Tissue Engineering Approach for Reconstructing Bone
Defects Using Mesenchymal Stem Cells
Mohamadreza Baghaban Eslaminejad, Ph.D.*, Fatemeh Bagheri, M.Sc.
Stem Cell and Developmental Biology Department, Cell Sciences Research Center for Stem Cell Biology and Technology, Royan Institute, ACECR, Tehran, Iran
* Corresponding Address: P.O.Box: 19395-4644, Stem Cell and Developmental Biology Department, Cell Sciences Research Center for Stem Cell Biology and Technology, Royan Institute, ACECR, Tehran, Iran
Email: [email protected] Abstract
Received: 21/Dec/2008, Accepted: 22/Apr/2009
Regeneration of large bone defects is considered a challenging task by facio-mandibular and orthopedic surgeons. In these circumstances, either bone grafts or metal implants are currently being used. The inherent limitations associated with these methods have directed the attention of investigators to new technologies such as bone tissue engineering, a multi-disciplinary field in which life science as well as engineering is involved to manufacture an appropriate bone construct. The objectives of scientists involved in this field are to design and manufacture scaffolds with appropriate chemical and physical features, to direct cell dif-ferentiation within the scaffold using appropriate culture conditions and finally to render the engineered construct applicable for clinical use. In this article, the main components involved in the bone tissue engineering process have been reviewed. These include cells (with an emphasis on mesenchymal stem cells), scaffolds, growth factors and bioreactors, and tissue engineering approaches to tissue regeneration.
Keywords: Tissue Engineering, Bone Diseases, Mesenchymal Stem Cells, Scaffold
Yakhteh Medical Journal, Vol 11, No 3, Autumn 2009, Pages: 263-272
Review Article
Introduction
Bone structure and development
Bone is a live, dynamic tissue with a rich blood supply and a specific capacity for regeneration (1). Bone tissue could be considered to have at least four functions. It serves as a structural scaffold to which muscles are attached and plays a major role in their contraction. Bone supports the body vital organs including brain, spinal cord and bone marrow. Bone tissue is the main source of calcium and phosphate and bone (internal spaces) provides an appropriate microenvironment for hematopoi-etic cell differentiation (2). To facilitate the latter function, bone is elaborated from a complex archi-tecture composed of organic materials, inorganic materials and water. Inorganic material mainly takes the form of hydroxyapatite crystal (3). Min-erals including magnesium, potassium, fluoride, phosphate and citrate constitute a minor part of the inorganic material (4). The organic matrix of bone is mainly composed of type I collagen (more than 95%-97%). Organic materials include other colla-gen isoforms, and non-collacolla-genous proteins such as osteocalcin, osteonectin, osteoadherin, fibronectin, bone sialoprotein, thrombospondin, proteoglycan and glycosaminoglycan (5, 6).
There are three types of cells in bone tissue: os-teoblast, osteocyte and osteoclast. Osteoblasts are
bone-forming cells which have the high alkaline phosphatase activity required for bone mineraliza-tion. Osteocytes are actually ostoblastic cells that are trapped within their own deposited matrix dur-ing the osteogenesis process. Osteoclasts are bone macrophages specialized in bone resorption. (7). Bone histogenesis could be mediated by either intra-membranous or endo-chondral processes. In intra-membranous ossification, bone forms when mesenchymal precursors condense and differenti-ate directly into osteoblasts while in endochondral ossification, precursor cells first differentiate into cartilage cells, which are then replaced by bone cells (8).
Bone defects
insufficient attention has been paid to the treatment of these conditions (9).
Current treatments of bone defects
Among bone repair methods, autograft transplants are considered to be the gold standard (10) since they bring osteogenic, osteoinductive and osteo-conductive components to the defect sites without triggering host immune response. However, as the quantity of bone marrow that can be obtained for autograft is limited, and because it requires an ex-tensive operation which may cause morbidity, pain and possible infection of the donor site, there is an ongoing search for alternatives (11-13). Allograft bone transplantation is a potential alternative which overcomes the problem of quantity as it could be obtained from cadaver tissue. Allograft disadvan-tages, however, include less osteoinductivity, pos-sible trigger of host immune response and likely transmission of disease (11, 14). Another choice would be the use of metal implants. Although these substitutes are applicable in some cases they pos-sess several disadvantages; including first, they do not degrade after implantation, hence, secondary surgery is necessary to remove them from the host and second, they may release toxic ions which trig-ger host immune response and infection (15, 16). Synthetic materials or alloplasts are being sug-gested as the other choice for application in bone regeneration, but they are not particularly appro-priate as the host treats them as a foreign body and creates a thin fibrous membrane around them. This prevents the alloplast from being integrated into the host tissue and consequently being rejected (9). To overcome this problem, the attention of inves-tigators has been directed to new technologies as approaches to bone tissue engineering.
Modern treatment of bone large defects
Nowadays, bone constructs elaborated according to tissue engineering principals are regarded as an ideal choice to reconstruct bone segmental defects. Tissue engineering is a multidisciplinary science, defined as the application of the principles and methods of life science and engineering in order to understand the relationships between structure and function in normal and injured mammalian tissues and to develop biological substitutes for the repair, maintenance and improvement of tissue function (17). The objective of this strategy is indeed to overcome the limitations exhibited by transplanta-tion of tissue grafts and biomaterials.
Tissue engineering
The components that are involved in a tissue
en-gineering process include cells, scaffolds, growth factors and bioreactors.
Cells
Osteogenic cells are essential components in all advanced bone tissue engineering strategies. These include mesenchymal stem cell (MSCs) and ordi-nary bone cells (18-20).
Since the proliferation capacity of specialized cells in tissue is limited, ordinary bone cells (osteoblast) would not be appropriate for tissue engineering strategies. Furthermore, long-term cultivation of these cells is usually associated with their reduced activity. For this reason, MSCs are preferred over ordinary cells in most investigations. There are many review articles of the basic biology of MSCs (21-25).
