R eview
REVISTA PAULISTA DE MEDICIN A
Efficacy in tre atme nt of subclinical ce rvical HPV
infe ction without intrae pithe lial ne oplasia:
syste matic re vie w
Instituto Fernandes Figueira, Fundação O swaldo Cruz, Rio de Janeiro, Brazil
a b s t r a c t
CON TEX T:
The treatment o f the subclinical Human papillo mavirus (HPV) infectio n o f the uterine cervix is co ntro versial.OBJECTIVE:
To assess the efficacy o f any therapy fo r subclinical HPV infectio n o f the cervix witho ut intraepithelial neo plasia, via a search in the medical literature.M ETHOD:
W e perfo rmed a systematic review with a co mprehensive reference search in Medline, LILACS, Excerpta Medica, AIDSLIN E, Po pline, Co chrane Library and o ther autho rs’ reference lists to iden-tify experimental studies o f therapy fo r subclinical HPV infectio n with-o ut intraepithelial newith-o plasia with-o f the uterine cervix. In with-o rder twith-o identify unpublished studies, we also co ntacted experts in the area, clinical trial reg istries, pharmaceutical industries, g o vernment and research institutio ns. W e also searched o n the Internet and in the bo o k-o f-abstracts o f so me medical co nferences. The studies identified were masked and selected by inclusio n criteria to help ascertain their internal validity. The data abo ut reg ressio n o r pro g ressio n o f HPV infectio n were extracted fro m the studies included.RESULTS:
W e identified 6 7 studies related to the treatment o f sub-clinical HPV infectio n witho ut intraepithelial neo plasia o f the uterine cervix. O nly five clinical trials matched the inclusio n criteria and no ne demo nstrated sig nificant differences between the experimen-tal g ro up and the co ntro l g ro up co ncerning reg ressio n o f HPV infec-tio n (with o r witho ut CIN I) o r pro g ressio n to hig her g rades o f CIN .CON CLUSION :
The evidence we fo und in the medical literature re-g ardinre-g the efficacy o f any therapy fo r subclinical HPV infectio n witho ut intraepithelial neo plasia o f the uterine cervix was unsatisfac-to ry.KEY W ORDS:
HPV. Cervical Intraepithelial N eo plasia. Treatment. Systematic Review.• Fábio Russo mano • Aldo Reis • Maria Jo sé de Camarg o • Maria Virg ínia Peixo to Dutra • Sandra Co sta Fo nseca • Jean Anderso n
INTRODUCTION
The treatment o f subclinical human papillo mavirus
(HPV)
1infectio n is a matter o f co ntro versy. As defined by
Reid et al (1982), in this kind o f HPV infectio n, instead o f
pro ducing an o vert co ndylo ma, a “macro sco pic invisible,
no n-papillifero us epithelial hyperplasia” can be pro duced.
Co nsidering the high incidence o f cervical cancer wo
rld-wide, it wo uld be reaso nable to try to treat all fo rms o f
HPV infectio n to prevent future cancer develo pment. Ho
w-ever, co nsidering the high frequency o f spo ntaneo us
re-gressio n o f HPV infectio n and the lack o f a specific
antivi-ral drug, many experts fo llo w these patients co nservatively
and treat cervical intraepithelial neo plasia (CIN), sho uld
it develo p.
The go al o f this paper is to search fo r evidence
o f efficacy o f any treatment fo r subclinical HPV
infec-tio n o f the cervix when there is no co nco mitant CIN
using a systematic review o f the medical literature.
METHODS
Study search
Tri-als Registries, go vernment agencies, pharmaceutical
co mpanies and Internet sites.
In digital media, the search was carried o ut using
terms related to uterine cervix, treatment and
subclini-cal HPV infectio n (Table 1). The search perio d ranged
fro m 1977 to March 1997, since the first studies linking
HPV to cervical neo plasia date fro m 1977. Studies
pub-lished in English, Spanish o r Po rtuguese were included.
The studies identified were obtained and their
meth-o dmeth-o lmeth-o gy was assessed tmeth-o verify their internal validity.
The criteria used to diagno se HPV infectio n
var-ied between autho rs. Different diagno stic criteria were
accepted if they were used co nsistently within a given
study, i.e. used to bo th select patients and to
deter-mine o utco me. This allo wed us to include studies do ne
prio r to the availability o f HPV-DNA detectio n
meth-o ds and tmeth-o avmeth-o id selectimeth-o n bias.
HPV infectio n diagno stic criteria included cyto
l-o gy, cl-o lpl-o scl-o py, histl-o ll-o gy l-o r a cl-o mbinatil-o n l-o f these
metho ds. So me o f the mo re recent studies also used
HPV-DNA detectio n metho ds in their analysis.
An instrument was built to assess the internal
va-lidity o f each study and identify studies fo r selectio n,
based o n criteria adapted fro m Guyatt et al
2-4(Table 2).
We assessed the reliability o f this instrument between
two o f the present autho rs (FR & SCF), assessing the
in-ternal validity o f a sample o f 15% o f the studies
identi-fied, and co ncluding that it had go o d reliability.
