Outcome of Platinum-Based Chemotherapy for
Non-Small Cell Lung Cancer Patients: A Meta-Analysis of 24
Studies
Qin Qin1., Chi Zhang1., Xi Yang1., Hongcheng Zhu1
, Baixia Yang2, Jing Cai2, Hongyan Cheng3, Jianxin Ma4, Jing Lu1, Liangliang Zhan1, Jia Liu1, Zheming Liu1, Liping Xu1, Xinchen Sun1*
1Department of Radiation Oncology, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, China,2Department of Radiation Oncology, Nantong Tumor Hospital, Nantong, Jiangsu Province, China,3Department of Geriatric Medicine, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, China,4Department of Radiation Oncology, the No. 2 People’s Hospital of Lian Yungang, Lian Yungang, Jiangsu Province, China
Abstract
Objective: Xeroderma pigmentosum group D(XPD) is an essential gene involved in the nucleotide excision repair (NER) pathway. Two commonly studied single nucleotide polymorphisms (SNPs) ofXPD(Lys751Gln, A.C, rs13181; Asp312Asn, G.A, rs1799793) are implicated in the modulation of DNA repair capacity, thus related to the responses to platinum-based chemotherapy. Here we performed a meta-analysis to better evaluate the association between the twoXPDSNPs and clinical outcome of platinum-based chemotherapy in non-small cell lung cancer (NSCLC) patients.
Methods:A comprehensive search of PubMed database was conducted to identify relevant articles. Primary outcomes included objective response (i.e., complete response + partial response vs. stable disease + progressive disease), progression-free survival (PFS) and overall survival (OS). The pooled and 95% confidence intervals (CIs) of ORs (odds ratios) and HRs (hazard ratios) were estimated using the fixed or random effect model.
Results: Twenty-four studies were eligible according to the inclusion criteria. None of the XPDLys751Gln/Asp312Asn polymorphisms was associated with objective response, PFS or OS in NSCLC patients treated with platinum drugs. However, in stratified analysis by ethnicity, theXPDLys751Gln (A.C) polymorphism was not significantly associated with increased response in Caucasians (OR = 1.35, 95%CI = 1.0–1.83,P= 0.122 for heterogeneity) but was associated with decreased PFS in Asians (HR = 1.39, 95%CI = 1.07–1.81,P= 0.879 for heterogeneity). Furthermore, a statistically significant difference existed in the estimates of effect between the two ethnicities (P= 0.014 for TR;P,0.001 for PFS).
Conclusions:XPDLys751Gln (A.C) may have inverse predictive and prognostic role in platinum-based treatment of NSCLC according to different ethnicities. Further studies are needed to validate our findings.
Citation:Qin Q, Zhang C, Yang X, Zhu H, Yang B, et al. (2013) Polymorphisms inXPDGene Could Predict Clinical Outcome of Platinum-Based Chemotherapy for Non-Small Cell Lung Cancer Patients: A Meta-Analysis of 24 Studies. PLoS ONE 8(11): e79864. doi:10.1371/journal.pone.0079864
Editor:Xiaoping Miao, MOE Key Laboratory of Environment and Health, School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, China
ReceivedAugust 22, 2013;AcceptedSeptember 25, 2013;PublishedNovember 15, 2013
Copyright:ß2013 Qin et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding:This work was supported by the Natural Science Foundation of China (Grant No. 81272504), the Innovation Team (NO. LJ201123), and Jiangsu Provincial Natural Science Fund (BK2011854), and ‘‘333’’ Project of Jiangsu Province (BRA2012210 (RS12)). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests:The authors have declared that no competing interests exist. * E-mail: [email protected]
.These authors contributed equally to this work.
Introduction
Lung cancer remains the most frequent human malignancy worldwide and represents a leading cause of cancer related death with only 15% of patients surviving five years or more [1]. Non-small cell lung cancer (NSCLC) accounts for approximately 80% of primary lung cancer and most patients have suffered from advanced disease at the time of diagnosis [2]. Currently, the standard chemotherapeutic regimen for the treatment of advanced NSCLC patients is based on the combination of platinum compounds and a third-generation cytotoxic agent [3]. However,
could predict the risk of lung cancer and the response of patients to platinum based chemotherapy.
Platinum agents exert anti-cancer activity mainly through the formation of DNA adducts, which inhibit DNA replication and eventually hinder cell division [9].
Nucleotide excision repair (NER) is a predominant pathway responsible for removing platinum-induced DNA lesions [10]. Thus the modification of NER pathway may have impact on tumor sensitivity to platinum based chemotherapy, and conse-quently influence clinical outcome and patient survival [11–13]. The xeroderma pigmentosum group D (XPD, also named excision reair cross-complementing group 2, ERCC2) gene encodes for an ATP-dependent DNA helicase, a subunit of the basal transcription factor II H (TFII H) which mediates DNA unwinding for the initiation of NER [14].XPDAsp312Asn and Lys751Gln are two common nonsynonymous single nucleotide polymorphisms (SNPs) in coding region of XPD gene and have been associated with impaired DNA repair capacity [12,15,16]. In recent years, a great number of molecular epidemiological studies have investigated the relationship of XPD polymorphisms with treatment response in NSCLC. While a possible role of the two SNPs as the predictor of response in advanced NSCLC is indicated, the results available in individual literature are inconsistent [17,18]. Thus, we performed this meta-analysis to evaluate the effects of XPD Asp312Asn (G.A) and Lys751Gln (A.C) polymorphisms on the efficacy of platinum-based chemotherapy in advanced NSCLC by assessing therapeutic response (TR), progression-free survival, and overall survival.
