PROFILE OF SPINAL TRAUMA IN KASHMIR
Mudasir Habib1, Muzefer Ahmad Ahanger2, Tarooq Ahmad Reshi3, Abdul Rashid Bhat4,
Shahnawaz Mansoor5, Mushtaq Ahmad Rather6
HOW TO CITE THIS ARTICLE:
Mudasir Habib, Muzefer Ahmad Ahanger, Tarooq Ahmad Reshi, Abdul Rashid Bhat, Shahnawaz Mansoor, Mushtaq Ahmad Rather. ”Profile of Spinal Trauma in Kashmir”. Journal of Evidence based Medicine and Healthcare; Volume 2, Issue 31, August 03, 2015; Page: 4548-4554, DOI: 10.18410/jebmh/2015/641
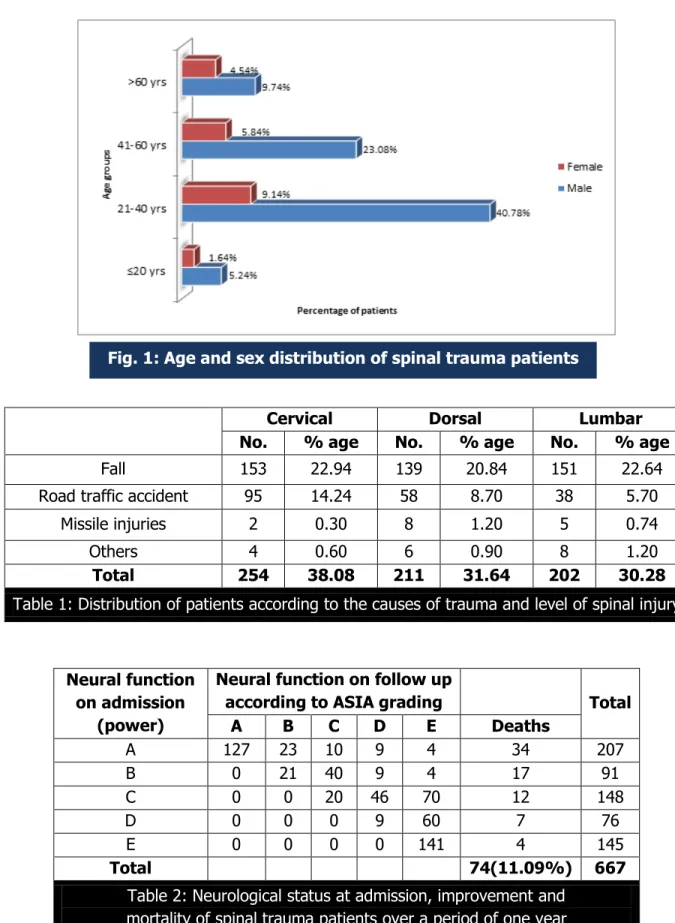
ABSTRACT: INTRODUCTION: Spinal cord injury is a devastating condition that affects all regions of the world. A high incidence of spinal cord injury in younger populations has resulted in enormous financial and physical costs for individual and the society. AIMS: The aim of this study was to know the epidemiological and clinico-radiological features of spinal trauma, analyse the diagnostic tools and to reveal the outcome of spinal trauma. METHODS: This was a retro-prospective hospital based study. All patients of spinal trauma admitted in the department of Neurosurgery SKIMS, Srinagar from September 2003 to October 2013 were taken up for the study. RESULTS: A total of 667 cases of spinal trauma were reported from September 2003 to October 2013. 526 were males and 141 were females. The most prevalent age group was 21-40 years (49.93%). Most common mode of injury was fall from height (66.41%), followed by Road traffic accidents (28.63%). 38.08% had cervical, 31.64% had dorsal and 30.28% had lumbar spine injury. Trauma was most common in the month of August and was mainly due to fall from height. 69.61% patients were managed surgically and 30.58% conservatively. 41.22% patients showed improvement in neurological grade, 20.68% made complete recovery, 26.53% showed no neurological improvement. CONCLUSION: Spinal trauma occurs most commonly in young productive age group. Fall from height is the most common cause of injury. CT and MRI are complementary to each other in diagnosis. Initial neurological grade is most important prognostic factor.
KEYWORDS: Spinal trauma, Neurological, Cervical, Dorsal, Lumbar spine injury.
