Revista de Saúde Pública
I SSN 0034- 8910 versão im pressaRev Saúde Pública 2003; 37(6)
Hypertension and salt intake in an urban population
Maria del Carm en Bisi Molinaa, Robert o de Sá Cunhab, Fernando Luis Herkenhoffb and José Geraldo Millb
a
Depart am ent o de Enferm agem do Cent ro Biom édico da Universidade Federal do Espírit o Sant o. Vit ória, ES, Brasil. bDepart am ent o de Ciências Fisiológicas do Cent ro Biom édico da Universidade Federal do Espírit o Sant o. Vit ória, ES, Brasil
ABSTRACT
Objective
To evaluat e t he salt int ake and urinary Na+/ K+ rat io in a random ized sam ple from an et hnically m ixed urban populat ion.
Methods
A random ized resident ial sam ple of 2,268 individuals aged 25- 64 in Vit ór ia, ES, w as select ed, of whom 1,663 ( 73.3% ) report ed t o t he Univer sit y Hospit al for st andar dized t est s. Salt , Na+ a n d K+ int ake w as est im at ed from 12- hour urine excret ion ( 7 p.m . t o 7 a.m .) and from t he m ont hly salt consum pt ion at hom e report ed in t he int erview . Clinic art erial pressure w as m easured t w ice under st andar d condit ions by t w o t r ained invest igat or s, using m er cur y sphygm om anom et r y. The St udent t and Tuk ey t est s w er e ut ilized for st at ist ical analy sis.
Urinary Na+ excret ion was higher in m en and individuals of lower socioeconom ic level ( P< 0.00 0) . No differ ence bet w een et hnic gr oups w as obser v ed. K+ ex cr et ion w as unr elat ed t o socioeconom ic lev el and et hnicit y, but w as significant ly higher am ong m en ( 25±18 vs. 22±18 m Eq/ 12h; P= 0.002) . Posit ive linear correlat ion was observed bet ween urinary Na+ ex cr et ion and sy st olic ( r = 0.15) and diast olic ( r= 0.19) art erial pressure. Hypert ensive individuals showed higher urinary Na+ excret ion and Na+/ K+ rat io t han norm ot ensive individuals. Report ed salt int ake w as around 50% of t he int ake est im at ed from 12- hour urine collect ion ( around 45% of 24- hour urinary excret ion) .
Conclusions
Salt int ake is st rongly influenced by socioeconom ic level and m ay part ially explain t he higher pr ev alence of hy per t ension in low er socioeconom ic classes.
Keywords
Sodium chloride, ana lysis. Sodium . Pot assium . Hypert ension, epidem iology. Prevalence. Socioeconom ic fact or s.
I N TRODUCTION
Art erial hypert ension is considered t o be a public healt h problem because of it s m agnit ude and risk and t he difficult ies in it s cont r ol. I t is also r ecognized as one of t he m ost im por t ant r isk fact or s for t he developm ent of cer ebr ovascular event s and m yocar dial infar ct .1 4
Sev er al populat ion st udies hav e giv en ev idence of t he im por t ance of cont r o lling hypert ension for t he reduct ion of cardiovascular m orbidit y and m ort alit y. Thus, t he high rat es of cardiovascular m orbidit y and m or t alit y in r ecent ly indust r ialized count r ies appear t o be significant ly dependent on t he high pr ev alence of ar t er ial hy per t ension in such count r ies.2 1 Alt hough t her e ar e no st udies w it h good nat ional- level represent at iveness available regarding art erial hypert ension in Brazil, localized research has show n high prevalence, w it hin t he range of 20 t o 45% of t he adult populat ion.8
I n m ost cases, t he cause of t he hy per t ension is unk now n. How ev er , t her e ar e sev er al fact or s t hat could be associat ed w it h r aising t he ar t er ial pr essur e, such as sedent ar y lifest y les, st r ess, sm ok ing, aging, fam ily hist or y, r ace, gender , w eight and diet ar y fact or s.
Assessm ent of sodium in t he diet is ext rem ely com plex, since it s daily consum pt ion varies subst ant ially. The daily sodium int ake m ay be under est im at ed, since t he differ ences in salt addit ion bet w een people ar e not t ak en int o consider at ion.7 I n addit ion t o t his, anot her problem encount ered in diet ary assessm ent is t he food com pos it ion t able ut ilized, which m ay vary great ly from one count ry t o anot her and not t ak e int o consider at ion r egional pr epar at ions and m anufact ur ed pr oduct s on t he dom est ic m ar ket .