5-8Each study was masked, with o nly its metho
d-o ld-o gy sectid-o n being assessable. Studies that met
in-clusio n criteria had their data extracted, including
sample size, treatment tested and treatment o utco me
in the experimental and co ntro l gro ups. Data was
ana-lyzed and synthesized but co uld no t be co mbined
be-cause o f differences in treatment mo dalities.
RESULTS
Results of the study search
Studies identified are listed in the Reference
sectio n (references 9 thro ugh 75) and a summary o f
the results o f the study search fro m each so urce is
sho wn in Table 3. Eight studies co uld no t be o btained
fo r review (references 9 thro ugh 16).
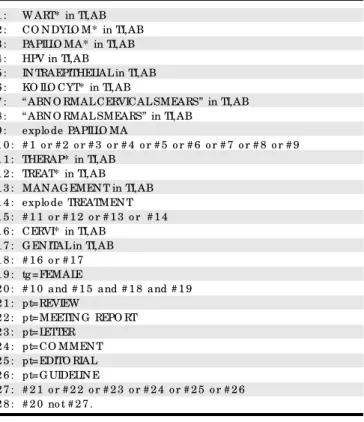
Table 1 - The strate gy use d to se arch for re late d
studie s in Me dline (applie s only to Silve rplatte r 3.1)
1 : W ART* in TI,AB 2 : CO N DYLO M* in TI,AB 3 : PAPILLO MA* in TI,AB 4 : HPV in TI,AB
5 : IN TRAEPITHELIAL in TI,AB 6 : KO ILO CYT* in TI,AB
7 : “ ABN O RMAL CERVICAL SMEARS” in TI,AB 8 : “ ABN O RMAL SMEARS” in TI,AB
9 : explo de PAPILLO MA
1 0 : # 1 o r # 2 o r # 3 o r # 4 o r # 5 o r # 6 o r # 7 o r # 8 o r # 9 1 1 : THERAP* in TI,AB
1 2 : TREAT* in TI,AB 1 3 : MAN AG EMEN T in TI,AB 1 4 : explo de TREATMEN T 1 5 : # 1 1 o r # 1 2 o r # 1 3 o r # 1 4 1 6 : CERVI* in TI,AB
1 7 : G EN ITAL in TI,AB 1 8 : # 1 6 o r # 1 7 1 9 : tg =FEMALE
2 0 : # 1 0 and # 1 5 and # 1 8 and # 1 9 2 1 : pt=REVIEW
2 2 : pt=MEETIN G REPO RT 2 3 : pt=LETTER
2 4 : pt=CO MMEN T 2 5 : pt=EDITO RIAL 2 6 : pt=G UIDELIN E
2 7 : # 2 1 o r # 2 2 o r # 2 3 o r # 2 4 o r # 2 5 o r # 2 6 2 8 : # 2 0 no t # 2 7 .
Table 2 - Inclusion crite ria
(adapte d from Guyatt e t al 1993)
GEN ERAL ASPECTS
• Study o f treatment fo r subclinical HPV infectio n o f the cervix witho ut intraepithelial neo plasia (studies using the term “ lo w g rade lesio n” pub-lished after 1 9 9 0 , were also co nsidered).
• Co mplete investig atio n, with final results sho wn.
M ETHODOLOGICAL ASPECTS
• Rando miz ed clinical trial, placebo -co ntro lled.
• Identical and valid diag no stic metho ds used to identify infected wo men and to measure the results after interventio n.
• Lo ss to fo llo w-up o f 1 0 % o r less. • Fo llo w-up perio d o f at least o ne mo nth. • Intentio n-to -treat analysis.
• Experimental and co ntro l g ro ups similar at entry into the study co n-cerning ag e and o ther facto rs that co uld interact with any treatment mo dality. Differences need to have been checked prio r to analysis. • The g ro ups must be treated and fo llo wed equally, apart fro m the experimental interventio n.
Table 3 - Re fe re nce source s and the ir re sults
(numbe r of studie s ide ntifie d)
Reference sources*
# of identified
# of non-obtained
studies
studies
Medline (alo ne) 1 7 2
Medline & Excerpta Medica 1 4
-Medline & LILACS 4 1
Medline & o ther autho rs’ reference lists 1 0 -Medline, Excerpta Medica &
o ther autho rs’ reference lists 4
-Excerpta Medica (alo ne) 3 1
Excerpta Medica &
o ther autho rs’ reference lists 2
-LILACS (alo ne) 1
-LILACS & o ther autho rs’ reference lists 2 -LILACS & experts’ info rmatio n 1 -O ther autho rs’ reference lists (alo ne) 7 2 Abstracts o f studies
presented in medical meeting s 2 2
Tota ls
6 7
8
Study selection
Of the 59 studies o btained in their full versio n, 5
were included
19-23and 54 were excluded.
