REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
In
vitro
evaluation
of
the
method
effectiveness
to
limit
inflation
pressure
cuffs
of
endotracheal
tubes
夽
Rafael
de
Macedo
Coelho
a,∗,
Thiago
Trigueiro
Morais
de
Paiva
a,
Ligia
Andrade
da
Silva
Telles
Mathias
b,caCentrodeensinoeTreinamento(CET),SantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil bFaculdadedeCiênciasMédicas,SantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
cDisciplineofAnesthesiologyandPain,SantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil
Received24April2014;accepted17June2014 Availableonline21January2016
KEYWORDS Method; Inflation; Cuffs; Tube; Pressure
Abstract
Backgroundandobjective: Cuffsoftrachealtubesprotectthelowerairwayfromaspirationof gastriccontentsandfacilitateventilation,butmaycausemanycomplications,especiallywhen thecuffpressureexceeds30cmH2O.Thisoccursinover30%ofconventionalinsufflations,so
itisrecommendedtolimitthispressure.Inthisstudyweevaluatedtheinvitroeffectiveness ofamethodoflimitingthecuffpressuretoarangebetween20and30cmH2O.
Method: Usinganadaptertoconnectthetested tubetotheanesthesiamachine,therelief valvewas regulatedto30cmH2O,inflating thecuffby operating therapid flowofoxygen
button.Therewere33trialsforeachtubeofthreemanufacturers,offivesizes(6.5---8.5),using threetimesinflation(10,15and20s),totaling1485tests.Afterinflation,thepressureobtained wasmeasuredwithamanometer.Pressure>30cmH2Oor<20cmH2Owereconsideredfailures.
Results:Therewereeightfailures(0.5%,95%CI:0.1---0.9%),withallbypressures<20cmH2O
andafter10sinflation(1.6%,95%CI:05---2.7%).Onefailureoccurredwitha6.5tube(0.3%, 95%CI:−0.3to0.9%),sixwith7.0tubes(2%,95%CI:0.4---3.6%),andonewitha7.5tube(0.3%, 95%CI:−0.3to0.9%).
Conclusion:Thismethodwaseffectiveforinflatingtrachealtubecuffsofdifferentsizesand manufacturers,limitingitspressuretoarangebetween20and30cmH2O,withasuccessrate
of99.5%(95%CI:99.1---99.9%).
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
夽 StudyconductedattheHospitalCentraldaIrmandadedaSantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](R.M.Coelho). http://dx.doi.org/10.1016/j.bjane.2014.06.012
PALAVRAS-CHAVE Método;
Insuflac¸ão; Balonetes; Cânulas; Pressão
Avaliac¸ãoin vitro daeficáciademétodoparalimitarapressãodeinsuflac¸ão dosbalonetesdascânulasendotraqueais
Resumo
Justificativaeobjetivo: Osbalonetesdascânulastraqueaisprotegemasviasaéreasinferiores da aspirac¸ãode conteúdo gástricoe facilitama ventilac¸ãopulmonar,mas podem provocar diversascomplicac¸ões,principalmentequandoapressãodobalonetesupera30cmH2O.Isto
ocorreemmaisde30%dasinsuflac¸õesconvencionais,sendorecomendadaalimitac¸ãodesta pressão.Nesteestudoavaliou-seinvitroaeficáciadeummétodoparalimitarapressãodos balonetesàfaixaentre20e30cmH2O.
Método: Utilizandoumadaptadorpara conectaracânula testadaao aparelhodeanestesia, regulou-seaválvulalimitadoradestea30cmH2O,insuflandoobalonetepormeiodo
aciona-mentodobotãodefluxorápidodeoxigênio.Realizaram-se33testesparacadacânuladetrês fabricantes,decincotamanhos(6.5a8.5),utilizandotrêstemposparainsuflac¸ão(10,15e20 segundos),totalizando1485testes.Terminadaainsuflac¸ão,mediu-seapressãoobtidacomum manômetro.Pressões>30cmH2Oou<20cmH2Oforamconsideradasfalhas.