Materials and Methods
Search strategy and study selection
The identification of potentially relevant studies was performed through a search in electronic database PubMed using the following terms ‘‘XPD or ERCC2’’ and ‘‘lung neoplasm or
non-small cell lung cancer’’ and ‘‘prognosis or outcome or survival or efficacy or response’’. The latest search was updated on August 20, 2013. Bibliographies of eligible studies, review articles and other relevant publications were also reviewed to identify all potential studies.
Articles published in English peer-reviewed journals that provided outcome data stratified by XPD polymorphic variants were included. The detailed eligible criteria were as follows: (1) patients with histologically or pathologically confirmed advanced, recurrent, or metastatic NSCLC; (2) the patients were treated with platinum-based chemotherapy; (3) XPD Lys751Gln (rs13181) or Asp312Asn (rs1799793) single nucleotide polymorphism was genotyped; (4) studies provided primary outcomes of interest including objective response, progression-free survival or overall survival. The studies were excluded from the analysis if any of the cases occurred: (a) platinum-based chemotherapy was used as neoadjuvant treatment; (b) critical information was missing or could not be obtained by our repeated requests.
Data extraction
Two investigators (Qin Qin and Chi Zhang) independently screened the studies and extracted the data from included studies by using standard data-abstraction forms. Disagreements were resolved through discussion with another investigator (Hongcheng Zhu). For each study, the following characteristics and information were collected: name of the first author, year of publication, country of origin, ethnicity, the number of enrolled patients, treatment protocol, clinical stage, outcome, and SNPs included in each study. In addition, response to chemotherapy according to genotypes, hazard ratios (HRs) for OS and PFS, and their 95% confidence intervals (CIs) were collected for statistical analysis. If a direct report of HR and 95% CI was not available [19], estimated value was derived indirectly from Kaplan-Meier curves using the methods described by Tierney et al. [20]. Survival rates on Kaplan-Meier curves were read by Engauge Digitizer version 4.1
(http://digitizer.sourceforge.net/), then the data read from Kaplan-Meier curves were entered in the calculation spreadsheet appended to Tierney’s paper.
Statistical methods
The odds ratio (OR) with its 95% CI were estimated to show the strength of the association between XPD polymorphism and objective response [CR (complete response) +PR (partial re-sponse)] in each study. Response to chemotherapy was assessed with RECIST [21] (Response Evaluation Criteria in Solid Tumors) criteria or WHO criteria every 2 or 3 treatment cycles. Stata SE 11.0 software was used to obtain pooled statistics for HRs of survival or ORs of chemotherapy response. The statistical significance of the pooled estimates was examined by Z test. The initial analyses were performed with a fixed effect model assuming homogeneity of the individual HRs. The assumption was tested by
performing Cochran Q-test for heterogeneity. The effect of heterogeneity was tested by performing I2 test. A significant Q-test (P,0.05) orI2.50% indicated the heterogeneity among the studies, and the random-effect model was applied for meta-analysis.
Sub-group analyses were performed according to ethnicities. The differences in the effect estimates between subgroups were compared as described by Altmanet al. [22]. Begger’s funnel plots and the Egger’s linear regression tests were used to evaluate the potential publication bias. All P values were 2-sided, and all analyses were carried out with Stata SE 11.0 software package.
Results
A total of 61 related papers were identified by initial screening (as of August 20, 2013), and 28 reports were identified after further Table 1.Studies included in this meta-analysis.