Briefly, MSCs are characterized by two proper-ties: the ability to extensively replicate and the capacity to differentiate into multiple cell lines. These cells are resident in many tissues in adults, including bone marrow (26-28). The notion that bone marrow houses osteogenic precursor cells was first proposed by Petrakova et al. who indi-cated the osteogenic ability of marrow cells trans-planted under the renal capsule (29). Since MSCs are usually obtained from the patient’s own bone marrow aspirates, their transplantation is not as-sociated with host versus graft reaction. Further-more, some research has indicated that MSCs ex-press no HLA class II receptor indicating that even non-autologous transplantation would not trigger host immune response (30).
Scaffold
Scaffolds are artificial matrices designed to mimic the mechanical and biological properties of the tissue matrix. Cells in tissues produce matrix that contains tissue specific molecules. The matrix, in turn, creates a complex network that supports the tissue and determines the shape of the tissue. In this tri-dimensional microenvironment, matrix-cell interaction initiates and promotes growth, migrations, differentiation, viability and organiza-tion of the cells as well as the remodeling of the matrix (31). In tissue engineering strategies, scaf-folds provide three-dimensional spaces for the cells to undergo proliferation and differentiation. Moreover, scaffolds serve as carriers to transfer cells and bioactive materials to defect sites (32).
Characteristics of scaffolds for bone tissue engi-neering
proper-ties similar to bone tissue. Scaffolds implanted in the body must be able to undergo degradation in order to be replaced by new tissue. The degrada-tion rate must be propordegrada-tional to the formadegrada-tion rate of the new tissue. If scaffold degrades rap-idly, it would be followed by fracture, and slow degradation would prevent new tissue formation (33-36). Products resulting from scaffold degra-dation should not be immunogenic or cytotoxic (33, 37). Moreover, scaffold porosity should be appropriate in terms of pore numbers, size and morphology (33, 35). These parameters are cru-cial to the nutrition of cells and penetration of vessels (38). Different ranges of pore size includ-ing 200-400 μm (39), 100-150 μm (33) and
100-600 μm (40) have been suggested for scaffolds
suitable for bone repair. In addition, scaffolds for bone tissue should possess a high surface/volume ratio (41). Interconnectivity of the pores is also a crucial factor which facilitates the diffusion of nutrients and formation of vessels (33, 35, 41). Since bone defects are irregular in shape and of different sizees, bone scaffolds should have the capacity to be manufactured in varieties of forms and sizes. The surface property of the scaffold is the other significant parameter that can influence the adherence of cells and their subsequent pro-liferation and differentiation. In this regard, the scaffolds’ surface characteristics, chemical en-ergy and composition are important factors (42, 43). Since a material with ideal surface properties is rare, the modification of most scaffold surfaces is inevitable (44, 45). A negative electrical charge oo the scaffold surface facilitates MSC adhesion, as well as expansion therein (46).
Seeded cells adhere to scaffolds surfaces either by receptor-independent or receptor-dependent mechanisms. In receptor-independent attachment, the adhesion is mediated by chemical bonds in-cluding hydrogen bonds and electrostatic attrac-tion between cell surface molecules and funcattrac-tion- function-al chemicfunction-al groups on the scaffold surfaces. Since such adhesions provide insufficient signal from the external environment into the cells, as conse-quence, cells may lose their viability. Receptor-dependent adhesion is mediated by extracellular matrix (ECM) molecules such as fibronectin, vitronectin, collagen and laminin (47). In order to improve cell adhesion, some researchers have focused on the incorporation of integrin domains including arginine-glycine-aspartate (RGD) oli-gopeptide on the scaffold’s surfaces (13).
Scaffold classification
Scaffolds can be classified as ceramic scaffolds,
natu-ral scaffolds, synthetic scaffolds and Hydrogels.
Ceramic scaffolds
Hydroxy apatite and tricalcium phosphate are among the ceramics most frequently used for bone tissue engineering because they consti-tute the main part of the natural bone matrix (48-50). Although these materials exhibit some valuable properties for bone tissue engineering, several disadvantages limit their application. These ceramics are very fragile and possess low mechanical stability. In addition, their degrada-tion rate is not very predictable. Degradadegrada-tion of these ceramics results in a considerable increase in blood levels of calcium and phosphate (51). To overcome the limitation associated with the mechanical stability of these ceramics we have recently fabricated a hybrid scaffold using tri-calcium phosphate in conjunction with alginate and gelatin (52).
Natural scaffolds (polymer)
Polysaccarids such as cellulose, starch, varieties of dextran, alginates, chitin/chitosan and gly-cosaminoglycan (GAG); specifically hyaloronic acids or proteins such as collagen, silk fibroin would be classified as natural scaffolds. Poly hy-droxyl butyrate, which is derived from bacteria, is also being considered as a natural scaffold (53, 54). The main advantages of these scaffolds are their low immunogenicity, high inherent bioac-tive properties, capacity for good interaction with the host tissue, high chemical diversity and, in some cases, unlimited sources (53).
Collagen, a natural polymer, can easily be obtained from tissues using enzymatic digestion and acid/ salt extraction. This polymer is frequently used as bone scaffolds in tissue engineering approaches. One advantage of collagen scaffold is that it can readily be degraded by the enzymatic activity of cytoplasmic lysosomes. The degradation rate can be controlled by manipulation of the specimen density and the level of cross-linkage between collagen molecules. Arg-Gly-Asp (RGD) peptide domains in collagen serve to maintain phenotype and activity of the cells (55).
Since collagen I constitutes the major protein of bone matrix, it increases adhesion and matura-tion of osteogenic cells (56). The disadvantage of collagen is its poor mechanical properties. Adding hard materials as hydroxy apatite may overcome this problem. Both collagen and hy-droxy apatite possess inhibitory effects on bacte-rial growth (57). Furthermore, collagen is being considered as ideal carrier for bone morphogenic
protein (BMP) (58). To enhance its structural characteristic and improve osteogenic capacity, collagen needs to be used in conjunction with mineral calcium (59), a non-proteinous polymer, such as chondroitin sulfate (60), poly lactic acid (61), poly lactic co-glycolic acid (62) and poly tetrafluoroethylene (63). Recently we demon-strated other properties of collagen in bone tis-sue engineering. According to our findings, Type I collagen gel in the seeding medium improves murine mesenchymal stem cell loading onto the scaffold, increases their subsequent proliferation, and enhances culture mineralization (64).