Resultados: Ocorreramoitofalhas(0,5%;IC95%:0,1---0,9%),sendotodasporpressões<20cm H2Oeapósinsuflac¸õesde10segundos(1,6%;IC95%:0,5---2,7%).Umafalhaocorreucomcânula
6.5(0,3%;IC95%:−0,3---0,9%),seiscomcânulas7.0(2%;IC95%:0,4---3,6%),eumacomcânula 7.5(0,3%;IC95%:−0,3---0,9%).
Conclusão:Estemétodomostrou-seeficazparainsuflarosbalonetesdecânulastraqueaisde diferentes tamanhosefabricanteslimitandosuapressãoàfaixa entre20 e30cmH2O, com
incidênciadesucessode99,5%(IC95%:99,1---99,9%).
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
When high pressure and low volume (HPLV) or high vol-umeandlow pressure(HVLP)endotracheal tubecuffs are inflated,theyexertpressureonthetrachealwallandmay lead to mucosal ischemia. This is directly related to the occurrenceofcomplicationsinupto90%ofpatients, includ-ing discomfort, sore throat, granuloma formation in the vocal cords, hoarseness, and serious complications such as recurrent laryngeal nerve and vocal cords paralysis, bloody sputum, tracheal-esophageal fistula, and tracheal rupture.1---4
Thereareseveralmethodsforinjectingairintothe tra-cheal tube cuff. The gold standard method is the direct measurement of cuff pressure (Cpressure) with calibrated manometer,analog5ordigital,6andisrecommendedinadult
andpediatricpatients.5,7---9However,itsuseisnotroutinein
Brazil.
Theinjectionofairintothecuffwithasyringeisthemost usedmethod.Thismethodissimple,fast,andlowcost,but therelationshipbetweenthevolumeofinjectedairandthe resultingcuff-to-tracheal wallpressure(C---Tpressure)is non-linear,causingcuffdistentionin30---98%ofcases,7,8,10,11---13
depending on the population studied, endotracheal tube used,andtheclinicalcontext.14
Other methods to limit the C---Tpressure have been pro-posed,suchasthetechniquesofminimalocclusivevolume (MOV) and minimum leak technique (MLT), but without scientificconfirmationofclinicalbenefit.6Pressure
adjust-ment alternative techniques have been suggested or are
underdevelopment, usingmodified endotracheal tubes,15
specialsyringes,16 andhospitalequipmentavailableinthe
units,17---21 howeverwithout eliminatingtheneed for
addi-tionalequipment.
Whenthecircularsystemisusedasthepressuresourceto inflatethetrachealtubecuffs,itispossibletolimitthe max-imumpressureinthesystemthroughtheadjustablepressure relief valve (APRV), also called pop-off valve, making it impossiblefortheCPandC---Tpressurereachvalueshigherthan themaximum setbythe APRVadjustment.In ordertodo this,simplyadapttheoutputofthecircularsystemtothe Luer-typeentry ofthe endotracheal tube pilotballoon----a methodnotfoundinthescientificliterature.
The possibility of limitingthe pressure withinthe cuff tosafelevelsusingasimple,widelyavailable,andlowcost methodcanreducetheoccurrenceandmagnitudeofvarious complications,manyofthemserious.Thisissuemotivated thepresentstudydesignedtoevaluateaninvitroefficacyof endotrachealtubecuffinsufflationmethod,withthe inter-nalpressuresetbetween20and30cmH2O.
Method
Aninvitroexperimentalstudyoftheefficacyofamethod forendotracheal tubecuffinflatingwasperformed. Given thenatureof thisstudy,theassessment bytheInstitution ResearchEthicsCommitteewaswaived.