Study Year Country Ethnicity Drug Case N Stage Outcome SNPs of XPD HWE
Cheng et al.[29] 2013 China Asian Platinum-based 115 IIIB-IV OS/PFS Lys751Gln 0.76 Li et al.[30] 2013 China Asian Platinum-based 496 IIIA- IV TR/OS/PFS Lys751Gln and
Asp312Asn
-Chen et al.[31] 2012 China Asian Platinum-based 355 IIIB- IV TR Lys751Gln .0.05
Li et al.[32] 2012 China Asian Platinum-based 89 IIIA- IV TR Lys751Gln 0.53
Liao et al.[33] 2012 China Asian Gemcimtabine+platinum 62 IIIB- IV TR/OS Lys751Gln and Asp312Asn
0.74/0.89
Provencio et al.[34] 2012 Spain Caucasian Vinorelbine+cisplatin 180 IIIB- IV TR/PFS Lys751Gln and Asp312Asn
,0.05/0.48
Wu et al.[35] 2012 China Asian Platinum-based 353 IIIA- IV TR/OS Lys751Gln and Asp312Asn
.0.05
Ren et al.[36] 2012 China Asian Platinum-based 340 IIIB- IV OS Lys751Gln .0.05
Zhang et al.[37] 2012 China Asian Gemcimtabine+cisplatin 632 I- IV OS Lys751Gln and Asp312Asn
0.83/0.58
Ludovini et al.[38] 2011 Italy Caucasian Cisplatin+gemcimtabine/ taxol/vinorelbine
192 IIIB- IV TR/OS/PFS Lys751Gln .0.05
Mathiaux et al.[19] 2011 France Caucasian Platinum-based 85 IIA- IV PFS Lys751Gln -Vi,nolas et al.[39] 2011 Spain Caucasian Cisplatin+vinorelbine 94 IIIB- IV TR/OS/PFS Lys751Gln and
Asp312Asn
0.07/0.19
Liu et al[40] 2011 China Asian Platinum-based 199 IIIA- IV OS/PFS Lys751Gln 0.22
Li et al.[41] 2010 China Asian Platinum-based 115 IIIB- IV TR Lys751Gln .0.05
Kalikaki et al.[42] 2009 Greece Caucasian Platinum-based 119 IIIA- IV TR/OS Lys751Gln and Asp312Asn
.0.05
Yao et al.[43] 2009 China Asian Platinum-based 108 IIIB- IV TR/OS Lys751Gln 0.28
Gandara et al.[44] 2009 USA Both Paclitaxel+carboplatin 381 IIIB- IV TR/OS/PFS Lys751Gln .0.05 Tibaldi et al.[18] 2008 Italy Caucasian Gemcitabine+cisplatin 65 IIIB- IV TR/OS/PFS Lys751Gln and
Asp312Asn
.0.05
Booton et al.[45] 2006 UK Caucasian Carboplatin+docetaxel 108 III- IV TR/OS Lys751Gln and Asp312Asn
0.89/0.39
Penas et al.[20] 2006 Spain Caucasian Gemcitabine+cisplatin 132 IIIB- IV OS/PFS Lys751Gln and Asp312Asn
.0.05
Isla et al.[17] 2004 Spain Caucasian Cisplatin+docetaxel 62 IIIB- IV TR/OS/PFS Lys751Gln and Asp312Asn
0.95
Ryu et al.[46] 2004 Korea Asian Cisplatin+paclitaxel/ docetaxel/ gemcimtabine
107 IIIB- IV TR Lys751Gln and Asp312Asn
0.54/0.69
Gurubhagavatula et al.[12]
2004 USA Caucasian Platinum-based 103 IIIA- IV OS Asp312Asn .0.05
Camps et al.[47] 2003 Spain Caucasian Gemcitabine+cisplatin 33 IIIB- IV TR Lys751Gln ,0.05
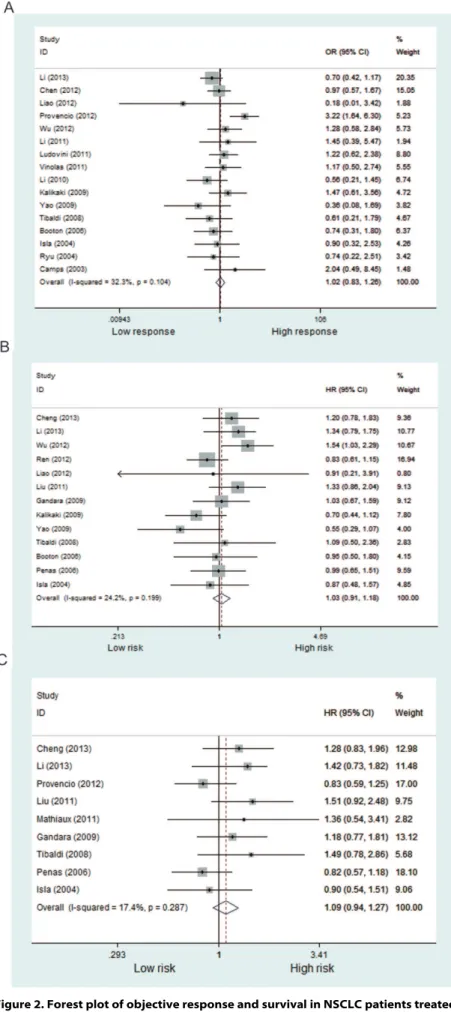
Figure 2. Forest plot of objective response and survival in NSCLC patients treated with platinum-based chemotherapy according to XPD Lys751Gln polymorphism (A/C+C/C vs. A/A).(A) objective response; (B) OS; (C) PFS.
examination. Two studies were excluded because all patients were not treated with platinum-based chemotherapy. Moreover, two studies were excluded from the analysis because the data were inestimable and the authors were unreachable. As a result, 24 studies including 4,468 NSCLC patients were eligible for inclusion in our meta-analysis. The process of selecting publications was presented in Fig. 1 and the characteristics of the included studies were listed in Table 1. A total of 17 studies including 2,919 patients reported the correlation between XPD polymorphisms and treatment response, 11 studies including 2,001 patients reported XPD polymorphisms and PFS, and 17 studies including 3,561 patients reported XPD polymorphisms and OS.
