jcoloproctol(rioj).2016;36(3):173–175
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Idiopathic
megacolon
in
a
teenager
treated
by
laparoscopic
rectosigmoidectomy
夽
Carlos
Eduardo
Oliveira
Sodero
∗,
Emerson
Abdulmassih
Wood
da
Silva,
Dirceu
de
Castro
Rezende
Júnior,
Gustavo
Roberto
Carvalho
Tiveron,
Aurélio
Fabiano
Ribeiro
Zago,
Rafael
Andrade
de
Oliveira,
Bernardo
Rosa
e
Souza,
Luciano
Ricardo
Pelegrinelli
UniversidadeFederaldoTriânguloMineiro(UFTM),HospitaldeClínicas,Uberaba,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26March2015 Accepted11April2016 Availableonline27April2016
Keywords:
Megacolon Megarectum Duhamel
a
b
s
t
r
a
c
t
Chronicconstipationinchildrenandadolescentsisrelativelycommonandareasonfor consultation withpediatriciansandproctologists.Mostcasesrespondtomedical treat-ment.AdvancedcasesofmegacolonandmegarectumcanbetreatedsurgicallybyDuhamel technique.
Thiscasereportdescribesa15-year-oldpatientwithchronicintestinalconstipation refrac-torytoclinicaltreatmentassociatedwithmegacolonandmegarectum,whichwassurgically treated.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Megacolon
idiopático
em
adolescente
tratado
por
retossigmoidectomia
videolaparoscópica
Palavras-chave:
Megacolon Megarreto Duhamel
r
e
s
u
m
o
A constipac¸ãointestinal crônica em crianc¸aseadolescentes érelativamentecomum e motivode consultasa pediatrase coloproctologistas.Amaioriadoscasos respondeao tratamentoclínico.Casosavanc¸adosdemegacolonemegarretopodemsertratados cirur-gicamenteatravésdacirurgiadeDuhamel.
Esterelatodecasodescreveumpacientede15anosdeidadecomquadrodeconstipac¸ão intestinalcrônicarefratáriaaotratamentoclínicoassociadaamegacolonemegarreto,o qualfoitratadocirurgicamente.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
夽
StudyconductedatDisciplineofColoproctology,DepartmentofSurgery,HospitaldeClínicas,UniversidadeFederaldoTriângulo Mineiro(UFTM),Uberaba,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.E.O.Sodero).
http://dx.doi.org/10.1016/j.jcol.2016.04.002
174
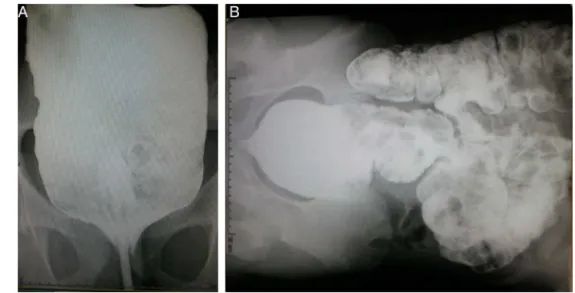
jcoloproctol(rioj).2016;36(3):173–175Fig.1–Bariumenema. Source:ProctologyService,HC-UFTM.
Introduction
Chronicconstipationinchildrenandadolescentsisrelatively commonandareasonforconsultationwithpediatriciansand proctologists.Therearenoformalstatisticsofthisdiseasein thisagegroup,butthiscomplaintcorrespondsto3–5%ofall pediatricconsultationsandto10–25%ofreferralsto gastroen-terologistsandproctologists.1
Morethan50%ofcasesusuallyhaveagoodresponseto clinicaltreatment, but ina minorityofpatients, the surgi-cal treatment is imperious(some casesof megacolon and megarectum).2
Case
presentation
Awhite,male,15-yearoldpatient(accompaniedbyanadult responsiblewoman)cametotheColoproctologyService out-patientclinic(HC-UFTM)complainingof“gettingconstipated since childhood.” The woman reported that since the age of4 the patient suffers from constipation that, on certain occasions,lastsforafullmonth(sic).Shealsoreportedthat sinceabout a year ago there is a frequentneed for “ene-mas” and denied other diseases, the use ofmedicines, or previous surgeries,and that socially the patient is“a very withdrawn boy.” During the physical examination of the patient’sabdomen,wecouldperceiveadistendedabdomen with a non-pulsatile, depressible, painless palpable mass in his left hemiabdomen. The proctological examination revealed a normotonic sphincter and a large amount of hardstoolsoccupyingthe rectum, aswell asa widerectal ampulla.
