in w hich w e found t he presence of H. pylori ( Table 2) . Conversely, in t he OLP group, w hose percent age of bact erial DNA was t he highest , t he only st at ist ically
VLJQL¿FDQW GLIIHUHQFH EHWZHHQ SDWLHQWV ZLWK DQG
w it hout t he presence of H. pylori DNA was in t he periodont al PD ( 2.88 m m and 2.22 m m respect ively, p= 0.003) . Alt hough t he average PD was great er in pat ient s harboring t he DNA of such bact eria, it was not described as relat ed w it h periodont it is ( Table 2) .
D I SCUSSI ON
Th e r elat ion sh ip bet w een lesion s of t h e or al m ucosa and t he pr esence of H. py lor i has been evaluat ed and descr ibed in a lim it ed num ber of st udies. An associat ion bet w een gast r oint est inal diseases and apht hae ( oral ulcerat ion) has been dem onst rat ed and t he int erest around t his pat hology and a H. pylori infect ion aroused. Albanidou- Farm aki, et al.3 ( 2005) st at ed t hat 34 out of 48 pat ient s w it h
recurrent m inor apht hous ulcerat ions t est ed posit ive f or H. py lor i. He det ect ed t h e assessed pr ot ein ant ibodies I gG, I gA and ant i- CagA in t he serum of 59 pat ient s and in t he saliva of 24 pat ient s. The aut hors also found t hat t he appropriat e eradicat ion of t he bact eria led t o t he com plet e cure of t he lesions or t o rem arkable im provem ent s. I n anot her invest igat ion, w e observed t he presence of I gG ant ibodies against
H. pylori in 52% of t he invest igat ed pat ient s w it h
recurrent apht hous st om at it is ( RAS) . How ever, t he aut hors found H. pylori DNA in t he ulcerat ions of only one case and concluded t hat t his pat hogen is not relat ed w it h RAS13. Riggio, et al.18 ( 2000) , using
t he PCR, found H. pylori DNA in 3 out of 28 biopsies fr om RAS18. Based on t he r esult s of 22 pat ient s
w it h various m ucosal ulcerat ive disorders ( including r e c u r r e n t a p h t h o u s s t o m a t i t i s , v i r u s h e r p e s sim plex lesions, and erosive lichen planus lesions) , Shim oyam a, et al.21 ( 2000) suggest ed t hat t here is
no associat ion bet w een t hese pat hologies and t he presence of H. pylori. Only t w o out of seven pat ient s w it h a herpes sim plex infect ion t est ed posit ive for
H. pylori – bot h for t he cult ure t est and for t he H. pylori ant igen21. I n an earlier invest igat ion, Port er,
et al.16 ( 1997) exam ined serum I gG ant ibodies and GLG QRW ¿QG DH. py lor i infect ion as an essent ial
et iologic fact or in t h e dev elopm en t of r ecu r r en t apht hous st om at it is and ot her oral m ucosal lesions w it h ulcerat ions16.
Th e e t i o l o g y o f o r a l l e u k o p l a k i a a n d o r a l lichen planus has not been fully explained. I n t his st udy, lesions w er e m ainly in t he buccal m ucosa [ leukoplakia in 48 ( 89% ) pat ient s and in 67 ( 93% )
SDWLHQWVZLWK2/3@:HIRXQGDVLJQL¿FDQWO\KLJKHU
incidence of H. pylori DNA in t he sam ples of t he oral cavit y of pat ient s from bot h st udy groups - 22.2% in com par ison t o t he cont r ol gr oup, in w hich t he bact eria was not present . How ever, t here w ere no st at ist ical differences bet w een t he presence of H.
pylori DNA in t he group w it h leukoplakia - 20% and
w it h lichen planus - 23.6% .