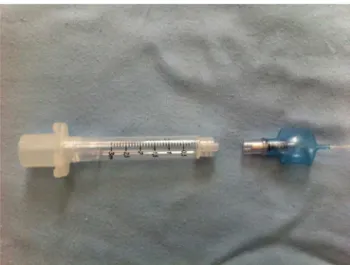
Figure1 Adapter usedto connect the anesthesiamachine circularsystemoutlettothetrachealtubepilotballoon.
insufflationis27---35%.8,11Confidenceintervalwascalculated
forthesuccessrateofeachendotrachealtubemodelofthe samemanufacturer, samesize(internal diameterin mm), and time of insufflation----time---diameter---manufacturer combination(TDM).Consideringasuccessrateof95%,total errorrate=15%,and95%confidencelevel,itwasobtained ann=32pergroup(TDMcombination).
Three different times (10, 15 and 20s) for the insuf-flation of endotracheal tubes of five different diameters (6.5,7.0, 7.5, 8.0 and8.5mm inner diameter)and three manufacturers(Dahlhausen,PortexandRüsch)weretested, resultingin45groups(differentTDMcombinations).Inorder toidentify possiblebiasescaused bythe different perfor-manceof each operator, or by thesame operator change inperformance due tomultiple repetitions oftests, each repetitionwasnumberedandperformedfollowingan estab-lishedsequence.Also,inordertoidentifyapossiblechange inperformanceduetoadefectiveendotrachealtube,three endotrachealtubesofthesamesizeandmanufacturerwere used,numbered1---3, and 11 insufflations weremade per tube,pertest,resultingin33testspergrouptotaling1485 tests.Forinsufflations lasting10s, the sequence oftubes was1,2and3;forinsufflationslasting15s,thesequenceof tubeswas3,1and2;andfor insufflationslasting20s,the sequenceoftubeswas2,3and1,sothatallofthe num-bered tubes were usedin all positions in the insufflation sequence.Moreover,the operatorstake turns,alternating theorderof insufflation, sothat each oneperformed 10, 15 or 20s insufflations with tubes of each size and each manufacturer.
The practical part wasperformed by two operators,a doctorspecialistinanesthesiology(Operator1),anda3rd year resident doctor in anesthesiology (Operator 2), both withpreviousexperienceof100repetitionseachinthe pro-posedinsufflationmethod.
To perform the coupling between the 15mm standard outletof the anesthesiamachine circularsystem andthe standardLuerconnectionofthetrachealtubepilotballoon, anadapter isrequired. Theadapter, madebythe investi-gatorhimselfusedastandard15mmAdamsconnectorofa 7.5endotrachealtube(internaldiameterinmm)toa3mL syringewithoutthe plunger (Fig.1).Thus,the anesthesia
machinecircularsystemisadaptedtothe15mmconnector, while the standard Luer-type connection of thesyringe is adaptedtotheendotrachealtubepilotballoon,openingits valvetoallowinsufflation.
TheanesthesiamachineusedforthetestswastheDräger FabiusGS®,whoseAPLvalvewassettothemaximum pres-sureof30cmH2Oandoxygenflowsetto10Lmin−1.Then, theadapterisconnectedtotheanesthesiamachine15mm outlet, andthe reservoirbag for ventilationis inflated by operatingthehigh-flowoxygenbutton.
Beforeeachinsufflation,themaximumairvolumeofeach tube cuffwasaspirated witha syringe.Then,theportion corresponding to the endotracheal tube cuff was placed insidea20mLsyringewithouttheplunger(of20mminternal diameter),fixedtothetesttablesurfacewithtape,keeping thecannulapassivelyrestingonitandalsofixedtothetable withtape.
One of the two operators spontaneously started each insufflation connecting the tracheal tube pilot balloon with the anesthesia machine through the adapter. After the predetermined timefor insufflation,the adapter was disconnected from the pilot balloon, interrupting the insufflation. Then, an aneroid manometer (Cuff Pres-sure Gauge, VBM Medizintechnik, Sula, Germany) was used tomeasure the pressure achievedwith the insuffla-tion.