Considering t hat m ore t han 95% of t he sodium int ake is excret ed in t he urine an d t h at diet ar y assessm ent s present m any operat ional problem s, 24- hour urine excret ion has been ut ilized as a m arker for daily sodium consum pt ion, despit e t he great variabilit y bet ween individuals. Thus, t here needs t o be caut ion regarding clinical and physiological int er pr et at ions based on a single evaluat ion. This problem can, how ever, be overcom e in populat ion- based st udies, giv en t hat t he ur inar y ex cr et ion of sodium is considered t o be a good indicat or for salt consum pt ion on a given day.9
The m aj or it y of st udies aim ing t o find an associat ion bet w een sodium consum pt ion and art erial hypert ension have ut ilized 24 - hour urinary excret ion of sodium as a daily m arker, and in m any such st udies a consist ent r elat ionship has been found. Ev idence of an associat ion bet w een sodium consum pt ion and hypert ension has also been report ed by t he I NTERSALT Group,1 1 especially w it h r egar d t o assessm ent s of t he differ ences in t he pr ev alence of ar t er ial hy per t ension t hat is associat ed w it h t he lev el of indust r ializat ion of t he populat ions st udied. West er n populat ions and t hose w it h high salt consum pt ion appear t o have t he highest percent ages of hypert ension, w hile rural or prim it ive populat ions t hat do not m ak e use of added salt pr esent low er pr ev alence or no cases of ar t er ial hy per t ension.1 1 How ever , over w eight and sedent ar y lifest yles pr esent in t hese populat ions m ay be significant confounding v ar iables. Ot her st udies hav e been conduct ed along t hese lines in sev er al populat ions, w it h t he obj ect iv e of pr ov ing t he hy pot hesis t hat high salt int ake in t he diet increases blood pr essur e lev els, independent of age and ot her fact or s, w hich t oday is w ell est ablished.
I n addit ion t o t he operat ional difficult ies in assessing sodium consum pt ion, t he quest ions relat ing t o sen sit iv it y t o sodium appear t o be difficult t o resolve when st udied in hum an beings. I n effect , som e individuals excret e larger quant it ies of sodium wit hout an increase in art erial pressure while it is t he opposit e for ot her s.6 The physiological r esponse t o incr eased sodium int ak e r esult s in t he r educt ion of t he act iv it y of t he r enin- angiot ensin- aldost er one syst em and an incr ease in t he r elease of at r ial nat r iur et ic pept ide. These sy st em s int er act w it h each ot her and w it h ot her sy st em s, as w ell as act ing in t he r educt ion of sy m pat het ic act iv it y dir ect ed t ow ar ds t he k idney s. The genet ic differ ences responsible for t hese different responses of t he hum an body are not yet w ell know n. I t w ould appear t o be difficult t o est ablish, a pr ior i, who would be in t he first or second group when large num bers of individuals in t he populat ion are st udied, especially w hen such populat ions are racially het erogeneous. Wit h regard t o t his quest ion, som e st udies have now given evidence t hat Negro individuals have gr eat er sensit iv it y t o sodium t han w hit es do.2 0
M ETHOD
Th e st udy design w as based on cr oss- sect ional r esear ch m et hodology and w as developed by m eans of surveying and analyzing socioeconom ic and healt h dat a in a probabilist ic sam ple of resident s from t he m unicipalit y of Vit ória, ES. The sam pling plan had t he obj ect ive of ensuring t hat t he research w ould be socioeconom ically , geogr aphically and dem ogr aphically r epr esent at iv e of t he r esident s of t his m unicipalit y. The r esident populat ion aged 25 t o 64 year s in t he cit y of Vit ór ia w as st udied. Accor ding t o t h e cen su s car ried out by Fundação I BGE in t he year 1996, t he resident populat ion of Vit ória was 265,874 inhabit ant s. The sam pling w as perform ed in four st ages: by dist rict , I BGE census sect or, draw ing lot s t o choose hom es, and draw ing lot s t o choose t he individual from each hom e. The sur vey w as conduct ed w it h j ust one r esident of t he hom e t hat w as dr aw n, w it hin t he age gr oup of t he st udy . The draw was carried out by m eans of a random izat ion m echanism . A select ion of 2,268 resident ial hom es locat ed in Vit ória was m ade and t hese w er e v isit ed. The indiv idual select ed at each of t hese hom es w as giv en ex planat ions of t he pur poses of t he r esear ch and inv it ed t o par t icipat e in t he st udy , aft er obt aining his or her consent . The proj ect received approval from t he Et hics Com m it t ee of t h e Biom edical Cent er of Universidade Federal do Espírit o Sant o ( UFES) .
The dat a collect ion w as car r ied out by int er v iew er s and t r ained t echnicians in t he y ear s 1999 and 2000, by m eans of quest ionnaires applied during visit s t o 2,200 individuals in t he select ed hom es. Dur ing t he hom e visit , t he par t icipant r eceived guidance and m at er ials for t he 12- hour urine collect ion covering t he period from 7 p.m . t o 7 a.m . of t he next day.