Among the other bone matrix molecules that are effective in osteogenesis is GAG which is com-posed of long carbohydrate chains (65, 66). Hyal-oronan has been indicated to have both osteocon-ductive and osteoinosteocon-ductive properties (67, 68). In addition, the positive roles of sulfated GAG, their combination with collagen and perlecan in bone differentiation have been reported (69, 70).
Synthetic scaffolds (polymer)
In this group are several scaffolds including poly lactic acid (PLA), poly lactic co-glycolic acid (PLGA), poly ethylene glycol, poly caprolacton, poly vinyl alcohol and alumina (71-75).
Aliphatic polyesters such as poly glycolic acid (PGA), poly-l-lactic acid (PLLA) and poly (lactic-co-glycolic acid) (PLGA) are the most frequently used polymers in tissue engineering and have ob-tained Food and Drug Administration (US) ap-proval for human use. They degrade with non-en-zymatic hydrolysis (55). Degradation products are released into body fluids and excreted through nat-ural metabolic pathways. Degradation time varies between several weeks to several months depend-ing on their crystal structure, molecular weight and the ratio of copolymer lactic acid and glycolic acid in their structure. These scaffolds can be easily pre-pared in different shapes and dimensions because they are flexible at high temperatures (76). Syn-thetic scaffolds are preferred over natural scaffolds since comparatively they have superior mechani-cal properties, and an appropriate degradation rate and microstructure.
Use of synthetic scaffolds with ceramic nano par-ticles could be a revolutionary approach in the bone tissue engineering field. Recently we have indicated that PLLA/ nano hydroxyapatite scaf-folds possessed good mechanical properties and biocompatibility compared with PLLA alone. Ac-cording to our findings the hybrid scaffolds sup-ported MSC adhesion and proliferation more than PLLA alone (77).
Hydrogels
Hydrogels are polymeric systems with cross-linked structures capable of absorbing a consid-erable volume of water-based solutions. Cells are trapped within the hydrogel during the gelation process. The number of pores in hydrogels can be determined by adding a certain amount of cross-linker which, in turn, determines the volume of water absorbed by the hydrogels (78). The dis-advantage of hydrogels is their poor mechanical properties. There are several important scaffolds that are classified as hydrogels. These include chi-tosan, poly vinyl alcohol, alginate and silk fibroin, the latter being considered more suitable for bone tissue engineering due to its good biocompatibil-ity, flexibility and mechanical stability (12). Al-ginates, which are derived from brown seaweed and approved by the FDA as wound cover, have frequently been used in tissue engineering proc-esses (79). Multilayer hydrogels are among the most appropriate scaffolds for cell co-culture in which one cell type secretes growth factors and matrix molecules which affect the growth and differentiation of other cell type (80).
Growth factors
induce bone forming cells into the defect site. It has been indicated that BMP2 plays a crucial role in expression of osteogenic markers including al-kaline phosphatase and osteocalcin through the mitogen-activated protein kinase (MAPK) path-way (90). BMPs have also been shown to induce the cells to express the cbaf-1/Runx2 gene (82). In tissue engineering strategies, growth factors such as platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF) are used to promote vessel formation. This is of considerable significance, especially in large con-structions in which the nutrition of the cells in deep parts of the scaffold may be impaired (91). Growth factors can be immobilized on scaffold surfaces through covalent bonds. The other meth-od would be to encapsulate growth factor within carriers which gradually destruct and release the growth factor (92, 93).
Bioreactors
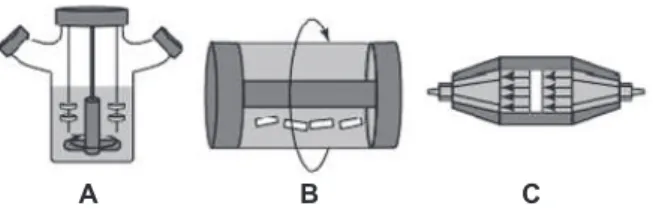
Bone tissue is a tridimensional system with a complex and mechanically active structure. In this tissue, osteoblasts are in interaction with each other while experiencing mechanical forces and consistent changes in ECM architec-ture (94). While recent studies have indicated the usefulness of mimicking the osteoblast dy-namic natural microenvironment in bone tissue engineering cultures, in most previous studies, a static cell culture was used to establish tissue engineering culture. The main disadvantage of static culture is the limitation associated with the diffusion of nutrients to deeper parts of the scaffold, leading to insufficient nutrition of the cells (95). In static culture conditions, cells can-not distribute evenly throughout the scaffolds (96, 97). In addition, static culture can not pro-vide mechanical stimulation which is important for osteocyte activity. It has been indicated that mechanical stress could enhance Cbaf-1/Runx2 expression in bone precursor cells (98). To overcome the limitation associated with static culture, bioreactors have been developed to be used in tissue engineering processes. The ob-jectives of bioreactors use are the followings: a) to provide a uniform distribution of cells within scaffolds, b) to provide cells deeper in the scaffold with sufficient nutrients c) to ex-pose the cells to mechanical stimulation appro-priate for bone differentiation and remodeling (96, 97). Bioreactors appropriate for bone tis-sue engineering include spinner flasks, rotating wall vessels and direct perfusion bioreactors (99, 101) (Fig 1).
Fig 1: Some bioreactors that are appropriate for bone tissue engineering. A: spinner flask bioreactor; B: rotating wall vessels and C: direct perfusion bioreactors (99)
Tissue engineering approaches to tissue regen-eration
The ultimate goal of the tissue engineering process is to reconstruct tissue defects. For this purpose, several strategies have been proposed. The strate-gies differ from each other in terms of the number of components (i.e. cells, scaffolds and growth factors) that each strategy utilizes to produce the construct (Fig 2).
Fig 2: Tissue engineering approaches to tissue regeneration (102).