Valuesbetween20and30cmH2Owereconsidered appro-priate,andvalueslessthan20cmH2Oorexceeding30cm H2O wereconsidered failures.Statisticalanalysiswas per-formed usingSPSS13.0 forWindows,with95% confidence intervals, andobtained dataonthe proportionof general failureandfailureforthefollowingvariables:manufacturer, size,insufflationtime,andoperator.
Results
All 1485 testswere performed withnotest discarded. Of the1485tests,1477(99.5%)hadpressuresconsidered ade-quate and eight tests failed (0.5%) (95% CI: 0.1---0.9%). All cases of failure occurred due to inappropriately low pressures.
Comparisonbetweenmanufacturers
Comparing the different manufacturers of the cannulas used,therewasnofailureintestswiththecannulas manu-facturedbyDahlhausen,6failures(1.2%)withthecannulas manufacturedbyPortex(95%CI:0.2---2.2%),and2failures (0.4%) withthe cannulas manufactured by Rüsch(95% CI:
−0.2to1.0%).
Comparisonbetweencannulas’sizes
Therewasonefailure(0.3%)withthe6.5mmcannula(95% CI:−0.3to0.9%),sixfailures(2.0%)withthe7.0mm
can-nula(95%CI:0.4---3.6%),onefailure(0.3%)withthe7.5mm cannula(95%CI:−0.3to0.9%),andnofailurewiththe8.0
Table1 Incidenceofgeneralfailureandforeachobserved variable(resultsexpressedin%and95%CI).
Variables Failure 95%CIlimits
Lower Upper
General 0.5% 0.1% 0.9%
Brand
Dahlhausen 0 0 0
Portex 1.2% 0.2% 2.2%
Rusch 0.4% −0.2% 1.0%
Size
6.5 0.3% −0.3% 0.9%
7.0 2.0% 0.4% 3.6%
7.5 0.3% −0.3% 0.9%
8.0 0.0% 0.0% 0.0%
8.5 0.0% 0.0% 0.0%
Time
10 1.6% 0.5% 2.7%
15 0.0% 0.0% 0.0%
20 0.0% 0.0% 0.0%
Operator
1 0 0 0
2 1.1% 0.3% 1.9%
Comparisonbetweentheinsufflationtimes
Alleightfailuresoccurredintubesinsufflatedfor10s(1.6%; 95% CI: 0.5---2.7%); therewas no failure with15 and 20s insufflations.
Comparisonbetweenoperators
Alleightfailuresoccurred withthe Operator2(1.1%;95% CI:0.3---1.9%).
Thegeneralandspecificfailureratiosforeachobserved variableareshowninTable1.
Discussion
Theincorporationofinflatablecuffstotrachealtubes rep-resented a huge technological advancement, promoting greater safety for patients and allowing the advance of pulmonary ventilation techniques.22,23 However, its use is
associatedwithseveralcomplicationsrelatedmainlytothe cuffhigh pressure(Cpressure).2,3,24 LimitingCpressure to30cm H2Osignificantlyreducesthecomplicationsassociatedwith theairway4,25;thus,theuseofamethodtolimitC
pressureis mandatory.7,26
ThegoldstandardmethodforCpressurecontrol,consisting of calibratedmanometers,5---7 enablescontinuous or
inter-mittent measurement of Cpresure in realtime, enabling to adjustitwithoutinterruptingthemeasurement.Amongits limitations arethe equipmenthigh cost andthe need for regular calibration. However, this method did not spread amonghealthprofessionals,particularlyamongphysicians, andisnotroutinelyusedafterorduringtrachealintubation maintenance.
Inthisstudy,weperformedan invitrotestofan alter-native method of tracheal tube cuff insufflation, limiting Cpresuretopressuresnotgreaterthan30cmH2O,anditwas notfound inthe literatureany publicationwiththesame orsimilarmethod.Also,forthisreasonthisstudywas ini-tiallycarriedoutinvitrototestthemethod’sfunctionality beforeexposingpatients toa technique without scientifi-callyproveneffects.