The select ed indiv iduals w er e ask ed t o at t end t he Car diov ascular I nv est igat ion Clinic of t he Universit y Hospit al for t est s t o be per for m ed on t he follow ing day . Of t he t ot al sam ple, 1,663 indiv iduals at t ended. As w ell as handing in t he 12- hour urine collect ed during t he preceding night , art erial pressure w as m easured, a quest ionna ir e w as com plet ed r egar ding diet ar y and lifest yle habit s, blood w as collect ed and ot her t est s w er e per for m ed w it h t he aim of det er m ining t he car diov ascular r isk . The quant ificat ion of sodium and pot assium in m m ol/ L was done by m eans of flam e spect rophot om e t r y , using com m ercial kit s. The values found in t he urine sam ples were convert ed int o 12 - hour urine elect r oly t e quant it ies. The daily quant it y of sodium w as est im at ed by m eans of t he equat ion Na+24h = 1.7Na+12h+ 49.8 ( r= 0.88, p< 0.01) , which was derived from t he v alidat ion st udy on 50 norm ot ensive individuals.1 5
The salt consum pt ion w as init ially est im at ed fr om calculat ion of t he 24 - hour sodium excret ion, assum ing t hat all t he sodium int ake had been in t he form of NaCl. The consum pt ion was also est im at ed from t he quant it y of salt consum ed very m ont h in t he hom e ( according t o inform at ion collect ed v ia t he quest ionnair e) . These dat a w er e cor r ect ed for t he num ber of people w ho had m eals in t he hom e. The Na/ K r at io w as calculat ed fr om t he quant it ies of t hese elect r oly t es in t he 12- hour urine and was ut ilized as a m arker for t he diet ary qualit y.
SAP of gr eat er t ha n or equal t o 140 m m Hg and/ or DAP of great er t han or equal t o 90 m m Hg, or furt herm ore t hose using ant ihypert ensive m edicat ions, are ident ified as hypert ensive.
The indiv iduals w er e classified int o fiv e socioeconom ic classes, on t he basis of dat a on t he edu cat ion level of t he head of t he fam ily and t he t ype and quant it y of dom est ic equipm ent in t he hom e ( Fundação I BGE) .1 0
The com par ison of av er ages bet w een t he sex es w as done by m eans of t he St udent t t est for independent sam ples. For t he ot her variables ( socioeconom ic class, r ace and pr essur e st ages) , one -w ay v ar iance analy sis ( ANOVA) -w as ut ilized, follo-w ed by t he Tuk ey t est. The degr ee of associat ion bet w een v ar iables w as found by m eans of t he Pear son cor r elat ion coefficient ( r ) . The sim ple and part ial aged- cont r olled cor r elat ions bet w een SAP, DAP and MAP and t he 12- hour urinary Na and K ex cr et ion and t he ur inar y Na/ K r at io w er e also calculat ed. For analy sis of t he dat a, t he SPSS pr ogr am for Windows ( version 10.0.1) was ut ilized.
RESULT S
The sam ple st udied consist ed of 764 m en ( 45.9% ) and 899 w om en ( 54.1% ) . These per cent ages ar e close t o t he dist ribut ion by sex for t he 143,539 inhabit ant s of Vit ória ( 46.2 and 53.8% ) wit hin t he 25 -64 y ear age gr oup, accor ding t o t he 2000 census.1 0
Wit h regard t o socioeconom i c class, 10.9% were in class A, 27.5% in B, 29.4% in C, 28.4% in D and 3.8% in E.
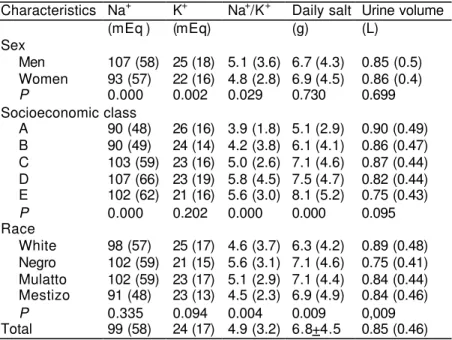
Table 1 pr esent s t he aver ages and st andar d deviat ions of t he var iables st udied and t he ur ine volum e, accor ding t o sex , socioeconom ic class and r ace. Significant differ ences were found in Na+12h and Na/ K bet w een t he sex es and socioeconom ic classes (P< 0.05) . The Na/ K rat io and urine volum e were lower am ong individuals of Negro race (P< 0.05) . No significant difference bet w een Na+12h and race w as found ( F= 1.13) .
Table 1 – Average and standard deviation of the measurements and nutritional indicators of the sample studied, according to sex, socioeconomic class and race.