One method would be to conduct bone regenera-tion using scaffold alone. In this strategy, scaffold is placed in defect site and host cells migrate into the scaffold pore system (37, 39, 102). Another method would be to transplant autoulogous cells alone (without scaffold) into the defect site. It has been reported that in such a method, most cells may undergo apoptotic cell death because cell vi-ability is dependent on surface adherence which is not provided in the absence of scaffold (37,102, 103). A third method would be the use of scaffold with growth factors such as BMPs, TGF b1 and PDGF (104, 105). This strategy is referred to as growth factor-based tissue engineering. The fourth strategy would be the use of scaffolds coated with cells. This is referred to as cell-based tissue engi-neering. In this approach, the scaffold serves as the carrier onto which cells can adhere, proliferate and
A B C
deposit matrix. Meanwhile, the scaffold undergoes gradual degradation and eventually it is replaced by repair tissue (106-108). In such a strategy, the scaffold serves to physically support the defect es-pecially during the early days of transplantation when the repair tissue is not yet formed (17, 39, 102, 106).
MSC-based bone tissue engineering
Several experiments have so far been conducted using MSC-based bone tissue engineering. The presence of MSCs within scaffolds can increase the rate and amount of bone formation through two mechanisms: a) first as MSCs are osteogenic cells they can be directly involved in bone formation b) second MSCs can increase the osteoconductive properties of biomaterials by releasing osteogenic factors which, in turn, facilitate ostoeoprogenitor migration into the defect site. These effects result in enhanced bone formation in the scaffold/cell construct compared to scaffold alone.
Several animal model studies, as well as clinical trials that have provided good evidence of the ef-ficiency of the MSC-based bone tissue engineer-ing approach to regeneration of large bone defects are reviewed in the following paragraphs. In a study by Bruder et al constructs consisting of 65% hydroxy apatite/35% ß tricalcium phosphate and MSCs were created. These, along with scaffold alone, were transplanted into canine 21-mm fem-oral segmental defects. The results indicated that in femurs with cell/scaffold constructs more oste-ointegration of the implants with host tissue oc-curred compared with scaffold alone. Moreover, there were several fractures in the femur treated with scaffolds that had not been transplanted with cells (109).
In a similar study, Kon et al. transplanted hydroxy apatite ceramics coated with MSCs into large de-fects in ovine tibia and compared the results with those transplanted with scaffold alone. According to their results, in scaffold/MSC constructs, bone tissue appeared to form on the outer surfaces of the scaffold, as well as in the scaffold’s internal spaces, while in scaffolds that had not been trans-planted with cells the bone was only observed on the outer surfaces of the scaffold (110).
According to our own recent observations, both hydroxyl apatite and Bio-Oss scaffold coated with MSCs can enhance ectopic bone formation when transplanted into canine master muscle (111, 112). Furthermore, we recently reported that MSCs loaded into these ceramic scaffolds can regenerate rat calvarial bone defects more ef-fectively than scaffold loaded with plasma-rich
platelet (PRP) (113). Similarly, we found that MSC/ceramic constructs can reconstruct large defects in canine mandibolar bone better than scaffold alone (114). All these studies imply that scaffold loaded with MSCs would be more effi-cient than scaffold alone.
After several preliminary animal experiments, the first report on the use of bone constructs pro-duced using the MSC-based tissue engineering approach in humans was published by Quarto et al. who prepared hydroxyl apatite ceramics the shape of the defects and loaded them with the patient own MSCs. Good integration has been observed when such constructs have been trans-planted into patient long bone with 4-8 cm seg-mental defects (115).
In a clinical trial to reconstruct a large defect in the mandible of a 56 year old man, Gronthos de-signed a titanium mesh in the form and size of the patient’s mandible defect and filled it with hydroxyl apatite porous scaffolds loaded with MSCs and rhBMP-7. The construct was then im-planted into the patient’s latissimus dorsi mus-cle for 7 weeks at the end of which the implants with acquired vascular bundles were transplanted into the patient’s defect site. A few months later, the patient was able to initiate chewing. Unfor-tunately, after 15 months, the patient died of a myocardial infarction. However, this procedure was a breakthrough in regenerative medicine us-ing tissue engineerus-ing approaches (116).
Cell loading into scaffold pore systems
system (121). Recently we have reported that the presence of collagen gel in the seeding medium can significantly enhance the efficiency of cell loading into the scaffold pores (64).
Future Prospects
The objective of bone tissue engineering is to cure large bone fractures and defects using osteo-conductive scaffolds, osteogenic cells and induc-ing growth factors. Despite all the progress that has been made in this field, clinical use remains limited due to some outstanding problems. These include the shortage of biomaterials with appropri-ate mechanical, biological and chemical character-istics, problems associated with angiogenesis in large constructs and finally the ability to produce scaffolds that correspond to the complex shape of bone defects. To overcome these limitations close collaboration between the biological sciences and engineering sciences is needed.
References
1. Rodan GA. Introduction to Bone Biology. Bone. 1992; 13: S3-S6.
2. Yaszemski MJ, Payne RG, Hayes WC, Langer R, Mikos AG. Evolution of bone transplantation: Molecular, cellular and tissue strategies to engineer human bone. Biomaterials. 1996; 17: 175-85.
3. Hellmich C, Ulm FJ. Average hydroxyapatite concen-tration is uniform in the extracollagenous ultrastructure of mineralized tissues: Evidence at the 1-10-microm scale. Biomech Model Mechanobiol. 2003; 2: 21-36.
4. Rey C, Kim HM, Gerstenfeld L, Glimcher MJ. Struc-tural and chemical characteristics and maturation of the calcium phosphate crystals formed during the cal-cification of the organic matrix synthesized by chicken osteoblasts in cell culture. J Bone Miner Res. 1995; 10: 1577-1588.
5. Young MF, Kerr JM, Ibaraki K, Heegaard AM, Robey PG. Structure, expression, and regulation of the major noncollagenous matrix proteins of bone. Clin Orthop. 1992; 281: 275-294.