Inthisstudytherewereeightfailuresin1485tests(0.5%; 95%CI:0.1---0.9%),allduetoinappropriatelylowpressures. This represents an extremely small proportion of failure whenthisresultiscomparedwiththemostclinicallyused method----cuffinsufflation by injecting air from a syringe, that has a proportion of hyperinsufflation between 23.5% and64.5%ofcases,8,9,11,12andmayreachupto98%.13Among
these failures, six (75%) occurred in a single experiment (Portex tube, #7.0, 10s of insufflation, Operator 2), and theother twofailures in separate experiments (one with Rüschtube #6.5,10s of insufflation,Operator2, andone withRüschtube#7.5,10sofinsufflation,Operator2).
Despitetheexperimentaldesignofthisstudy,some varia-bles are impossible to control and may have contributed tothese failures. Among thesevariables are the nominal pressureofoxygennetwork,qualityoftrachealtubes man-ufacture,operatorperformance,andthecuff’srelationship withthebufferintheinsufflation.
The input pressure of the medical gases used in anesthesia equipment is maintained in the range of 4.5---5.5kgfcm−2.However,this pressureeventually shows
fluctuations,whichcanincreaseorreducetheflowof oxy-gen during the triggering of the high flux of O2 button, directly interferingin the cuffinsufflation processby the methodinthisstudy.
Regarding tracheal tubes construction pattern, small variationsinthecuffcompositionorformatchangethe elas-tance(pressure:volume ratio),witha directeffect on theobtainedresults.
Anotherfactor toconsideris the performance of each operator. Even applying the method with attention and technical accuracy, intra- and interpersonal variations in the process execution may interfere with the final pres-suremeasuredbyallowingthepilotballoonvalveopening and/or closing for times or at different times, uninten-tionallyaddingor removingacuffgasaliquot.Despitethe differenceof experiencebetween theoperatorswho per-formed the tests, both had the same degree of training inthismethod,havingperformedatleast100insufflations eachinapreviouspilotstudy.Therefore,thedifferent fail-ureincidencesbetweenoperatorsmaynotbeattributedto thedegreeofexperiencewiththismethod.However,small variationsinperformingthemethodcannotberuledoutas possiblecausesforthefailuresseenwithOperator2,albeit veryinfrequent(1.1%;95%CI:0.3---1.9%).
purpose,usingconcentrictubesmadeofpolyurethaneand latexthinmembranes,27 butitsmanufacturewouldrequire
complex laboratory resources, precluding its use in this work.
The choice of a 20mL syringe as a buffer wasdue to the fact that it was a rigid tube, easily found, low cost, withan internal diameter of 20mm----similarto the aver-ageinternal diameterofthe adultmaletrachea.Because theobjectiveof thisstudy wastoevaluate the effective-nessofamethodtolimitthepressurewithinthecuff,the buffer’sdiameterandcompliancedidnotneedtohavethe samecharacteristicsof thehumantrachea,since, regard-lessof these, the valveset to30cm H2O wouldlimit the pressureincreaseabovethis value.However,theuse ofa fixeddiameter bufferassociated withdifferentsizetubes may influence the method’s performance as the cuffs of smallertubesrequiremorevolumeandforagivenflowmore time,inordertoreachsufficientsize,soitswallscomein contactwiththe buffer andallowthe balanceof Cpressure. LargertubesreachthebalanceofCpressureinlesstime.This couldexplain why the failures occurred with the smaller tubesandintheshortestinsufflationtime,eventhoughwith verylowincidence.Thisproblemcouldbesolvedby keep-inginsufflation for a longertime or usinga smaller inner diameter buffer. However, it does not represent a disad-vantageofthismethodinclinicalpractice,asthepatient’s tracheainnerdiameterisnotamodifiablefactor,andmost oftenunknown.Thechoiceoftubesizetakesintoaccount thepatient’ssexandanthropometricdata(weight,height, larynxsize)andnaturallymaintainsthesizeratiobetween theouter diameterofthe chosencuff tube andtheinner diameterofthepatient’strachea,minimizingoreven elim-inatingthisproblem.However,clinicalstudiesareneededto proveit.