INTRODUCTION: Spinal cord injury (SCI) is a devastating and debilitating condition that affects all regions of the world.(1) Motor vehicle accidents, falls, sports and the penetrating wounds
(Gunshot/missile injuries) being the most common mechanisms of injury, with young population being commonly involved.(2-5) The cause of spinal injury varies with age, and particularly sex, with
males being three to four times as likely to sustain an injury as female. The high incidence of spinal cord injury in younger populations has resulted in enormous financial and physical costs for individual and the society.(6) Significant variation in prevalence in spinal cord injury exists among
geographic locales, so these data are paramount for the local and regional health care functioning. An understanding of the prevalence of spinal cord injury is essential for planning cost–effective care and for developing preventive strategies. SCI patients often require extended treatment in an intensive care unit.(7) With improvements in imaging techniques and our
understanding of the primary and secondary mechanisms of spinal cord injury,(8,9) there is
epidemiology and outcome of spinal trauma, so to guide for prevention, treatment and rehabilitation provide the basis for this study.
AIMS:
To know the epidemiological and clinico-radiological features of spinal trauma in Kashmir.
To reveal the outcome of spinal trauma.
METHODS: We analysed all the patients of spinal trauma admitted in the department of Neurosurgery SKIMS, Srinagar during 10 consecutive years from 2003 to 2013. SCI was diagnosed using clinical methods, Plain X- rays, CT scans and MRI. The Neurologic level and extent of injury were defined using the international standards set forth by the American Spinal Injury Association (ASIA). 463 patients were operated, and the types of surgical procedures used were as follows: decompressive corpectomy and inter-body fusion/fixation, non-decompressive posterior trans-pedicular fixation, decompressive laminectomy and laminotomy. 204 patients were managed conservatively. The patients were assessed at different intervals of time using ASIA grading. The final observations were considered at one year after the injury. The results were compiled and analysed using statistical law of variance.
Cervical Dorsal Lumbar No. % age No. % age No. % age
Fall 153 22.94 139 20.84 151 22.64
Road traffic accident 95 14.24 58 8.70 38 5.70
Missile injuries 2 0.30 8 1.20 5 0.74
Others 4 0.60 6 0.90 8 1.20
Total 254 38.08 211 31.64 202 30.28
Table 1: Distribution of patients according to the causes of trauma and level of spinal injury
Neural function on admission
(power)
Neural function on follow up
according to ASIA grading Total A B C D E Deaths
A 127 23 10 9 4 34 207
B 0 21 40 9 4 17 91
C 0 0 20 46 70 12 148
D 0 0 0 9 60 7 76
E 0 0 0 0 141 4 145
Total 74(11.09%) 667
Table 2: Neurological status at admission, improvement and mortality of spinal trauma patients over a period of one year
DISCUSSION: Spinal cord injury (SCI) is a catastrophic event that results in impairments that affects almost every aspect of a person’s bodily function. Spinal cord injury is virtually unmatched in the level of devastation it brings to a person’s personal, social and economic aspects of life. Egyptian physicians long ago labelled SCI as an ailment not to be treated at all. However, advances in treatment that began during the World War II and have progressed since allowed many persons with SCI to live much longer. Today in many cases, patients with SCI can expect to live an almost normal lifespan.
A total of 667 of spinal trauma were admitted in the department of Neurosurgery SKIMS, Srinagar in 10 years, with no apparent change detected over a decade. A preponderance of males over females was found in our study with males numbering 526 and females 141, with male/ female ratio of 3.7 to 1 which is comparable to other studies.(10)
Commonest age group involved were young adults between the 21 and 40 years of age in both males and females. It is these young people who are the most active part of the society, therefore exposed to the factors that lead to this devastating condition, which is similar to the other reports.(11,12)
Although many cases of spinal cord injury shows geographical variation, Literature from developed countries, report that Road traffic accidents account for the maximum number of spinal injuries.(13) However in our region we found that mostly the injuries are due to fall from
trees, mountain slopes, roofs, electric poles (66.41%) and Road traffic accidents account for (28.63%) of cases. Falls were the most common cause and that most of the spinal trauma cases occur in autumn and summer seasons. This can be explained on the basis that during these months, Walnuts are harvested in Kashmir. Walnut tree is very tall tree and is grown mostly in rural areas. Its branches are very long. The persons harvesting the walnuts additionally carry a stick in their hands for harvesting the walnuts which makes them unstable and these trees become very slippery due to rain. Moreover most of the construction work in Kashmir is carried out during these months. That is why falls are most common in autumn and summer and more common in rural areas.