6. Robey PG. Vertebrate mineralized matrix proteins: Structure and function. Connect Tissue Res. 1996; 35: 131-136.
7. Hall BK. Bones and cartilage. developmental evo-lutionary skeletal biology. New York: Academic Press; 2005; 13-30
8. Olsen BR, Reginato AM, Wang W. Bone development. Annu Rev Cell Dev Biol. 2000; 16: 191-220.
9. kaigler D, Mooney D. Tissue engineering’s impact on dentistry. J dent Edu. 2001; 65: 456-462.
10. Gazdag AR, Lane JM, Glaser D, Forster RA. Alterna-tives to autogenous bone graft: efficacy and indications. J Am Acad Orthop Surg. 1995; 3: 1-8.
11. Ikada Y. Challeng in tissue engineering. J R Soc In-terface. 2006; 3: 589-601.
12. Tanaka T, Hirose M, Kotobuki N , Ohgushi H, Furu-zono T, Sato J. Nano-scaled hydroxyapatite/silk fibroin
sheets support osteogenic differentiation of rat bone marrow mesenchymal cells. Mater Sci Eng C. 2007; C 27: 817-823.
13. Logeart-Avramoglou D, Anagnostou F, Bizios R, Pe-tite H. Engineering bone: challenges and obstacles. J Cell Mol Med. 2005; 9: 72-84.
14. de Boer HH. The history of bone grafts. Clin Orthop. 1988; 226: 292-298.
15. Törmälä P, Vainionpää S, Kilpikari J, Rokkanen P. The effects of fibre reinforcement and gold plating on the flexural and tensile strength of PGA/PLA copolymer materials in vitro. Biomaterials. 1987; 8(1): 42-5. 16. Chen CC, Chueh J-Y Tseng H, Huang H-M, Lee S-Y. Preparation and characterization of biodegradable PLA polymeric blends. Biomaterials. 2003; 24: 1167-1173. 17. Langer R, Vacanti JP. Tissue engineering. Science. 1993; 260: 920-926.
18. Aubin JE. Bone stem cells. J Cell Biochem. 1998; S 30-31: 73-82.
19. Stangenberg L, Schaefer DJ, Buettner O, Ohnolz J, Moebest D, Horch RE, et al. Differentiation of osteob-lasts in three-dimensional culture in porous cancellous bone matrix: quantitative analysis of gene expression based on real-time reverse transcription polymerase chain reaction. Tissue Eng. 2005; 11: 855-864.
20. Bruder SP, Fink DJ, Caplan AI. Mesenchymal stem cells in bone development, bone repair, and skeletal re-generation therapy. J Cell Biochem. 1994; 56: 283-294. 21. Minguell JJ, Erices A, Conget P. Mesenchymal stem cells. Exp Biol Med. 2001; 226: 507-520.
22. Fibbe WE. Mesenchymal stem cells. A potential source for skeletal repair. Ann Rheum Dis. 2002; 61: ii29-ii31.
23. Barry FP. Biology and clinical applications of mes-enchymal stem cells. Birth Defects Res Part C Embryo Today. 2003; 69: 250-256.
24. Tuan RS, Boland G, and Tuli R. Adult mesenchymal stem cells and cell-based tissue engineering. Arthritis Res Ther. 2003; 5, 32-45.
25. Eslaminejad MB, Eftekhari-Yazdi P. Mesenchymal stem cells: In vitro differentiation among bone and carti-lage cell lineages. Yakhteh. 2007; 9: 158-169.
26. Presnell SC, Petersen B, Heidaran M. Stem cells in adult tissues. Semin Cell Dev Biol. 2002; 13: 369-376. 27. Guilak F, Awad HA, Fermor B, Leddy HA, Gimble JM. Adipose-derived adult stem cells for cartilage tissue engineering. Biorheology. 2004; 41: 389-399.
28. Boulton M, Albon J. Stem cells in the eye. The Inter J Biochem Cell Biol. 2004; 36: 643-657.
29. Petrakova KV, Tolmachava AA, FriedensteinAJ. Bone formation occurring in bone marrow transplan-tation in diffusion chambers. Bull exp biol med. 1963; 56(12): 87-91.
30. Le Blanc K, Tammik L, Sundberg B, Haynesworth SE, Ringden O. Mesenchymal stem cells inhibit and stimulate mixed lymphocyte cultures and mitogenic re-sponses independently of the major histocompatibility complex. Scand J Immunol. 2003; 57: 11-20.
31. Huang S, Ingber DE. The structural and mechanical complexity of cell-growth control. Nat Cell Biol. 1999; 1: E131-138.
32. Kim BS, Mooney DJ. Development of biocompatible synthetic extracellular matrices for tissue engineering. Trends Biotechno. 1998; 16(5): 224-230.
33. Maquet V, Jerome R. Design of macroporous biode-gradable polymer scaffolds for cell transplantation. Po-rous Mater Tissue Eng. 1997; 250: 15-42.
34. Middleton JC, Tipton AJ. Synthetic biodegradable polymers as orthopedic devices. Biomaterials. 2000; 21: 2335-2346.
35. Shapiro L, Cohen S. Novel alginate sponges for cell culture and transplantation. Biomaterials. 1997; 18:583-590.
36. Hutmacher DW. Scaffolds in tissue engineering bone and cartilage. Biomaterials. 2000; 21: 2529-2543. 37. Thompson R, Wake MC, Yaszemski M, Mikos AG. Biodegradable polymer scaffolds to regenerate organs. Adv Polym Sci. 1995; 122: 247-274.
38. Murphy WL, Simmons CA, Kaigler D, Mooney DJ. Bone regeneration via a mineral substrate and induced angiogenesis. J Dent Res. 2004; 83: 204-210.
39. Lu L, Mikos AG. The importance of new processing techniques in tissue engineering. MRS Bull. 1996; 21: 28-32.
40. Pirhonen E, Moimas L, Haapanen J. Porous Bioac-tive 3-D Glass Fiber Scaffolds For Tissue Engineering. Applications Manufactured By Sintering Technique. Key engineering materials. 2003; 240-242: 237-240.