Characteristics Na+ K+ Na+/K+ Daily salt Urine volume
(mEq ) (mEq) (g) (L)
Sex
Men 107 (58) 25 (18) 5.1 (3.6) 6.7 (4.3) 0.85 (0.5) Women 93 (57) 22 (16) 4.8 (2.8) 6.9 (4.5) 0.86 (0.4)
P 0.000 0.002 0.029 0.730 0.699
Socioeconomic class
A 90 (48) 26 (16) 3.9 (1.8) 5.1 (2.9) 0.90 (0.49) B 90 (49) 24 (14) 4.2 (3.8) 6.1 (4.1) 0.86 (0.47) C 103 (59) 23 (16) 5.0 (2.6) 7.1 (4.6) 0.87 (0.44) D 107 (66) 23 (19) 5.8 (4.5) 7.5 (4.7) 0.82 (0.44) E 102 (62) 21 (16) 5.6 (3.0) 8.1 (5.2) 0.75 (0.43)
P 0.000 0.202 0.000 0.000 0.095
Race
White 98 (57) 25 (17) 4.6 (3.7) 6.3 (4.2) 0.89 (0.48) Negro 102 (59) 21 (15) 5.6 (3.1) 7.1 (4.6) 0.75 (0.41) Mulatto 102 (59) 23 (17) 5.1 (2.9) 7.1 (4.4) 0.84 (0.44) Mestizo 91 (48) 23 (13) 4.5 (2.3) 6.9 (4.9) 0.84 (0.46)
P 0.335 0.094 0.004 0.009 0,009
Na+ 12h: 12-hour urinary sodium excretion; K+ 12h: 12-hour urinary potassium excretion; Na+/K+: ratio of 12-hour urinary sodium excretion to 12-hour urinary potassium excretion; daily salt: daily salt intake divided by number of persons.
The figures represent averages with standard deviations.
Taking int o consider at ion t hat no differ ence in ur ine volum e w as found bet w een t he sexes and socioeconom ic classes, it can be infer r ed t hat t he qualit y of t he m easur em ent s w as sat isfact or y and t hat st udy of t he elem en t s Na+ an d K+ in 12- hour urine provides reliable m arkers for t he consum pt ion of t hese elect r oly t es. Ten indiv iduals ( 0.6% ) of t he sam ple at t ended t he clinic but did not hand in t he 12- hour urine collect ion. I t is probable t hat som e of t he individuals originally select ed in t he household sam pling did not som e for t he t est s in t he clinic because t hey had not done t he ur ine collect ion over t he preceding night . Am ong t hose w ho did hand in t he urine, 0.4% report ed t hat t hey had not done t he collect ion in accor dance w it h t he prot ocol and w ere excluded from t he sam ple.
Wit h regard t o t he consum pt ion variables, w hich are indicat ed as average and st andard deviat ion in Table 2, only t he quant it y of sodium ex cr et ed in t he 12- hour urine increased progressively wit h t he art erial pressure class. I ndividuals in t he “ excellent ” art erial pressure class ( SAP < 120 and DAP < 80 ) pr esent ed t he low est 12 - hour urinary sodium excret ion ( 86± 57 m Eq) , and t his value was significant ly lower t han what was found in t he “ norm al” ( 94± 48 m Eq, P< 0.05), “ high norm al” (102± 54 m Eq,
P< 0.001) , st age 1 ( 109± 61 m Eq) , st age 2 ( 110± 63 m Eq, P< 0.001) and st age 3 ( 120± 65 m Eq,
P< 0.05) art erial pressure classes. The sodium / pot assium rat io was also lowest in t he “ excellent ” art erial pressure class ( 4.5± 2.7) and significant ly different from t he st ages 1 ( 5.2± 2.9, P< 0.05) and 3 ( 5.9± 3.2, P< 0.05) . No significant differences w ere found in t he 12 - hour urinary pot assium excret ion and daily salt consum pt ion bet w een t he ar t er ial pr essur e st ages. The salt consum pt ion est im at ed from t he 12 - hour urinary sodium excret ion followed t he sam e t rend as t he 12- hour sodium values.