In our study 38.08% of cases had cervical trauma, followed by 31.64% having involvement of dorsal spine and 30.28% having involvement of lumbar spine. Overall the cervical region was involved in majority of the patients than the dorsal and lumbar, but the percentage found was slightly lower than found in most of the other studies. This can be explained by the etiology of the spinal trauma, as fall from height is the most common cause here. It was noted in our study that fall from height was more likely to injure the lumbar spine, whereas fall and road traffic accident contributed to more cervical spine injuries. These observations are similar to those reported in a previous study by Jackson et al.(14) Cars and buses in Kashmir do not always have
safety mechanisms to decrease the effects of whiplash injuries. This is one of the reason that cervical injuries are more common in Road traffic accidents.
Agarwal P et al(15) in their study observed ratio of male to female who sustained spinal
Schizas C et al(16) impressed that surgical indications in spinal trauma remains a
controversial topic. In general, unstable cervical injuries such as displaced odontoid fracture, burst fracture or tear drop fracture require surgical intervention. The lumbodorsal compression injuries without posterior wall involvement or significant kyphosis can be treated conservatively. Surgery is indicated in fracture- dislocations and burst fractures with significant canal narrowing and/or major khyphosis.
Various surgical approaches were used in our study. For cervical spine, Anterior cervical approach was used in 68 patients, for cervico-dorsal junction (C7-D2), lateral clavico-sternotomy approach was used in 14 patients. At SKIMS, indigenous and special technique of Trans-axillary approach (through axillary pit between 2nd and 3rd ribs) was used in 16 patients and was used to
decompress the D2, 3 vertebral fractures. The Modified postero-lateral Trans –thoracic Trans-pleural approach was used for the dorsal bodies of third to eleventh vertebrae. The dorso-lumbar junction (D12-L1) and lumbar 2nd and 3rd bodies were approached through Modified
postero-lateral Extra-pleural Retro-peritoneal approach.(17)
In our study we found that the initial neurological deficit was the most important factor for the outcome of these patients, patients with incomplete injury at admission had good recovery and patients with complete injury at admission had poor outcome.
No patient was made worse as a result of surgery. 275(41.22%) patients improved their neurological grade. 138 (20.68%) patients made complete recovery; most of these patients had grade C and grade D injury at admission. Four patients improved from grade “A” at admission to grade “E”, and 177(26.53%) patients had no neurological improvement. In our study we had a mortality of 11.09%, the mortality was more in patients who had a complete type of injury and more in cervical trauma cases.
Pickett GE et al(18) reported in-hospital mortality of 8% and was significantly higher in
elderly.
B Silberstein, S Rabinovich(19) reported a mortality of 16.8% and most of the patients who
died (84.8%) had injuries of the cervical spinal cord at the level of C4 and above.
The conservatively managed patients were put on prolonged bed rest needed for consolidation and stabilization of spine, and as a result percentage of complications (pressure sores, infections of respiratory and urinary tract) was high as compared to surgically treated patients. We noticed in our study that patients who were operated had less hospital stay, were mobilized early and had faster neurological recovery than the conservatively treated patients.
Kormas et al(20) found that the patients of surgical group had fever complications and a
shorter hospital stay than the patients in the conservative group, same findings were observed in our study.
Mc lain RF, Burlcus JK et al(21) found that surgical instrumentation allowed immediate
mobilization of severely injured patients, reducing thromboembolic and pulmonary complications and reducing overall morbidity and mortality.
REFERENCES:
1. Ackery A, Tator C, Krassioukov A. A global perspective on spinal cord injury epidemiology. J Neurotrauma. 2004; 21(10): 1355–1370.
2. Bhatoe H S, Singh P. Missile injuries of the spine. Neurol India 2003; 51: 507-11.
3. Bohlman H, Boada E. Fractures and dislocations of lower cervical spine. In: Cervical spine research society (ed.).The cervical spines Philadelphia: Lippincott; 1983: 232-67.
4. Sonntag V, Hadley M. Management of upper cervical instability. Willkins R(ed.) Neurosurgery update. New York: McGraw- Hill; 1991: 222-3.