There are no st udies on t he presence of H. pylori DNA in oral cavit y of pat ient s w it h leukoplakia. I n a recent st udy carried out in t he Sout hw est ern of I r an w it h 4 1 pat ien t s, r esear ch er s det ect ed t h e I gG ant i H. pylori in as m any as 52% of oral lichen planus pat ient s and 66% of cont rol group pat ient s.
7KHDXWKRUVGLGQRW¿QGDQDVVRFLDWLRQEHWZHHQD H. pylori infect ion and OLP, regardless of t he clinical
present at ion17.
There is am biguous view as t o w het her or not t he oral cav it y m ay har bor H. pylor i, par t icular ly in per iodont it is pat ient s. By evaluat ing 3 0 adult pat ient s posit ive t o a urease t est w it h diagnosed gingivit is or periodont it is, Gebara and coaut hors10
( 2004) found H. pylori in saliva, in t he supragingival and subgingival plaque of 43.3% of subj ect s, and
D ODFN RI VWDWLVWLFDOO\ VLJQL¿FDQW DVVRFLDWLRQ ZLWK
t he pat ient s’ per iodont al st at us10. Ot her aut hor s DOVRIDLOHGWR¿QGDVLJQL¿FDQWDVVRFLDWLRQEHWZHHQ
periodont al disease and poor oral hygiene and a H.
pylori infect ion4,5.
How ever, based on t he st udy of a cross- sect ional dat a analysis by Dye, et al.8 ( 2002) , it was found
t hat poor periodont al healt h relat ed w it h advanced p er i od on t i t i s ch r act er i zed b y d eep p er i od on t al pocket s m ay be associat ed w it h a H. py lor i oral infect ion.
I n t his st udy, t he oral hygiene and t he periodont al st at us of t he st udy groups w it h leukoplakia and OLP w ere st at ist ically w orse in com parison t o t he cont rol group. This m ay indicat e t he associat ion bet w een t he presence of H. pylori DNA and dent al plaque,
DQGDOVRWKHDVVRFLDWLRQEHWZHHQWKHLQÀDPPDWLRQ
of periodont al t issues and t he presence of H. pylori co u l d b e t ak en i n t o co n si d er at i o n . Th e w o r se periodont al st at us and oral hygiene were also present in H. pylori posit ive pat ient s w it h leukoplakia. I n H.
pylori SRVLWLYHSDWLHQWVZLWK2/3WKHRQO\VLJQL¿FDQW
difference was in t he dept h of t he periodont al pocket . Alt hough t he lev els of oral hy giene and gingival bleeding w ere w orse in t he group w it h leukoplakia, w e saw no st at ist ical difference in t he presence of
highlight t he average periodont al pocket dept h ( 3.36 m m in leukoplakia and 2.88 m m in OLP H. pylori posit ive pat ient s) was not relat ed t o periodont it is. Som e st udies under line t he r elat ionship bet w een t he presence of H. pylori and t he occurrence of a periodont al pocket w it h a dept h of 5 m m or m ore and advanced periodont it is1. Result s of t his st udy
indicat ed t he presence of H. pylori was not relat ed w it h periodont it is.
I n our st udy, w e select ed pat ient s according t o t h e per iodon t al st at u s, w h ich w as ch ar act er ized by m ild periodont it is according t o t he Offenbacher
FODVVL¿FDWLRQ:HH[FOXGHGSDWLHQWVZLWKSHULRGRQWDO
pocket s deeper t han 4 m m and w it h BOP great er t h a n 5 0 % f r o m t h e st u d y. Th e cu r r en t st u d y show s t he associat ion bet w een t he presence of H.
py lor i DNA and pat hological oral m ucosa lesions
such as leukoplakia and oral lichen planus. Since t he evaluat ed st at e of per iodont ium and hygiene levels w ere w orse in pat ient s w it h H. pylori DNA,
WKH LQÀXHQFH RIH. py lor i on t he developm ent of
t hese pat hologies is debat able. On t he ot her hand, t he presence of H. pylori m ay have an addit ional
LQÀXHQFHRQWKHORFDOHQYLURQPHQW&RQVLGHULQJWKH
r ole of H. py lor i in pat hogenesis of oral m ucosal lesions or ulcerat ions is st ill unclear, it seem s t hat pat ient s w it h oral lesions as leukoplakia and oral lich en plan u s, an d con cu r r en t gast r ic pr oblem s, should be t est ed for t he pr esence of a H. py lor i infect ion.