41. Chen VJ, Smith LA, Ma PX. Collagen-Inspired Na-no-fibrous Poly(L-lactic acid) Scaffolds for Bone Tissue Engineering Created from Reverse Solid Freeform Fab-rication. Mat Res Soc Proc. 2004; 823.
42. Anselme K, Bigerelle M, Noel B, Dufresne E, Ju-das D, Iost A, et al. Qualitative and quantitative study of human osteoblast adhesion on materials with various surface roughnesses. J Biomed Mater Res. 2000; 49: 155-166.
43. Dobkowski J, Kolos R, Kaminski J, Kowalczynska HM. Cell adhesion to polymeric surfaces: Experimental study and simple theoretical approach. J Biomed Mater Res. 1999; 47: 234-242.
44. Ikada Y. Surface Modification of Polymers for Medi-cal Applications. Biomaterials. 1994; 15: 725-736. 45. Tziampazis E, Kohn J, Moghe PV. PEG-variant biomaterials as selectively adhesive protein templates: model surfaces for controlled cell adhesion and migra-tion. Biomaterials. 2000; 21: 511-520.
46. Eriksson C. Bone morphogenesis and surface charge. Clin Orthop. 1976; 121: 295-302.
47. Bačáková L, Filová E, Rypáček F, Svorčík V, Starý V. Cell Adhesion on Artificial Materials for Tissue Engineer-ing. Physiol Res. 2004; 53: S35-S45.
48. Toquet J, Rohanizadeh R, Guicheux J, Couillaud S, Passuti N, Daculsi G, et al. Osteogenic potential in vitro of human bone marrow cells cultured on macroporous biphasic calcium phosphate ceramic. J Biomed Mater Res. 1999; 44: 98-108.
49. Ohgushi H, Miyake J, Tateishi T. Mesenchymal stem cells and bioceramics: Strategies to regenerate the skel-eton. Novartis Found Symp. 2003; 249: 118-132. 50. Fischer EM, Layrolle P, Van Blitterswijk CA, De Bru-ijn JD. Bone formation by mesenchymal progenitor cells cultured on dense and microporous hydroxyapatite par-ticles. Tissue Eng. 2003; 9: 1179-1188.
51. Adams CS, Mansfield K, Perlot RL, Shapiro IM. Ma-trix Regulation of Skeletal Cell Apoptosis. Role of cal-cium and phosphate ions. J Biol Chem. 2001; 276(23): 20316-20322.
52. Eslaminejad MB, Mirzadeh H, Yossef Mohamadi Y, Nickmahzar A. Bone differentiation of marrow-derived mesenchymal stem cells using β-tricalcium phosphate-alginate-gelatin hybrid scaffolds. J Tissue Eng Regen Med. 2007; 1: 417-424.
53. Toshio H. Biodegradable polymers for biomedical uses. Prog Polym Sci. 1994; 19: 663-702.
54. Chen LJ, Wang M. Production and evaluation of bio-degradable composites based on PHB-PHV copolymer. Biomaterials. 2002; 23(13): 2631-2639.
55. Atala A. Engineering tissues, organs and cells. J Tis-sue Eng Regen Med. 2007;1(2): 83-96.
56. Wiesmann HP, Nazer N, Klatt C, Szuwart T, Meyer U. Bone tissue engineering by primary osteoblast-like cells in a monolayer system and 3-dimensional collagen gel. J Oral Maxillofac Surg. 2003; 61: 1455-1462. 57. Wahl DA, Czernuszka JT. Collagen-hydroxyapatite composites for hard tissue repair. Eur Cell Mater. 2006; 11: 43-56.
58. Chevallay B. Herbage D.Collagenbased. biomateri-als as 3D scaffold for cell cultures: applications for tis-sue engineering and gene therapy. Med Biol Eng Com-put. 2000; 38: 211-218.
59. Niemeyer P, Krause U, Punzel M, Fellenberg J, Si-mank HG. Mesenchymal stem cells for tissue engineer-ing of bone: 3Dcultivation and osteogenic differentiation on mineralized collagen. Z Orthop Ihre Grenzgeb. 2003; 141: 712-717.
60. Rebaudi A, Silvestrini P, Trisi P. Use of a resorbable hydroxyapatite-collagen chondroitin sulfate material on immediate postextraction sites: A clinical and histologic study. Int J Periodontics Restorative Dent. 2003; 23: 371-379.
61. Hu YY, Zhang C, Lu R, Xu JQ, Li D. Repair of ra-dius defect with bone-morphogenetic-protein loaded hydroxyapatite/ collagen-poly(L-lactic acid) composite. Chin J Traumatol. 2003; 6: 67-74.
62. Liu G, Hu YY, Yan YN, Xiong Z, Wang Z, Lu R, et al. Effects of collagen I coating on the porous poly-lacti-deco-glycolid on adhesion, proliferation, and differentia-tion of mesenchymal stem cells. Zhonghua Yi Xue Za Zhi. 2003; 83: 580-583.
63. Wikesjo UM, Qahash M, Thomson RC, Cook AD, Rohrer MD, Wozney JM, et al. Space-providing expand-ed polytetrafluoroethylene devices define alveolar aug-mentation at dental implants induced by recombinant human bone morphogenetic protein 2 in an absorbable collagen sponge carrier. Clin Implant Dent Relat Res. 2003; 5: 112-123.
64. Eslaminejad MB, Mirzadeh H, Nickmahzar A, Moha-madi Y, Mivehchi H. Type I collagen gel in seeding me-dium improves murine mesencymal stem cell loading onto the scaffold, increases their subsequent prolifera-tion and enhances the culture mineralizaprolifera-tion. J Biomed Mater Res B Appl Biomater. 2009; 90: 659-667.
65. Sasaki T, Watanabe C. Stimulation of osteoinduc-tion in bone wound healing by high-molecular hyaluron-ic acid. Bone. 1995; 16: 9-15.
66. Pohunkova H, Stehlik J, Vachal J, Cech O, Adam M. Morphological features of bone healing under the effect of collagen-graft-glycosaminoglycan copolymer sup-plemented with the tripeptide Gly-His-Lys. Biomaterials. 1996; 17: 1567-1574.
mouse intramembranous osteogenesis in vitro. Cell Tis-sue Res. 1998; 294: 323-333.