5. Weiss J Mid and lower cervical spine injuries.In: Wilkins R (ed.) Neurosurgery. New York: McGraw- Hill; 1985: 1708-15.
6. Kirshblum S; Campagnolo D; Delisa J (2001). Spinal Cord Medicine. Lippincott Williams & Wilkins.
7. Hadley, M. N. (2002). Management of acute spinal cord injuries in an intensive care unit or other monitored setting. Neurosurgery 2002. Mar; 50(3suppl): S51-7.
8. Tator CH, Duncan EG, Edmonds VE, et al: Comprasion of surgical and conservative management in 208 patients with spinal cord injury. Can J Neurosci 14: 60-69, 1987.
9. Wagner FC, Chehrazi B: Early decompression and neurological outcome in acute cervical spinal cord injuries. J Neurosurg 56: 699-705, 1982.
10.Shingu H, Ikata T, Katoh S, Akatsu T. Spinal cord injury in Japan: A nationwide epidemiological survey in 1990. Paraplegia 1994; 32: 3-8.
11.Karamehmetoglu SS et al. Traumatic spinal cord injuries in Southeast Turkey: an epidemiological study. Spinal Cord 1997; 35: 531-533.
12.Nobuaga AL, Go BK, Karunas RB. Recent Demographic and Injury Trends in People Served by the Model Spinal Cord Injury Care Systems. Arch Phys Med Rehabil 1999; 80: 1372-1382.
13.Whiteneck G, Tate D, Charlifue S. Predicting community reintegration after spinal cord injury from demographic and injury characteristics. Arch Phys Med Rehabil 1999; 80: 1485. 14.Jackson AB, Dijkers M, DeVivo MJ, Poczatek RB. A demographic profile of new traumatic
spinal cord injuries: change and stability over 30 years. A RCH PHYS Med Rehabil 2004: 85: 1740-1748.
15.Agarwal P, Upadhyay P, Raja K. A demographic profile of traumatic and non- traumatic spinal injury cases: a hospital based study from India. Spinal Cord 2007; 45: 597-602.
16.Schizas C, Mouhsine E, Chevalley F, Theumann N, Duff J. Rev Med Suisse. 2005 Dec 21; 1(46): 2978-81.
17.Bhat AR, Wani MA, Kirmani AR, et al: Missile injuries of spine and spinal cord in civilian Kashmir – Analysis and outcome evaluated by new Modified SKIMS-Functional scales. Indian Journal of Neurotrauma 9(2012) 99-111.
18.Pickett GE, Campos-Benitez M, Keller JL, Duggal N. Epidemiology of traumatic spinal cord injury in Canada. Spine (Phila Pa 1976), 2006Apr 1; 31(7): 799-805
20.Kormas, Korhes D. Fractures of the upper Thoracic spine, Bone Joint surg (BR)1997;79-B: Supp-II.
21.Mclain RF, Burkus JK, Benson DR. Segmental instrumentation for thoracic and thoracolumbar fractures. Prospective analysis of construct survival and five years follow up spine J. 2001 Sep-Oct. 1(5): 310-23.
5. Senior Resident, Department of Surgery, SKIMS, Soura, Srinagar.
6. Senior Resident, Department of Anesthesiology and Critical Care, GMC, Srinagar.
NAME ADDRESS EMAIL ID OF THE CORRESPONDING AUTHOR:
Dr. Mudasir Habib, Senior Resident, Department of Surgery,
SKIMS, Soura, Srinagar-190011. E-mail: shahmudasir07@gmail.com
Date of Submission: 21/07/2015. Date of Peer Review: 22/07/2015. Date of Acceptance: 24/07/2015. Date of Publishing: 30/07/2015.
AUTHORS:
1. Mudasir Habib
2. Muzefer Ahmad Ahanger 3. Tarooq Ahmad Reshi 4. Abdul Rashid Bhat 5. Shahnawaz Mansoor 6. Mushtaq Ahmad Rather
PARTICULARS OF CONTRIBUTORS:
1. Senior Resident, Department of Surgery, SKIMS, Soura, Srinagar.
2. Senior Resident, Department of Surgery, SKIMS, Soura, Srinagar.
3. Senior Resident, Department of Surgery, SKIMS, Soura, Srinagar.