In an attempt to correlate some of these factors with theoccurredfailureepisodes,thetestswereconducted fol-lowingafixed andpre-establishedorder,accordingtothe sequencenumberofthethreetubes,ofeachsizeand man-ufacturer,numbered1---3.However,theincidenceoffailure in thisstudy wasquite small,not allowingits association withanyseen factors.Alleightfailuresoccurred withthe shortestinsufflationtime(10s)andasingleoperator (Oper-ator2),withsixofthem(75%)inasingleexperiment(Portex tube,#7.0,threefailureswithtube#1,twowith#2,andone withtube#3.Onecannotsaythatthesefailuresfoundinthis particularexperimentareduetotheshorttimeto insuffla-tion,oruncontrolledfactorssuchasthosementionedabove. Possibly,thesefailuresdonotresultfromhumanerror,asthe Operator2showedextremelylowfailurerateofonly1.1% (95%CI:0.3---1.9%).Norofshorttimetoinsufflation,since despiteallthefailureshaveoccurredintubesinflated for 10s theproportionoffailuresin thisgroupwas1.6%(95% CI:0.5---2.7%),withmeanpressurevaluessimilartothoseof otherinsufflationtimes(10s:24.30cmH2O;15s:25.77cm H2O;20s:25.35cmH2O).
Whatisstatedintheprecedingparagraphsmayexplain thepressuredifferencesseenaftersamesizetubes insuffla-tion,usingthesamemethod.Theexistenceofsuchvariables beyondtheproposedmethodcontroldoesnotdiminishthe datavalue,asthesamevariableswillbefoundinother con-textsandwillsimilarlyinfluencetheresultofapplyingthis methodinclinicalstudiesoreveninclinicalpractice.
Amongthe limitationsof theproposed methodmaybe mentionedthatitdoes notcompletelypreventthe under-pressurizationofcuffs,althoughrarely,anddoesnotallow pressuremeasurementanditssetting,allowingonlytolimit ittothemaximumvalueconsideredsafe.Itsuseisalsonot possibleinanesthesiamachineswithoutgradedAPRVandis inadvisableincaseswhereitisnotpossibletomeasurethe circularsystempressureduetothefailureofAPRV commu-nication withthe machine manometer, asin machines of lowerstandardquality.
The fact that there have been no failures related to inappropriately high pressures (greater than 30cm H2O) demonstrates that this method,while effectively limiting thecuffpressure,maybeusefultoreduceinjuriesrelated tomucosalandother airwaystructurecompression bythe cuffs. Other studies, in clinical settings and with other devicesbearinginflatablecuffs,suchastracheotomytubes, supraglotticairwaydevices,anddouble-lumentubes,should beconductedinordertodemonstratethepracticaluseand possiblebenefitsofthismethod.
Conclusion
Theproposedandappliedmethodinthisstudywaseffective toinsufflateinvitrothetrachealtubecuffsofdifferentsizes andmanufacturers,limitingitsinternalpressuretoarange between20and30cmH2O.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Estebe J-P, Delahaye S, Le Corre P. Alkalinization of intra-cuff lidocaine and use of gel lubrication protect against tracheal tube-inducedemergencephenomena. Br JAnaesth. 2004;92:361---6.
2.Kaneda N, Goto R, Ishijima S, et al. Laryngeal granuloma causedbyshort-termendotrachealintubation.Anesthesiology. 1999;90:1482---3.
3.Audu P, Artz G, Scheid S, et al. Recurrent laryngeal nerve palsy after anterior cervical spine surgery. Anesthesiology. 2006;105:898---901.
4.Liu J, Zhang X, Gong W, et al. Correlations between controlled endotracheal tube cuff pressure and postpro-cedural complications: a multicenter study. Anesth Analg. 2010;111:1133---7.