XPD Lys751Gln (rs13181A.C)
Objective response. Fifteen studies including 2,383 patients were qualified for analyzing the association between XPD
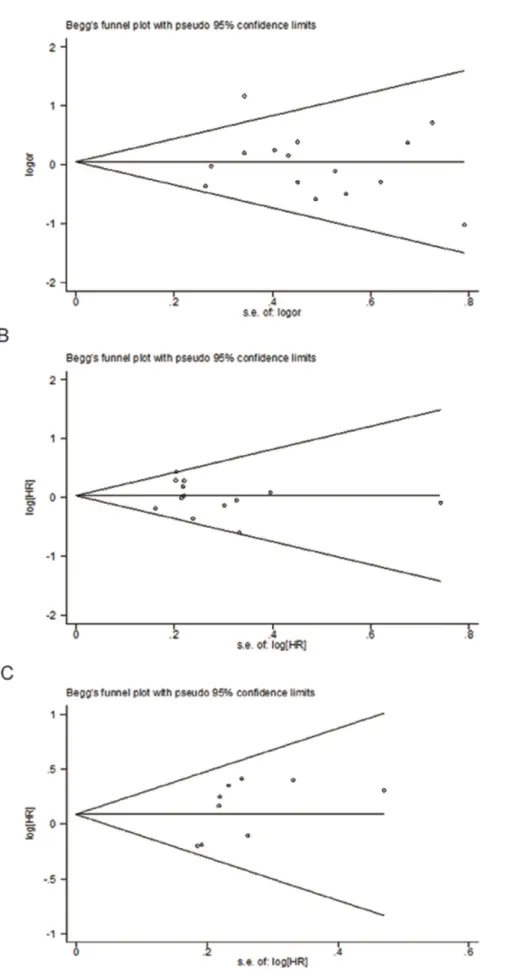
Lys751Gln polymorphism and TR in NSCLC patients. In the dominant model, the minor variant C was not associated with objective response in all patients (Table 2, Fig. 2). The ORs in homozygous and heterozygous models were similar to those in dominant model (Table 2). However, stratified analysis by ethnicity showed a significant difference in the estimates of effect between Caucasians and Asians in dominant model (P= 0.014). The C/C and A/C genotypes of XPD751 were borderline associated with favorable objective response in Caucasian patients treated with platinum-based regimen (C/C+A/C vs. A/A: OR = 1.35,P= 0.05; Fig. 3); while the variant allele appeared to show an inverse association in Asian patients (C/C+A/C vs. A/A: OR = 0.80, P= 0.129; Fig. 3). No publication bias was detected according to the results of funnel plot and the Egger’s test (C/ C+A/C vs. A/A:PBegg= 0.767;PEgger= 0.748; Fig. 4).
Overall survival. Data from 16 included studies (including 3,458 patients) were applicable for the analysis. As shown in Fig 2B, the variant genotype of XPD751 was associated with a nonsignificant increase of hazard for death in all patients (C/ C+A/C vs. A/A: HR = 1.03,P= 0.631; C/C vs. A/A: HR = 1.29,
P= 0.198; A/C vs. A/A: HR = 1.09,P= 0.369; Table 2). Likewise, stratified analysis by ethnicity showed no significant correlation between XPD Lys751Gln polymorphism and overall survival in Asian or Caucasian patient (Fig. 3). No publication bias was detected by either the funnel plot or Egger’s test (C/C+A/C vs. A/ A:PBegg= 0.246;PEgger= 0.512; Fig. 4).
Progression -free survival. A total of 11 studies (including 2,001 patients) were eligible for inclusion in the analysis. The pooled results showed no significant association between XPD
Lys751Gln polymorphism and PFS under either kinds of genetic model (Table 2, Fig. 2). Nevertheless, subgroup analysis by ethnicity showed a significant increase in the hazard of progression in Asian patients (C/C+A/C vs. A/A: HR = 1.39, P= 0.015; Fig 3). Further comparison indicated remarkably significant difference in the estimate of effect between Asian and Caucasian populations (P,0.001). No significant publication bias was detected by either the funnel plot or Egger’s test (C/C+A/C vs. A/A:PBegg= 0.118;PEgger= 0.131; Fig. 4).
XPD Asp312Asn (rs1799793G.A)
Objective response. Ten studies including 1,588 patients were eligible for the final analysis. Pooled data from all patients indicated that the variant A allele was not associated with objective response under either genetic model (Fig. 5; Table 2). In addition,
stratified analysis by ethnicity did not demonstrate significant difference (A/A+A/G vs. GG: OR = 0.81, P= 0.233 for Asians; OR = 0.95, P= 0.761 for Caucasians). No publication bias was detected by either the funnel plot or the Egger’s test (A/A+A/G vs. GG:PBegg= 0.602;PEgger= 0.353).
Overall survival. Nine studies including 2,053 subjects were included for the final analysis. Among them, 4 studies used dominant model, 5 studies used homozygous model, and 6 used heterozygous model. The data of included studies were combined according to the genetic model, respectively. The pooled outcome indicated that the A/A genotype was marginally associated with a poorer OS compared with G/G genotype (A/A vs. G/G: HR = 1.29, P= 0.055). No association was found in the other two genetic models (Fig 5; Table 2). There was no publication bias given the symmetrical distributions of the funnel plot or the Egger’s test (A/A+A/G vs. GG:PBegg= 0.308;PEgger= 0.259).