68. Rhodes NP, Srivastava JK, Smith RF, Longinotti C. Metabolic and histological analysis of mesenchymal stem cells grown in 3-D hyaluronan-based scaffolds. J Mater Sci Mater Med. 2004; 15: 391-395
69. Farrell E, O'Brien FJ, Doyle P, Fischer J, Yannas I, Harley BA, et al. A collagen-glycosaminoglycan scaffold supports adult rat mesenchymal stem cell differentiation along Osteogenic and chondrogenic routes. Tissue Eng. 2006; 12: 459-468.
70. Mongiat M, Fu J, Oldershaw R, Greenhalgh R, Gown AM, Iozzo RV. Perlecan protein core interacts with extra-cellular matrix protein 1 (ECM1), a glycoprotein involved in bone formation and angiogenesis. J Biol Chem. 2003; 278: 17491-17499.
71. Rezwana K, Chena QZ, Blakera JJ, Boccaccinia AR. Biodegradable and bioactive porous polymer/inorganic composite scaffolds for bone tissue engineering. Rev Biomaterials. 2006; 27: 3413-3431.
72. Newman KD, McBurney MW. Poly (D, L lactic-co-glycolic acid) microspheres as biodegradable microcar-riers for pluripotent stem cells. Biomaterials. 2004; 25: 5763-5771.
73. Cao T, Ho KH, Teoh SH. Scaffold design and in vitro study of osteochondral coculture in a three-dimensional porous polycaprolactone scaffold fabricated by fused deposition modeling. Tissue Eng. 2003; 9 :S103-S112. 74. Nuttelman CR, Mortisen DJ, Henry SM, Anseth KS. Attachment of fibronectin to poly(vinyl alcohol) hydro-gels promotes NIH3T3 cell adhesion, proliferation, and migration. J Biomed Mater Res. 2001; 57: 217-223. 75. Kitamura S, Ohgushi H, Hirose M, Funaoka H, Takakura Y, Ito H. Osteogenic differentiation of human bone marrowderived mesenchymal cells cultured on alu-mina ceramics. Artif Organs. 2004; 28: 72-82.
76. Peppas NA, Langer R. New challenges in biomateri-als. Science. 1994; 263(5154): 1715-1720.
77. Nejati E, Firouzdor V, Eslaminejad MB, Bagheri F. Needle-like nano hydroxyapatite/poly(l-lactide acid) composite scaffold for bone tissue engineering applica-tion. Mater Sci Eng C. 2009; 29: 942-949.
78. Bryant SJ, Nuttelman CR, Anseth KS. The effects of crosslinking density on cartilage formation in photo-crosslinkable hydrogels. Biomed Sci Instrum. 1999; 35: 309-314.
79. Smidsrød O, Skjåk-Braek G. Alginate as immobiliza-tion matrix for cells. Trends Biotechnol. 1990 ;8(3): 71-78.
80. Sharma B, Elisseeff JH. Engineering structurally organize cartilage and bone tissues. Ann Biomed Eng. 2004; 32: 148-159.
81. Rose FR, Oreffo RO. Bone tissue engineering: hope vs hype. Biochem Biophys Res Commun. 2002 ; 292(1): 1-7.
82. Jadlowiec JA, Celil AB, Hollinger JO. Bone tissue engineering: recent advances and promising therapeutic agents. Expert Opin Biol Ther. 2003; 3(3): 409-423. 83. Reddi AH. Bone morphogenetic proteins: an uncon-ventional approach to isolation of first mammalian mor-phogens. Cytokine Growth Factor Rev. 1997; 8: 11-20. 84. Wozney JM. The bone morphogenetic protein family and osteogenesis. Mol Reprod Dev. 1992; 32: 160-167. 85. Lind M, Bünger C. Factors stimulating bone
forma-tion. Eur Spine. J(2001); 10: S102-S109.
86. Ramoshebi LN, Matsaba TN, Teare J, Renton L, Patton J, Ripamonti U. Tissue engineering: TGF-β su-perfamily members and delivery systems in bone regen-eration. Expert Rev Mol Med. 2002; 4: 1-11.
87. Cheng H, Jiang W, Phillips FM, Haydon RC, Peng Y, Zhou L, et al. Osteogenic activity of the fourteen types of human bone morphogenetic proteins (BMPs). J Bone Joint Surg Am. 2003; 85: 1544-1552.
88. Dimitriou R, Dahabreh Z, Katsoulis E, Matthews SJ, Branfoot T, Giannoudis PV. Application of recombinant BMP-7 on persistent upper and lower limb nonunions. Injury. 2005; 36: S51-59.
89. Murnaghan M, McIlmurray L, Mushipe MT, Li G. Time for treating bone fracture using rhBMP-2: a randomised placebo controlled mouse fracture trial. J Orthop Res. 2005; 23: 625-631.
90. Gallea S, Lallemand F, Atfi A, Rawadi G, Ramez V, Spinella-Jaegle S, et al. Activation of mitogen-acti-vated protein kinase cascades is involved in regulation of bone morphogenetic protein-2-induced osteoblast differentiation in pluripotent C2C12 cells. Bone. 2001; 28(5): 491-498.
91. Colton CK. Implantable biohybrid artificial organs. Cell Transplant. 1995; 4: 415-436.
92. Wong C, Inman E, Spaethe R, Helgerson S. Fibrin-based biomaterials to deliver human growth factors. Thromb Haemost. 2003; 89: 573-582.
93. Kirker-Head CA. Potential applications and delivery strategies for bone morphogenetic proteins. Adv Drug Deliv Rev. 2000; 43: 65-92.
94. Rabbany SY, Heissig B, Hattori K, Rafii S. Molecu-lar pathways regulating mobilization of marrow-derived stem cells for tissue revascularization. Trends Mol Med. 2003; 9(3): 109-117(9).
95. Yu X, Botchwey EA, Levine EM, Pollack SR, Lau-rencin CT. Bioreactor-based bone tissue engineering: The influence of dynamic flow on osteoblast phenotypic expression and matrix mineralization. Proc Natl Acad Sci USA. 2004;101(31): 11203-11208.