Table 2 – Averages and standard deviations for the consumption variables, according to the arterial pressure stages. Arterial pressure stages* Consumption variables
Na+ 12h K+ 12h Na+/K+ Daily salt Estimated salt
(mEq) (mEq) (g) (g)
Excellent 86 (57) 22 (18) 4.5 (2.7) 6.5 (4.0) 11.2 (5.6) Normal 94 (48)*** 23 (17) 4.8 (4.3)* 6.4 (4.0) 12.0 (4.8)*** High normal 102 (54)*** 24 (15) 5.0 (3.1)* 6.9 (4.5) 12.7 (5.3)*** Stage 1 109 (61)*** 24 (14) 5.2 (2.9)* 7.2 (4.5) 13.4 (6.0)*** Stage 2 110 (63)*** 26 (20) 4.9 (2.7)* 7.3 (3.7) 13.5 (6.2)*** Stage 3 120 (65)*** 24 (16) 5.9 (3.2)* 7.2 (4.5) 14.4 (6.4)***
P 0.000 0.171 0.001 0.134 0.000
SAP: systolic arterial pressure; DAP: diastolic arterial pressure
*Excellent: SAP<120 and DAP<80; normal: SAP<130 and PAD<85; high normal: SAP between 130 and 139 or DAP between 85 and 89; stage 1: SAP between 140 and 159 or DAP between 90 and 99; stage 2: SAP between 160 and 179 or DAP between 100 and 109; stage 3: SAP>180 or DAP>110; Na+ 12h, 12-hour urinary sodium excretion; K+ 12h, 12-hour urinary potassium excretion; Na+/K+, sodium/potassium ratio; daily salt, daily quantity of salt consumed per person; estimated salt, estimated consumption of salt from 12-hour urinary sodium excretion.
*P<0.05, vs. excellent pressure stage.
***P<0.001
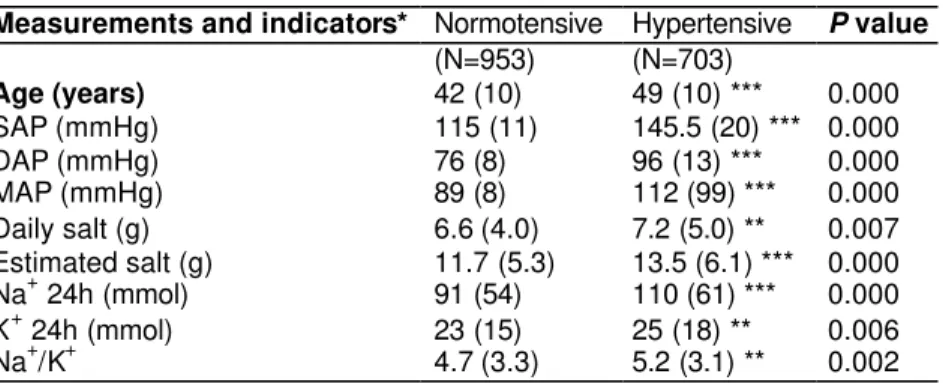
Table 3 pr esent s t he av er ages and st andar d dev iat ions for t he hem odynam ic m easurem ent s and var iable st udied, accor ding t o t he classificat ion of t he individuals as hyper t ensive or nor m ot ensive. All t he m easurem ent s for t he individuals classified as hypert ensive differ from t hose of t he group classified as nor m ot ensiv e. When only t w o groups w ere ut ilized for classifying t he individuals, m easurem ent s t hat previously did not differ from one group t o anot her, such as daily salt consum pt ion, becam e st at ist ically differ ent in t his sit uat ion ( hy per t ensiv e: 7.2± 5.0 g, nor m ot ensiv e: 6.6± 4.0 g, P< 0.05).
Table 3 – Averages and standard deviations of the hemodynamic measurements and consumption variables for the sample studied, according to the classification of individuals as hypertensive or normotensive.
Measurements and indicators* Normotensive Hypertensive P value (N=953) (N=703)
Age (years) 42 (10) 49 (10) *** 0.000
SAP (mmHg) 115 (11) 145.5 (20) *** 0.000
DAP (mmHg) 76 (8) 96 (13) *** 0.000
MAP (mmHg) 89 (8) 112 (99) *** 0.000
Daily salt (g) 6.6 (4.0) 7.2 (5.0) ** 0.007 Estimated salt (g) 11.7 (5.3) 13.5 (6.1) *** 0.000 Na+ 24h (mmol) 91 (54) 110 (61) *** 0.000
K+ 24h (mmol) 23 (15) 25 (18) ** 0.006
Na+/K+ 4.7 (3.3) 5.2 (3.1) ** 0.002
*SAP: systolic arterial pressure; DAP: diastolic arterial pressure; MAP: mean arterial pressure; Na+ 12h, 12- hour urinary sodium excret ion; K+ 12h, 12 - hour urinary pot assium excret ion; Na+/ K+, sodium / pot assium r at io; daily salt , daily quant it y of salt consum ed per per son; est im at ed salt , est im at ed consum pt ion of salt from 12- hour ur inary sodium excret ion.
The dat a ar e pr esent ed as av er ages ( w it h st andar d dev iat ion) .