Progression -free survival. Only three studies were eligible for the analysis of the association between XPD Asp312Asn polymorphism and PFS. In homozygous and heterozygous models, the HRs were 0.97 (P= 0.92) and 0.90 (P= 0.437), respectively (Table 2). No publication bias was detected in the funnel plots or Egger’s test (A/G vs. G/G: PBegg= 1.0; P
Egger= 0.387).
Discussion
In this meta-analysis, we found no statistical evidence for an association between twoXPDSNPs (Asp312Asn/Lys751Gln) and overall clinical outcomes of NSCLC patients treated with platinum-based chemotherapy. However, stratified analysis indi-cated an ethnic difference by showing that the A/C and C/C genotypes ofXPD751 polymorphism were significantly associated with favorable objective response in Caucasian patients while a higher progression risk in Asian patients.
Although platinum-based doublet chemotherapy is currently considered as the standard care for first-line treatment of advanced NSCLC, a large proportion of patients display varying levels of resistance, indicating a remarkable individual variability in the therapeutic efficacy and prognosis. The heterogeneity could not be fully explained by currently used prognostic parameters in clinical setting such as TNM stage, performance status, and weight loss. Thus, identifying new biomarkers for better predictive and prognostic assessment is urgently needed. Single nucleotide polymorphisms are now considered as potential candidate biomarkers for cancer prognosis due to their modification of functions of critical genes involved in phenotypic drug sensitivity. Mechanisms of platinum mediated cytotoxicity include the formation of bulky DNA adducts resulting in both inter- and intra-strand cross-links that block DNA replication and lead to cancer cell death. The platinum-DNA adducts are recognized and removed by the nucleotide excision repair (NER) pathway, which modulates platinum-based chemotherapeutic efficacy by removing platinum-produced DNA damage [23,24]. The DNA repair protein XPD has been identified as a critical molecular in DNA lesion removal by NER through exerting two primary functions (i) stabilization of the transcription factor complex TFIIH; and (ii) 59R39helicase function. Experimental evidence has indicated that
XPD overexpression leads to bifunctional alkylating agent drug resistance and accelerated removal of interstrand cross-links [25]. Several common and putatively functional SNPs have been found
Figure 3. Subgroup analysis by ethnicity of objective response and survival in NSCLC patients treated with platinum-based chemotherapy according to XPD Lys751Gln polymorphism (A/C+C/C vs. A/A).(A) objective response; (B) OS; (C) PFS.
XPD Objective response Overall survival Progression-free survival
Lys751Gln Study{
Pooled OR P/Phet* Study{
Pooled HR P/Phet* Study{
Pooled HR P/Phet*
A/C vs. A/A 10 1.05(0.77–1.44) 0.742/0.894 6 1.09(0.91–1.30) 0.369/0.446 4 1.02(0.81–1.28) 0.873/0.345
C/C vs. A/A 7 1.09(0.49–2.44) 0.828/0.059 5 1.29(0.87–1.91) 0.198/0.011 4 0.99(0.64–1.53) 0.948/0.084
A/C+C/C vs. A/A
All 16 1.02(083–1.26) 0.818/0.104 13 1.03(0.91–1.18) 0.631/0.199 9 1.09(0.94–1.27) 0.267/0.287
Asian 8 0.80(0.60–1.07) 0.129/0.597 7 1.11(0.94–1.31) 0.217/0.062 3 1.39(1.07–1.81) 0.015/0.879
Caucasian 8 1.35(1.0–1.83) 0.050/0.122 6 0.92(0.74–1.13) 0.430/0.860 5 0.92(0.74–1.13) 0.418/0.477
Objective response Overall survival Progression-free survival
Asp312Asn Study{
Pooled OR P/Phet* Study{
Pooled HR P/Phet* Study{
Pooled HR P/Phet*
A/G vs. G/G 7 0.93(0.63–1.37) 0.718/0.665 6 1.03(0.70–1.50) 0.894/0.016 3 0.90(0.69–1.17) 0.437/0.609
A/A vs. G/G 5 0.98(0.51–1.90) 0.952/0.339 5 1.29(0.99–1.69) 0.055/0.324 2 0.97(0.53–1.78) 0.920/0.469
A/G+A/A vs. G/G
All 10 0.87(0.68–1.12) 0.284/0.770 4 1.78(0.89–3.55) 0.101/0.001 - -
-Asian 4 0.81(0.57–1.14) 0.233/0.275 - - -
-Caucasian 6 0.95(0.67–1.35) 0.761/0.905 - - -
-{
Study: the number of studies included in the analysis. *Phet:Pvalue of between-study heterogeneity. doi:10.1371/journal.pone.0079864.t002
XPD
Gene
Polymorp
hisms
and
Platinum
Therapy
ONE
|
www.ploson
e.org
8
November
2013
|
Volume
8
|
Issue
11
|
in XPD encoding sequence, of which rs13181 and rs1799793 SNPs [Asp312Asn (G.A) and Lys751Gln (A.C), respectively] are associated with suboptimal DNA repair capacity [15,16]. Therefore, it is conceivable that the two functional SNPs ofXPD
might reveal platinum sensitivity as an inborn trait, and have prognostic values among NSCLC patients treated with platinum agents. A number of molecular epidemiological studies have
reported the relationship betweenXPDSNPs and clinical outcome in NSCLC patients treated with platinum based chemotherapy. However, the estimates between the studies differed considerably and no consensus has yet been reached.