Thepatienthasundergoneabariumenema,whichshowed anadvancedmegacolonassociatedwithmegarectum(Fig.1A andB).
Theanorectalmanometryshowedcaudalmigrationofthe higher-pressurezone,thepresenceofananorectalinhibitory reflex,andhypertoniaoftheinternalanalsphincter.
NegativeserologyforChagasdisease
Fromthesedata,wehavesuggestedadiagnostichypothesis ofidiopathicmegacolonorHirschsprung’sdisease.
OnDecember5th,2014thepatientunderwentlaparoscopic rectosigmoidectomywitharetrorectal,low-colorectal anasto-mosiswithgoodpostoperativeevolution;hewasdischarged onDecember11th,2014.
Thepathology ofthe surgicalspecimenrevealed preser-vationofmyentericganglia,besidesmegacolon/megarectum. Inthepostoperativeoutpatientfollow-up,agoodprogression wasobserved,withafrequencyofdefecationof3/3dayswith normalconsistencystools.
Discussion
Chronic constipationis relatively common inchildren and adolescents,beingareasontoconsultationwithpediatricians andproctologists.Inadvancedcases,constipationis associ-atedwithpoorgrowth/developmentofthispopulation.3
Histological studies showed myenteric plexus denerva-tion inallcolonicsegments,asaresultofaninflammatory process.Thisprocessultimatelydestroys theganglioncells and generatesmotility changes,especially inthe sigmoid-rectoanal segment. This compromises the coordination of musclecontractionmovementsandhinderstheprogression andexpulsionofstools.4
Over 50% of cases respond to medical treatment. In a minorityofadvancedcasesofmegacolonandmegarectum, inwhichonecanseepoorgrowth/developmentofthepatient –andthereforeofhis/herqualityoflife,therewillbean indi-cationforsurgery(Duhamelanditsvariations).5
jcoloproctol(rioj).2016;36(3):173–175
175
In1963,BernardesandReisNeto&Cunhainconcurrent studiesintroduced bothinBraziland inLatinAmerica the ideaofusingtheDuhameltechniqueforsurgicaltreatment ofacquiredmegacolon.4
Theuseofmechanicalsuturing,whichobviatestheneed foraperinealcolostomy,providedthefinalelementstothe almost universal acceptanceof this technique,as the best currentlyproposedsurgicaltreatmentforthiscondition.4
The use of laparoscopy for the treatment of acquired megacolon, with the completion of the colon-rectum-anal anastomosis, has been introduced in 1994 and brought great benefits to the patient, particularly with respect to the period of hospitalization and a shorter recovery time postoperatively.4
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.FishmanLN,IsraelEJ.Anapproachtothechildwith constipation.SeminColonRectum.1994;5:116–23.
2.ClaydenGS.Managementofchronicconstipation.ArchDis Child.1992;67:340–4.
3.DiLorenzoC,FloresAF,ReddySN,SnapeWJJr,BazzocchiG, HymanPE.Colonicmanometryinchildrenwith
chronicintestinalpseudo-obstruction.Gut.1993;34: 803–7.
4.ReisNetoJA,PedrosoMA,LupinacciRA,ReisJuniorJÁ,Ciquini S,LupinacciRM,etal.MegacoloAdquirido-Perspectivas FisiopatológicasparaoTratamentoLaparoscópico.RevBras Coloproct.2004;24:49–62.