96. Sikavitsas VI, Bancroft GN, Mikos AG. Formation of three-dimensional cell/polymer constructs for bone tis-sue engineering in a spinner flask and a rotating wall vessel bioreactor. J Biomed Mater Res. 2002; 62:136-148.
97. Wiesmann H, Joos U, Meyer U. Biological and bio-physical principles in extracorporal bone tissue engi-neering. Part II. Int J Oral Maxillofac Surg. 2004; 33: 523-530.
98. Franceschi RT, Xiao G. Regulation of the osteoblast-specific transcription factor, Runx2: responsiveness to multiple signal transduction pathways. J Cell Biochem. 2003; 88(3): 446-454.
99. Martin I, Wendt D and Heberer M. The role of biore-actors in tissue engineering. Trends Biotechnol. 2004; 22(2): 80-86.
100. Bancroft GN, Sikavitsas VI, Mikos AG. Design of a flow perfusion bioreactor system for bone tissue-engi-neering applications. Tissue Eng. 2003; 9: 549-554. 101. Sikavitsas VI, Bancroft GN, Holtorf HL, Jansen JA, Mikos AG. Mineralized matrix deposition by marrow stromal osteoblasts in 3D perfusion culture increases with increasing fluid shear forces. Proc Natl Acad Sci USA. 2003; 100: 14683-14638.
102. Khademhosseini A, Langer R, Borenstein J, Vacan-ti JP. Microscale technologies for Vacan-tissue engineering and biology. PNAS. 2006; 103: 2480-2487.
103. Langer R. Selected advances in drug delivery and tissue engineering. J Control Release. 1999; 62: 7-11. 104. Ueda H, Hong L, Yamamoto M, Shigeno K, Inoue M, Toba T, et al. Use of collagen sponge incorporating transforming growth factor-beta1 to promote bone Use of collagen sponge incorporating transforming growth factor-beta1 to promote bone repa. Biomaterials. 2002; 23: 1003-1010.
105. Park YJ, Lee YM, Park SN, Sheenb SY, Chungb CP, Lee SJ. Platelet derived growth factor releasing chi-tosan sponge for periodontal bone regeneration. Bioma-terials. 2000; 21:153-159.
106. Marler JJ, Upton J, Langer R, Vacanti JP. Trans-plantation of cells in matrices for tissue regeneration. Adv Drug Deliver Rev. 1998; 33: 165-182.
107. Meyer U, Joos U, Wiesmann HP. Biological and biophysical principle in extracorporal bone tissue en-gineering. Part I. Int J Oral Maxillofac Surg. 2004; 33: 325-332.
108. Tsuchiya K, Mori T, Chen G, Ushida T, Tateishi T, Matsuno T, et al. Custom-shaping system for bone re-generation bye seeding marrow stromal cells onto a web like biodegradable hybrid sheet. Cell Tissue Res. 2004; 316: 141-153.
109. Bruder SP, Kraus KH, Goldberg VM, Kadiyala S. The effect of implants loaded with autologous mesen-chymal stem cells on the healing of canine segmental bone defects. J Bone Joint Surg Am. 1998; 80(7): 985-996.
110. Kon E, Muraglia A, Corsi A, Bianco P, Marcacci M, Martin I, et al. Autologous bone marrow stromal cells loaded onto porous hydroxyapatite ceramic accelerate bone repair in critical-size defects of sheep long bones. J Biomed Mater Res. 2000; 49(3): 328-337.
111. Eslaminejad MB, Jafarian M, Khojasteh A, Mash-hadi Abbas F, Dehghan MM, Houshmand B. Enhancing ectopic bone formation in canine masseter muscle by loading mesenchymal stem cells onto natural bovine bone minerals. Iranian J Vet Surg. 2007; 2(4): 25-35.
112. Eslaminejad MB, Jafarian M, Khojasteh A, Mash-hadi Abbas F, Dehghan MM, Hassanizadeh R. In vivo Bone Formation by Canine Mesenchymal Stem Cells Loaded onto HA/TCP Scaffolds: Qualitative and Quanti-tative Analysis. Yakhteh. 2008; 10(3): 205-212.
113. Khojasteh A, Eslaminejad MB, Nazarian H. Mes-enchymal stem cells enhance bone regeneration in rat calvarial critical size defects more than platelete-rich plasma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 106(3): 356-362.
114. Jafarian M, Eslaminejad MB, Khojasteh A, Mash-hadi Abbas F, Dehghan MM, Hassanizadeh R, et al. Marrow-derived mesenchymal stem cells-directed bone regeneration in the dog mandible: a comparison between biphasic calcium phosphate and natural bone mineral. 2008; 105: e14-e24.
115. Quarto R, Mastrogiacomo M, Cancedda R, Kutepov SM, Mukhachev V, Lavroukov A, et al. Repair of large bone defects with the use of autologous bone marrow stromal cells. N Engl J Med. 2001; 344(5): 385-386. 116. Gronthos S. Reconstruction of human mandible by tissue engineering. Lancet 2004; 364(9436): 735-736. 117. Mendes SC, Bezemer J, Claase MB, Grijpma DW, Bella G, Degli-innocenti F, et al. Evaluation of two bio-degradable polymeric systems as substrates for bone tissue engineering. Tissu Eng. 2003; 9: s91-s101. 118. Takahashi Y, Yamamoto M, Tabata Y. Osteogenic differentiation of mesenchymal stem cells in biodegrad-able sponges composed of gelatin and β-tricalcium phosphate. Biomaterials. 2005; 26: 3587-3596.
119. Wendt D, Marsano A, Jakob M, Heberer M, Mar-tin I. OscillaMar-ting perfusion of cell suspensions through three-dimensional scaffolds enhances cell seeding ef-ficiency and uniformity. Biotechnol Bioeng. 2003; 84: 205-214.
120. Godbey W, Hindy BSS, Sherman ME, Atala A. A novel use of centrifugal force for cell seeding into po-rous scaffolds. Biomat. 2004; 25: 2799-2805.