**P<0.01, vs. normotensive.
***P<0.001.
Table 4 pr esent s t he r esult s fr om t he cor r elat ion analy sis, befor e and aft er age- cont r ol, bet w een t he hem odynam ic m easurem ent s and t he var iables st udied. I t w as obser ved t hat only t he var iables Na+12h and Na/ K cont inued t o have a correlat ion w it h SAP, DAP and MAP.
Hemodynamic measurements Variables
SAP DAP MAP
Na+ 12h
before 0.15*** 0.19*** 0.18*** after 0.14*** 0.19*** 0.18*** K+ 12h
before 0.06* 0.05* 0.07** after 0.03 0.04 0.03 Na+/K+
before 0.07* 0.12*** 0.10*** after 0.10*** 0.14*** 0,13***
Daily salt
before 0.05 0.06* 0.06* after 0.04 0.05 0.05
SAP: systolic arterial pressure; DAP: diastolic arterial pressure; MAP: mean arterial pressure; Na+ 12h, 12-hour urinary sodium excretion; K+ 12h, 12-hour urinary potassium excretion; Na+/K+, sodium/potassium ratio; daily salt, daily quantity of salt consumed per person. The hemodynamic measurements were correlated with the consumption variables before and after age-control.
*P<0.05; **P<0.01; ***P<0.001.
Posit ive linear c orrelat ions were observed bet ween urinary sodium excret ion and SAP ( r= 0.15,
Figure – Linear regression of systolic arterial pressure (SAP) and diastolic arterial pressure (DAP) as a function of urinary sodium excretion and the sodium/potassium ratio.
DI SCUSSI ON
Differing from ot her populat ion st udies perform ed in Brazil, a large proport ion of t he individuals in higher social classes w elcom ed t he int er v iew er s int o t heir hom es and agr eed t o par t icipat e in t he st udy. This w as probably due t o publicit y t hrough t he m edia t hat w as given before and during t he fieldwork. However, one lim it at ion of t he st udy was t he low ret urn from individuals of class E. There w as also a low er proport ion of younger individuals at t ending t he clinic for t est s t o be per for m ed, and t he aver age age for t he gr oup st udied w as ar ound 45 year s. The per cent age of young individuals wit hin t he sam ple was lower t han found wit hin t he general populat ion of Vit ória, which m ay be consider ed t o be a lim it at ion.
The quant it y of daily added salt report ed w as 6.8± 4.5 g, t hus corresponding t o 52.3% of t he consum p t ion est im at ed from urinary sodium excret ion. However, t he added- salt m et hod does not t ak e int o account t he salt int ak e fr om nat ur al foods and m anufact ur ed pr oduct s. Alt hough t he est im at ed consum pt ion of added salt w as low er in class E t han in classes C and D, class E pr esent ed higher added- salt consum pt ion t han for t he ot her classes, pr obably due t o low er use of m anufact ur ed foods and ov er all quant it y of food eat en. This fact m ay , how ev er , be r elat iv e, since class E is less represent ed in t he sam ple. Anot her m at t er t hat can be highlight ed is t hat t he low er socioeconom ic classes pr obably have easier r ecollect ion of w hat quant it ies of food w er e consum ed in t he hom e.
High salt consum pt ion is t oday ut ilized as a pr edict or for car diov ascular diseases. I n West er n count ries, salt consum pt ion is high, not only in food preparat ion but also in food conservat ion. Ot her subst ances like m onosodium glut am at e are also great ly ut ilized in t his. Salt appears t o have great accept ance am ong t he y oung and has becom e indispensable in dough- based foods. Despit e t he few st udies on changes in diet ary st andards in Brazil, t he st udy by Barret o & Cyrillo,2 in t he cit y of São Paulo, show ed t hat t her e has been a r educt ion of 35% in dom est ic expendit ur e on fr uit and veget ables in t he fam i ly budget . The opposit e sit uat ion has been found for ex pendit ur e on m anufact ur ed foods. I t appear s t hat t his m odificat ion is not only r elat ed t o m ar ket pr ices but also m arket ing and t he dynam ics of life, which have an im port ant role in consum er decisions.
The st udy m ade by Tian et al1 9 in a Chinese populat ion ut ilizing t he diet ary m et hod ( t hree 24- hour records) ident ified consum pt ion of approxim at ely 6 g of sodium am ong t he urban populat ion, wit h 53% probably com ing from added salt , 17% from m anufact ured f oods, 16% from soybean- based sauces and 6% from m onosodium glut am at e. Cereal and veget ables w ere t he great est sources of pot assium in t he food. That st udy also suggest ed t he need for r educing sodium int ake, especially in relat ion t o salt added in t he prepa r at ion of m eals. This can be achieved by m eans of populat ion- based st r at egies aim ed at t he cont r ol of ar t er ial hy per t ension w it hin all social classes.