I t is im port ant t o t ake care of pat ient s w ho need t h er ap eu t ic in t er v en t ion s t o im p r ov e t h eir or al hygiene and periodont al st at us and elim inat e any possible addit ional fact ors in t he et iology of t hese lesions.
CON CLUSI ON
The r esult s of t his st udy show t he higher H.
pylori presence in t he oral cavit y of subj ect s w it h
leukoplakia and oral lichen planus w hen com pared
ZLWKFRQWUROJURXS7KHGHVFULEHG¿QGLQJVLQGLFDWH
t hat furt her research on t his t opic is necessary.
REFEREN CES
1- Adler I , Muiño A, Aguas S, Harada L, Diaz M, Lence A, et al.
Helicobact er pylori and oral pat hology: relat ionship wit h t he gast ric
infect ion. World J Gast roent erol. 2014; 20: 9922- 35.
2- Ainam o J, Bay I . Problem s and proposals for recording gingivit is and plaque. I nt Dent J. 1975; 25: 229- 35.
3- Albanidou- Farm aki E, Giannoulis L, Markopoulos A, Fot iades S, Aggouridaki X, Farm akis K, et al. Out com e following t reat m ent for
Helicobact er pylori in pat ient s wit h recurrent apht hous st om at it is.
Oral Dis. 2005; 11: 22- 6.
4- Anand PS, Kam at h KP, Anil S. Role of dent al plaque, saliva and per iodont al disease in Helicobat er py lor i infect ion. Wor ld J Gast roent erol. 2014; 20: 5639- 53.
5- Berrot eran A, Perrone M, Corrent i M, Cavazza M, Tom bazz C, Goncalvez R, et al. Det ect ion of Helicobact er pylori DNA in t he oral cavit y and gast roduodenal syst em of Venezuelan populat ion. J Med Microbiol. 2002; 51: 764- 70.
6 - Br ow n LM. Helicob act er p y lor i ep id em iolog y an d r ou t es of t ransm ission. Epidem iol Rev. 2000; 22: 283- 97.
7- Car r ozzo M, Thor pe R. Oral lichen planus: a r ev iew. Miner va St om at ol. 2009; 58: 519- 37.
8- Dye BA, Kruszon- Moran D, McQuillan G. The relat ionship bet ween periodont al disease at t ribut es and Helicobact er pylori infect ion am ong adult s in t he Unit ed St at es. AM J Public Healt h. 2002; 92: 1809- 15. 9- Freit as MD, Blanco- Carrión A, Gándara- Vila P, Ant únez- López J, García- García A, Gándara- Rey JM. Clinicopat hologic aspect s of oral leukoplakia in sm okers and nonsm okers. Oral Surg Oral Med Oral Pat hol Oral Radiol Endod. 2006; 102: 199- 203.
10- Gebara EC, Pannut i C, Faria CM, Cheht er L, Mayer MP, Lim a LA. Prevalence of Helicobact er pylori det ect ed by polym erase chain of periodont it is pat ient s. Oral Microbiol I m m unol. 2004; 19: 277- 80. 11- Krast eva A, Panov V, Krast eva A, Kisselova A. Oral cavit y and syst em ic diseases – Helicobact er pylori and dent ist ry. Biot echnol Biot ec EQ. 2011; 25: 2447- 541.
12- Lange DE, Plagm ann HC, Eenboom A, Prom sberger A. Clinical m et hods for t he obj ect ive evaluat ion of oral hygiene. Dt sch Zahnarzt l Z. 1997; 32: 44- 7.