By pooling dataset of 24 studies investigating the predictive role of XPD Asp312Asn (G.A) and Lys751Gln (A.C) in clinical outcome of NSCLC patients treated with platinum regimen, we
Figure 5. Forest plot of objective response and overall survival in NSCLC patients treated with platinum-based chemotherapy according to XPD Asp312Asn polymorphism (A/G+A/A vs. G/G).(A) objective response; (B) OS.
found that none of the two polymorphisms was related to TR, PFS or OS in overall population, which is consistent with the findings of the previous meta-analysis by Ming Yinet al. [26]. On the other hand, in our stratified analysis by ethnicity, it was striking to find that theXPD Lys751Gln polymorphism was significantly associ-ated with favorable objective response in Caucasians but with unfavorable PFS in Asians, which was not reported in the previous meta-analysis. The discrepant results might be due to a significantly larger sample size (2,383 vs. 694 for TR; 2,001 vs. 640 for PFS) of our meta-analysis, which remarkably improves the statistical power to detect a significant association and subse-quently draw a more reliable conclusion. Notably, there was an apparent discrepancy between Asians and Caucasians in the prognostic value of XPD rs13181 C allele, and the existence of ethnical difference was confirmed by statistical test (P,0.05). The discrepancy could be explained by the fact that the treatment outcome of platinum agents may be influenced by gene-gene interaction from different genetic background and gene-environ-ment interaction from different lifestyle. Moreover, other factors such as selection bias and different matching criteria may play a role.
Despite our efforts in performing a comprehensive and accurate analysis, limitations of our meta-analysis need to be pointed out. Firstly, differences in several characteristics of the study designs, including subject selection, chemotherapeutic protocol, and follow-up time may have caused wide heterogeneity in the results among included studies. Stratified analysis by the important host-, or treatment-related factors would be helpful to reduce the heterogeneity and improve the quality of meta-analysis. However, few of the studies provided information about genotype distribu-tion by subgroups, thus making such analyses impossible. Secondly, a proportion of estimates used in the analysis were unadjusted because not all included studies reported adjusted estimates. Even they did, the estimates were not adjusted by the uniform potential confounders. Thirdly, although toxicity is an important concern in the combinational therapy with platinum compounds in advanced NSCLC patients, the association between
XPD SNPs and platinum toxicities was unable to be evaluated because few studies provided related data; even they did, different
toxicity profiles were used in the studies. Finally, the role of gene-gene and gene-gene-environment interactions was not considered in the present analysis due to our lack of access to the original data from the included studies.
Nevertheless, several advantages of our meta-analysis should be acknowledged. First, significant number of subjects pooled from various studies significantly increased statistical power of the analysis. This is the latest meta-analysis on the XPD polymor-phisms on platinum-based chemotherapy in NSCLC patients. We have included 24 studies versus 22 studies included in a recent meta-analysis [27], and 12 studies included in a meta-analysis published in 2011 [28]. Second, we analyzed the association of XPD polymorphisms with PFS, which was not addressed in previous meta-analysis studies [27,28]. PFS is an important parameter that provides guidance for tumor chemotherapy. Thus our results will help predict prognosis of NSCLS patients. Third, the quality of studies included in this meta-analysis strictly satisfied our selection criteria, thus limiting the potential bias.
In conclusion, our meta-analysis indicated thatXPDLys751Gln polymorphism may be useful prognostic factors for assessing objective response and progression risk in advanced NSCLC patients treated with platinum-based regimen according to different ethnicities. However, further prospective studies with large sample size and long-term follow-up are required to confirm our findings. In addition, particular attention should be given to the role of gene-gene as well as gene-environment interactions in the modification of chemotherapy efficacy.
Supporting Information
Table S1 PRISMA checklist.
(DOC)
Author Contributions
Conceived and designed the experiments: QQ CZ XY HZ JL LZ XS. Performed the experiments: QQ CZ XY HZ BY JC HC. Analyzed the data: QQ CZ XY HZ JM JL ZL. Contributed reagents/materials/analysis tools: QQ CZ XY HZ BY JC HC JL LZ LX. Wrote the paper: QQ CZ XY XS.
References
1. Jemal A, Thomas A, Murray T, Thun M (2002) Cancer statistics, 2002. CA Cancer J Clin 52: 23–47.
2. Parkin DM, Pisani P, Ferlay J (1999) Estimates of the worldwide incidence of 25 major cancers in 1990. Int J Cancer 80: 827–841.
3. Einhorn LH (2008) First-line chemotherapy for non-small-cell lung cancer: is there a superior regimen based on histology? J Clin Oncol 26: 3485–3486. 4. Ardizzoni A, Boni L, Tiseo M, Fossella FV, Schiller JH, et al. (2007)
Cisplatin-versus carboplatin-based chemotherapy in first-line treatment of advanced non-small-cell lung cancer: an individual patient data meta-analysis. J Natl Cancer Inst 99: 847–857.