A diet t hat is poor er in fr uit and v eget ables and based on m anufact ur ed foods t hat ar e r icher in fat s and salt appear s t o be a pr edict or for healt h pr oblem s, par t icular ly t hose due t o pr essur e levels. I t is wit hin t his cont ext t hat t he sodium / pot assium rat io has been ut ilized a m arker for diet ary qualit y, given t hat a m ore adequat e diet in relat ion t o sodium and pot assium m ay be relat ed t o great er consum pt ion of fr uit and veget ables and low er consum pt ion of m anufact ur ed foods such as pr ocessed and canned foods. Som e st udies have dem onst rat ed t hat t his rat io is m ore im port ant t han separat e m easurem ent s of sodium and potassium .1 3 The st udy m ade by Kaufm ann et al1 2 in Afr ica show ed t hat t his r at io w as associat ed w it h t he sy st olic and diast olic ar t er ial pr essur es and t hat incr eased pr ev alence of hy per t ension w as associat ed bot h w it h econom ic and diet ar y changes. In t he pr esent st udy, salt consum pt ion and t he Na/ K rat io had a posit ive associat ion w it h increased pressure levels. I ndividuals in class A, wom en, whit es and m ixed - race individuals present ed lower Na/ K rat ios, independent of any increases in pot assium , and it can be infer r ed t hat t hese gr oups pr esent diet s t hat ar e m or e adequat e t han for ot her gr oups. This associat ion appear s t o be r esult ant fr om t he socioeconom ic class. High sodium consum pt ion m ay also be relat ed t o great er int ake of prepared foods w it h r e ady seasoning, w hich ar e v er y accessible for t he less fav or ed socioeconom ic classes. This relat ionship was also higher am ong Negroes. However, t heir salt int ake est im at ed from sodium ex cr et ion did not differ st at ist ically fr om t hat of ot her gr oups. This r esult m ay be r elat ed t o gr eat er sensit ivit y t o sodium present am ong individuals of Negro race, which m ay be linked t o t he lower urinary sodium excret ion found in t his group.
such consum pt ion. I n t he pr esent st udy, differ ences in daily salt consum pt ion w er e obser ved, w it h individuals in class A and w hit es present ing t he low est daily consum pt ion.
Result s from m et a- analyses ar e consist ent in dem onst r at ing t hat sodium r educt ion has a sm all but significant effect on ar t er ial pr essur e,4 especially am ong elderly individuals and t hose who present higher art erial pressure.1 Cappuccio3 em phasized t he need for m oderat e salt r educt ion in t he diet and incr ease in foods r ich in pot assium , not only as a fir st st ep in t he t r eat m ent of individuals w it h hy per t ension, but also especially as a pr ev ent iv e m easur e for r educing t he pr ev alence of ar t er ial hypert ension and it s com plic at ions w it hin t he populat ion.
A m ore balanced and healt hier diet ary pat t ern m ust be encouraged so as t o prom ot e changes in t he populat ion’s ant hropom et ric profile over t he long t erm t hat are m ore consist ent . There is now epidem iological evidence t hat im prov em ent in t he diet has a gr eat pot ent ial for pr ev ent ing t oday ’s illnesses.
REFEREN CES
1. Alderm an MH. Salt , blood pressure, and hum an healt h. Hy per t ension 2000; 36: 890- 3.
2. Barret t o SAJ, Cyrillo DC. Análise da com posição dos gast os com alim ent ação no m unicípio de São Paulo ( Brasil) na década de 1990. Rev Saúde Pública 2001; 35: 52 - 9.
3. Cappuccio FP. Diet ar y changes and t heir effect on blood pr essur e: w hat lesson should w e lear n? J Hum Hypert ens 1997; 11: 765- 6 .
4. Chobanian AV, Hill M. Nat ional heart , lung, and blood I nst it ut e Workshop on sodium and blood pr essur e. Hy per t ension 2000; 35: 858- 63.
5. Consenso Brasileiro de Hipert ensão Art erial - I I I Consenso Brasileiro de Hipert ensão Art erial – 1998. Available at URL: ht t p: / / depar t am ent os.car diol.br / dha/ publicacoes/ consenso3/ consen.asp [ 2000, Sep 20] .
6. Cow ley AW. Genet ic and nongenet ic det er m inant s of salt sensibilit y and blood pressure. Am J Clin Nu t r 1997; 6( Suppl) : 587S- 93S.
7. Espeland MA, Kum anyika S, Wilson AC, Reboussin DM, East er L, Self M et al. St at ist ical issues in analyzing 24- hours diet ary recall and 24 - hours urine collect ion dat a for sodium and pot assium int ak es. Am J Epidem iol 2001; 153: 996- 1006.