5.BlanchPB.Laboratoryevaluationof4brandsofendotracheal tubecuffinflator.RespirCare.2004;49:166---73.
6.Crimlisk JT,Horn MH,Wilson DJ, et al. Artificial airways: a survey of cuff management practices. Heart Lung. 1996;25: 225---35.
7.Galinski M, Tréoux V, Garrigue B, et al. Intracuff pressures of endotracheal tubes in the management of airway emer-gencies: theneed for pressure monitoring. AnnEmerg Med. 2006;47:545---7.
8.SenguptaP,SesslerDI,MaglingerP,etal.Endotrachealtubecuff pressureinthreehospitals,andthevolumerequiredtoproduce anappropriatecuffpressure.BMCAnesthesiol.2004;4:8---13. 9.TobiasJD,SchwartzL,RiceJ,etal.Cuffedendotrachealtubes
10.DobrinPB,GoldbergEM,CanfieldTR.Theendotrachealcuff:a comparativestudy.AnesthAnalg.1974;53:456---60.
11.ChapmanJ,PallinD,FerraraL,etal.Endotrachealtubecuff pressuresinpatientsintubatedbeforetransport.AmJEmerg Med.2009;27:980---2.
12.FeltenML,Schmautz E,Delaporte-CerceauS,etal. Endotra-chealtube cuffpressureis unpredictableinchildren.Anesth Analg.2003;97:1612---6.
13.Bassi M, Zuercher M, Erne JJ, et al. Endotracheal tube intracuffpressureduringhelicoptertransport.AnnEmergMed. 2010;56:89---93,e1.
14.YildirimZB,UzunkoyA,CigdemA,etal.Changesincuffpressure ofendotrachealtubeduringlaparoscopicandopenabdominal surgery.SurgEndosc.2012;26:398---401.
15.Stanley TH, Foote JL, Liu WS. A simple pressure relief valve to prevent increases in endotracheal tube cuff pres-sureandvolumeinintubatedpatients.Anesthesiology.1975;43: 478---81.
16.Slocum AH Jr, Slocum AH Sr, Spiegel JE. Technical commu-nication: design and in vitro testing of a pressure-sensing syringefor endotrachealtubecuffs.AnesthAnalg.2012;114: 967---71.
17.KimJM.Thetrachealtubecuffpressurestabilizerandits clini-calevaluation.AnesthAnalg.1980;59:291---6.
18.GravensteinN,Burwick N.Recoilofinflation syringeplunger limitsexcessiveendotrachealtubecuffpressure. Anesthesiol-ogy.1988;69:A730[Abstract].
19.DoyleDJ.Digitaldisplay ofendotrachealtube cuffpressures madesimple.Anesthesiology.1999;91:329.
20.ResnikoffE,KatzJA.Amodifiedepiduralsyringeasan endo-tracheal tubecuffpressure-controlling device.AnesthAnalg. 1990;70:208---11.
21.LenoirRJ.Venouscongestionoftheneck;itsrelationto laryn-gealmaskcuffpressures.BrJAnaesth.2004;93:476---7. 22.MillerRA.Anewlaryngoscope.Anesthesiology.1941;2:317---20. 23.SpiegelJE.Endotrachealtubecuffs:designandfunction.
Anes-thesiolNews.2010;36:51---8.
24.Nordin U. The trachea and cuff-induced tracheal injury:an experimentalstudyoncausativefactorsandprevention.Acta OtolaryngolSuppl.1977;345:1---71.
25.CombesJ,SchauvliegeF,PeyrousetO,etal.Intracuffpressure andtrachealmorbidity:influenceoffillingcuffwithsaline dur-ingnitrusoxideanesthesia.Anesthesiology.2001;95:1120---4. 26.Lewis FR, Schlobohm RM, Thomas AN. Prevention of
complications from prolonged tracheal intubation. Am J Surg.1978;35:452---7.