5. Liu L, Wu C, Wang Y, Zhong R, Duan S, et al. (2011) Combined effect of genetic polymorphisms in P53, P73, and MDM2 on non-small cell lung cancer survival. J Thorac Oncol 6: 1793–1800.
6. Liu L, Wu J, Zhong R, Wu C, Zou L, et al. (2012) Multi-loci analysis reveals the importance of genetic variations in sensitivity of platinum-based chemotherapy in non-small-cell lung cancer. Mol Carcinog.
7. Liu L, Wu J, Wu C, Wang Y, Zhong R, et al. (2011) A functional polymorphism (-1607 1G—.2G) in the matrix metalloproteinase-1 promoter is associated with development and progression of lung cancer. Cancer 117: 5172–5181. 8. Ke J, Zhong R, Zhang T, Liu L, Rui R, et al. (2013) Replication study in
Chinese population and meta-analysis supports association of the 5p15.33 locus with lung cancer. PLoS One 8: e62485.
9. van de Vaart PJ, Belderbos J, de Jong D, Sneeuw KC, Majoor D, et al. (2000) DNA-adduct levels as a predictor of outcome for NSCLC patients receiving daily cisplatin and radiotherapy. Int J Cancer 89: 160–166.
10. Wu Q, Christensen LA, Legerski RJ, Vasquez KM (2005) Mismatch repair participates in error-free processing of DNA interstrand crosslinks in human cells. EMBO Rep 6: 551–557.
11. Azuma K, Komohara Y, Sasada T, Terazaki Y, Ikeda J, et al. (2007) Excision repair cross-complementation group 1 predicts progression-free and overall survival in non-small cell lung cancer patients treated with platinum-based chemotherapy. Cancer Sci 98: 1336–1343.
12. Gurubhagavatula S, Liu G, Park S, Zhou W, Su L, et al. (2004) XPD and XRCC1 genetic polymorphisms are prognostic factors in advanced non-small-cell lung cancer patients treated with platinum chemotherapy. J Clin Oncol 22: 2594–2601.
13. Lord RV, Brabender J, Gandara D, Alberola V, Camps C, et al. (2002) Low ERCC1 expression correlates with prolonged survival after cisplatin plus gemcitabine chemotherapy in non-small cell lung cancer. Clin Cancer Res 8: 2286–2291.
14. Spitz MR, Wu X, Wang Y, Wang LE, Shete S, et al. (2001) Modulation of nucleotide excision repair capacity by XPD polymorphisms in lung cancer patients. Cancer Res 61: 1354–1357.
15. Duell EJ, Wiencke JK, Cheng TJ, Varkonyi A, Zuo ZF, et al. (2000) Polymorphisms in the DNA repair genes XRCC1 and ERCC2 and biomarkers of DNA damage in human blood mononuclear cells. Carcinogenesis 21: 965– 971.
16. Lunn RM, Helzlsouer KJ, Parshad R, Umbach DM, Harris EL, et al. (2000) XPD polymorphisms: effects on DNA repair proficiency. Carcinogenesis 21: 551–555.
17. Isla D, Sarries C, Rosell R, Alonso G, Domine M, et al. (2004) Single nucleotide polymorphisms and outcome in docetaxel-cisplatin-treated advanced non-small-cell lung cancer. Ann Oncol 15: 1194–1203.
19. Mathiaux J, Le Morvan V, Pulido M, Jougon J, Begueret H, et al. (2011) Role of DNA repair gene polymorphisms in the efficiency of platinum-based adjuvant chemotherapy for non-small cell lung cancer. Mol Diagn Ther 15: 159–166. 20. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR (2007) Practical
methods for incorporating summary time-to-event data into meta-analysis. Trials 8: 16.
21. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, et al. (2000) New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 92: 205–216.
22. Altman DG, Bland JM (2003) Interaction revisited: the difference between two estimates. BMJ 326: 219.
23. Furuta T, Ueda T, Aune G, Sarasin A, Kraemer KH, et al. (2002) Transcription-coupled nucleotide excision repair as a determinant of cisplatin sensitivity of human cells. Cancer Res 62: 4899–4902.
24. de las Penas R, Sanchez-Ronco M, Alberola V, Taron M, Camps C, et al. (2006) Polymorphisms in DNA repair genes modulate survival in cisplatin/gemcita-bine-treated non-small-cell lung cancer patients. Ann Oncol 17: 668–675. 25. Aloyz R, Xu ZY, Bello V, Bergeron J, Han FY, et al. (2002) Regulation of
cisplatin resistance and homologous recombinational repair by the TFIIH subunit XPD. Cancer Res 62: 5457–5462.
26. Yin M, Yan J, Voutsina A, Tibaldi C, Christiani DC, et al. (2011) No evidence of an association of ERCC1 and ERCC2 polymorphisms with clinical outcomes of platinum-based chemotherapies in non-small cell lung cancer: a meta-analysis. Lung Cancer 72: 370–377.
27. Qiu M, Yang X, Hu J, Ding X, Jiang F, et al. Predictive Value of XPD Polymorphisms on Platinum-Based Chemotherapy in Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. PLoS One. 2013 Aug 19;8(8):e72251.