8. Freit as OC, Carvalho FR, Neves JM, Veludo PK, Parreira RS, Gonçalves RM et al. Pr ev alence of Hypert ension in t he urban populat ion of Cat anduva, in t he st at e of São Paulo, Brazil. Ar q Br as Car diol
9. Fr ost CD, Law MR, Wald NJ. By how m uch does diet ar y salt r educt ion low er blood pr essur e? I I - Analysis of observat ional dat a w it hin populat ions. BMJ 1991; 302: 815 - 8 .
10. Fundação I nst it ut o Br asileir o de Geogr afia e Est at íst ica. Pesquisa por am ost r a de dom icílios 2000: m icr odados. Rio de Janeiro; 2001.
11. I nt er salt Cooper at ive Resear ch Gr oup. An int er nat ional st udy of elect r olyt e excr et ion and blood pressure: result s for 24- hour urinary sodium and pot assium excret ion. BMJ 1988; 297: 319 - 28.
12. Kaufm ann EE, Owoaj e SA, Jam es SA, Rot ini CN, Cooper RS. Det erm inant s of hypert ension in West Afr ica: cont r ibut ion of ant hr opom et r ic and diet ar y fact or s t o ur ban- rural and socioeconom ic gradient s.
Am J Epidem iol 1992; 143: 1203 - 18.
13. Kot chen TA, Kot chen JM. Diet ar y sodium and blood pressure: int eract ions wit h ot her nut rient s.
Am J Clin Nut r 1997; 65( Suppl) : 708S- 11S.
14. MacMahon S, Pet o R, Cut ler J. Blood pr essur e, st r ok e and cor onar y hear t disease: effect s of prolonged differences in blood pressure- evidence from nine pr ospect iv e obser v at ional st udies cor r ect ed for dilut ion bias. Lancet 1995; 335: 765- 74.
15. Molina, MCB. Hipert ensão art erial e fat ores nut ricionais: um est udo de base populacional no m unicípio de Vit ória/ ES [ Doct oral t hesis] . Vit ória: Universidade Federal do Espír it o Sant o; 2002.
16. Pearson TA, Blair SN, Daniels SR, Eckel RH, Fair JM, Fort m ann SP et al. AHA Guidelines for prim ary prevent ion of cardiovascular disease and st roke: 2002 updat e. Cir culat ion 2002; 106: 388- 91.
17. Sacks FM, Svet key LP, Vollm er WM, Appel LJ, Bray GA, Harsha D et al. Effect s on blood pressure of reduced diet ary sodium and t he Diet ary Approaches t o St op Hypert ension ( DASH) diet . N Engl J Med 2001; 344: 3 - 10.
18. The sixt h r epor t of t he Joint Nat ional on Pr event ion, Det ect ion, and Tr ea t m ent of High Blood Pressure ( JOI NT VI ) . Ar ch I nt Med 1997; 157: 2413 - 46.
19. Tian HG, Hu G, Dong QN, Yang XL, Nan Y, Piet inen P et al. Diet ary sodium and pot assium , socioeconom ic st at us and blood pressure in a Chinese populat ion. Appet it e 1996; 26: 235 - 46.
20. Weinberger MH. Salt sensibilit y of blood pressure in hum ans. Hy per t ension 1996; 27: 481- 90.
21. Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: part I : general consider at ions, t he epidem iological t r ansit ion, r isk fact or s, and im pact of urbanizat ion. Cir culat ion
2001; 27: 2746- 53.
Address to correspondence
Maria del Carm en Bisi Molina
Depart am ent o de Enferm agem , Cent ro Biom édico da Universidade Federal do Espírit o Sant o Av. Marechal Cam pos s/ nº
29040 - 090 Vit ória, ES
E- m ail: m dcarm [email protected] .br
Sour ce of funding:
Supported by
t he Conselho Nacional de Desenvolvim ent o Cient ífico e Tecnológico ( CNPq – grant no. 521148/ 97 - 6 ) an d Facit ec ( Fundo de Apoio à Ciência e à Tecnologia) / Vit ór ia Cit y Aut hor it yBased on doct or al t hesis pr esent ed w it hin t he post gr aduat e pr ogr am in Phy siological Sciences of Universidade Federal do Espírit o Sant o, 2002.
Received on 5/ 8/ 2002. Review ed on 6/ 6/ 2003. Approved on 10/ 6/ 2003.
© 2 0 0 3 Fa cu lda de de Sa ú de Pú blica da U n iv e r sida de de Sã o Pa u lo
Ave nida D r . Ar na ldo, 7 1 5 0 1 2 4 6 - 9 0 4 Sã o Pa ulo SP Br a zil
Te l./ Fa x : + 5 5 1 1 3 0 6 8 - 0 5 3 9