13- Mansour- Ghanaei F, Asm ar M, Bagherzadeh AH, Ekbat aninezhad S. Helicobact er py lor i in fect ion in or al lesion s of pat ien t s w it h recurrent apht hous st om at it is. Med Sci Monit . 2005; 11: 576- 9. 14- Mom t az H, Souod N, Dabiri H, Sarshar M. St udy of Helicobact er
pylori genot ype st at us in saliva, dent al plaques, st ool and gast ric
biopsy sam ples. World J Gast roent erol. 2012; 18: 2105- 11. 1 5 - Of f en bach er S, Bar r os S, Beck JD. Ret h in k in g per iodon t al LQÀDPPDWLRQ-3HULRGRQWRO
16- Port er SR, Barker GR, Scully C, Macfarlane G, Bain L. Serum I gG ant ibodies t o Helicobact er pylori in pat ient s wit h recurrent apht hous st om at it is and ot her oral disorders. Oral Surg Oral Med Oral Pat hol Oral Radiol Endod. 1997; 83: 325- 8.
17- Pour shahidi S, Fak hr i F, Ebrahim i H, Fak hraei B, Alipour A, Gh ap an ch i J, et al. Lack of associat ion b et w een Helicob act er
pylor i infect ion and oral lichen planus. Asian Pac J Cancer Pr ev.
2012; 13: 1745- 7.
18- Riggio MP, Lennon A, Wray D. Det ect ion of Helicobact er pylori DNA in recurrent apht hous st om at it is t issue by PCR. J Oral Pat hol Med. 2000; 29: 507- 13.
19- Roopashree MR, Gondhalekar RV, Shashikant h MC, George J, Thippeswam y SH, Shukla A. Pat hogenesis of oral lichen planus – a review. J Oral Pat hol Med. 2010; 39: 729- 34.
20- Sand LP, Jalouli J, Larsson PA, Hirsch JM. Prevalence of Epst ein-Barr virus in oral squam ous cell carcinom a, oral lichen planus, and norm al oral m ucosa. Oral Surg Oral Med Oral Pat hol Oral Radiol Endod. 2002; 93: 586- 92.
2 1 - Sh im oy am a T, Hor ie N, Kat o T, Kan ek o T, Kom iy am a K. Helicobact er pylori in oral ulcerat ions. J Oral Sci. 2000; 42: 225- 9. 22- Song Q, Lange T, Spahr A, Adler G, Bode G. Charact er ist ic dist ribut ion pat t ern of Helicobact er pylori in dent al plaque and saliva det ect ed wit h nest ed PCR. J Med Microbiol. 2000; 49: 349- 53. 23- Sugerm an PB, Savage NW, Walsh LJ, Zhao ZZ, Zhou XJ, Khan A, et al. The pat hogenesis of oral lichen planus. Crit Rev Oral Biol Med. 2002; 13: 350- 65.
24- Van der Meij EH, van der Waal I . Lack of clinicopat hological cor r elat ion in t he diagnosis of oral lichen planus based on t he SUHVHQWO\DYDLODEOHFULWHULDDQGVXJJHVWLRQVIRUPRGL¿FDWLRQV-2UDO Pat hol Med. 2003; 32: 507- 12.
9DQ GHU :DDO , 6FKHSPDQ .3 YDQ GHU 0HLM (+ $ PRGL¿HG FODVVL¿FDWLRQDQGVWDJLQJV\VWHPIRURUDOOHXNRSODNLD2UDO2QFRO 2000; 36: 264- 6.
26- Zhou Y, Jiang L, Liu J, Zeng X, Chen QM. The prevalence of hepat it is C virus infect ion in oral lichen planus in an et hnic Chinese cohort of 232 pat ient s. I nt J Oral Sci. 2010; 2: 90- 7.