28. Wei SZ, Zhan P, Shi MQ, Shi Y, Qian Q, et al. Predictive value of ERCC1 and XPD polymorphism in patients with advanced non-small cell lung cancer receiving platinum-based chemotherapy: a systematic review and meta-analysis. Med Oncol. 2011 Mar;28(1):315–21.
29. Cheng H, Qin Q, Sun X, Li F, Sun N, et al. (2013) Predictive Effect of XPA and XPD Polymorphisms on Survival of Advanced NSCLC Patients Treated with Platinum-based Chemotherapy: A Three-dimensional (3-D), Polyacrylamide Gel-Based DNA Microarray Method. Technol Cancer Res Treat.
30. Li XD, Han JC, Zhang YJ, Li HB, Wu XY (2013) Common variations of DNA repair genes are associated with response to platinum-based chemotherapy in NSCLCs. Asian Pac J Cancer Prev 14: 145–148.
31. Chen X, Sun H, Ren S, Kim Curran V, Zhang L, et al. (2012) Association of XRCC3 and XPD751 SNP with efficacy of platinum-based chemotherapy in advanced NSCLC patients. Clin Transl Oncol 14: 207–213.
32. Li D, Zhou Q, Liu Y, Yang Y, Li Q (2012) DNA repair gene polymorphism associated with sensitivity of lung cancer to therapy. Med Oncol 29: 1622–1628. 33. Liao WY, Shih JY, Chang GC, Cheng YK, Yang JC, et al. (2012) Genetic polymorphism of XRCC1 Arg399Gln is associated with survival in non-small-cell lung cancer patients treated with gemcitabine/platinum. J Thorac Oncol 7: 973–981.
34. Provencio M, Camps C, Cobo M, De las Penas R, Massuti B, et al. (2012) Prospective assessment of XRCC3, XPD and Aurora kinase A single-nucleotide
polymorphisms in advanced lung cancer. Cancer Chemother Pharmacol 70: 883–890.
35. Wu W, Li H, Wang H, Zhao X, Gao Z, et al. (2012) Effect of polymorphisms in XPD on clinical outcomes of platinum-based chemotherapy for Chinese non-small cell lung cancer patients. PLoS One 7: e33200.
36. Ren S, Zhou S, Wu F, Zhang L, Li X, et al. (2012) Association between polymorphisms of DNA repair genes and survival of advanced NSCLC patients treated with platinum-based chemotherapy. Lung Cancer 75: 102–109. 37. Zhang ZY, Tian X, Wu R, Liang Y, Jin XY (2012) Predictive role of ERCC1
and XPD genetic polymorphisms in survival of Chinese non-small cell lung cancer patients receiving chemotherapy. Asian Pac J Cancer Prev 13: 2583– 2586.
38. Ludovini V, Floriani I, Pistola L, Minotti V, Meacci M, et al. (2011) Association of cytidine deaminase and xeroderma pigmentosum group D polymorphisms with response, toxicity, and survival in cisplatin/gemcitabine-treated advanced non-small cell lung cancer patients. J Thorac Oncol 6: 2018–2026.
39. Vinolas N, Provencio M, Reguart N, Cardenal F, Alberola V, et al. (2011) Single nucleotide polymorphisms in MDR1 gen correlates with outcome in advanced non-small-cell lung cancer patients treated with cisplatin plus vinorelbine. Lung Cancer 71: 191–198.
40. Liu L, Yuan P, Wu C, Zhang X, Wang F, et al. (2011) Assessment of XPD Lys751Gln and XRCC1 T-77C polymorphisms in advanced non-small-cell lung cancer patients treated with platinum-based chemotherapy. Lung Cancer 73: 110–115.
41. Li F, Sun X, Sun N, Qin S, Cheng H, et al. (2010) Association between polymorphisms of ERCC1 and XPD and clinical response to platinum-based chemotherapy in advanced non-small cell lung cancer. Am J Clin Oncol 33: 489–494.
42. Kalikaki A, Kanaki M, Vassalou H, Souglakos J, Voutsina A, et al. (2009) DNA repair gene polymorphisms predict favorable clinical outcome in advanced non-small-cell lung cancer. Clin Lung Cancer 10: 118–123.
43. Yao CY, Huang XE, Li C, Shen HB, Shi MQ, et al. (2009) Lack of influence of XRCC1 and XPD gene polymorphisms on outcome of platinum-based chemotherapy for advanced non small cell lung cancers. Asian Pac J Cancer Prev 10: 859–864.
44. Gandara DR, Kawaguchi T, Crowley J, Moon J, Furuse K, et al. (2009) Japanese-US common-arm analysis of paclitaxel plus carboplatin in advanced non-small-cell lung cancer: a model for assessing population-related pharmaco-genomics. J Clin Oncol 27: 3540–3546.
45. Booton R, Ward T, Heighway J, Taylor P, Power F, et al. (2006) Xeroderma pigmentosum group D haplotype predicts for response, survival, and toxicity after platinum-based chemotherapy in advanced nonsmall cell lung cancer. Cancer 106: 2421–2427.
46. Ryu JS, Hong YC, Han HS, Lee JE, Kim S, et al. (2004) Association between polymorphisms of ERCC1 and XPD and survival in non-small-cell lung cancer patients treated with cisplatin combination chemotherapy. Lung Cancer 44: 311–316.