17,18,24-75The
pri-mary reaso n why studies were excluded was their study
design (42 studies - 77%). The remaining 12 (22%) sho wed
o ne o f the fo llo wing situatio ns: fo ur were clinical trials
but were no t placebo -co ntro lled; two had mo re than 10%
o f patients lo st to fo llo w-up; o ne tested adjuvant therapy
instead o f primary therapy; o ne assessed the o utco me
differently in experimental and co ntro l gro ups; o ne
ana-lyzed patients with HPV witho ut CIN to gether with
pa-tients with CIN I (published befo re 1990) o r CIN II; o ne
tested the therapy o n clinically-expressed HPV infectio n;
o ne repo rted o nly preliminary data; and in o ne we were
no t able to extract the info rmatio n needed fro m it.
In Table 4 and in the fo llo wing text we sho w a
brief summary o f the five studies that met the
inclu-sio n criteria. Two studies included at first were then
excluded. The first o ne was the study by Ylisko ski et
al, 1991.
17They had studied a gro up o f patients with
HPV witho ut CIN to gether with o thers with CIN. We
wro te to o ne o f the autho rs (KS) and he to ld us that
the data was no t available anymo re. The o ther study
was the o ne fro m Wo o dman et al, 1993.
18This study
presents treatment o utco mes fro m patients with pro
-gressio n risk and it was no t stated ho w many patients
had regressio n o r pro gressio n. We wro te to the first
autho r but we have no t had any reply yet.
Boothby et al.,
191990.
This is a rando mized clinical trial testing trichlo
-ro acetic acid (TCA) at 50% co ncentratio n, applied to the
cervix. Thirty-fo ur wo men with bio psy-pro ven HPV
infec-tio n o f the cervix were rando mly allo cated to receive TCA
o r no rmal saline in a blinded fashio n. The o utco me was
assessed 16 weeks after treatment. The treatment was
co nsidered a failure if there was evidence o f HPV o n Pap
smear o r bio psy. The text do es no t pro vide a similarities
analysis between the gro ups after treatment allo catio n.
Altho ugh the autho rs state that patients and
investiga-to rs were blinded investiga-to the treatment allo catio n, there is a
marked difference in cervix appearance after applying the
two substances. The applicatio n o f TCA turns the cervix
surface white, as a result o f chemical co agulatio n o f its
epithelium pro teins and impairment in viewing the co lo r
o f the stro ma. If this had been repo rted in patient reco rds,
to the patient o r kept in mind by the medical do cto r, the
blinding co uld have been impaired (po tential so urce o f
assessment bias). When the first 15 patients in each gro up
were analyzed, no differences were no ted and the study
was clo sed. No patients were lo st to fo llo w-up. Six wo men
in the experimental gro up and two in the co ntro l gro up
had undesirable side effects. Two wo men in the
experi-mental gro up develo ped CIN I.
Diakomanolis et al.,
201990.
This study enro lled 452 wo men with b io
psy-pro ven HPV cervical infectio n witho ut CIN. The autho rs
repo rt that “patients were allo cated rando mly under a
specific number” (page 506), which is unclear to us.
There is no similarities analysis between the study
gro ups after the allo catio n fo r treatment. The study
gro up had vapo rizatio n o f the entire transfo rmatio n
zo ne, distal endo cervical canal and “brushing” o f the
cervix po rtio while the co ntro l gro up received no
treat-ment. It was no t po ssible to blind the pro cedure
be-ing studied to patients and investigato rs. After 18
mo nths, 8 (5.6%) wo men fro m the treatment gro up
and 24 (7.7%) o f the co ntro l gro up sho wed pro
gres-sio n to pre- invasive disease (P = 0.42). No data was
presented o n the disappearance o f the disease.
Ruge et al.,
211992.
In this study 50 wo men with bio psy-pro ven HPV
infectio n with o r witho ut co nco mitant CIN I were
ran-do mly allo cated to a laser gro up o r a co ntro l gro up.
The re is no info rm atio n ab o ut the rando m izatio n
metho d used. Ho wever, despite this limitatio n, there
were no statistical differences between study and co
n-tro l gro ups in age, smo king, so cio eco no mic status,
sexual habits and co ntraceptive metho ds. The treatment
gro up had their entire transfo rmatio n zo ne “evapo rated”
to a depth o f 4-5 mm. The co ntro l gro up had no
treat-ment. As in the previo us study, there was no patient o r
Table 4 - Include d studie s
Author, publica tion yea r
Pa tients selected
Trea tment method tested
Bo o thby et al.,1 9 1 9 9 0 . HPV infectio n witho ut CIN 5 0 % trichlo ro acetic acid applicatio n.
Diako mano lis et al.,2 0 1 9 9 0 . HPV infectio n witho ut CIN CO
2 laser vapo riz atio n o f the entire transfo rmatio n z o ne, distal
reg io n o f the endo cervical canal and, mo re superficially, the ecto cervical reg io n o utside the transfo rmatio n z o ne. Rug e et al.,2 1 1 9 9 2 . HPV infectio n with o r witho ut CIN I CO
2 laser vapo riz atio n o f the entire transfo rmatio n z o ne and
adjacent areas to 4 -5 mm in depth. Ho rding et al.,2 2 1 9 9 3 . HPV infectio n with o r witho ut CIN I CO
2 laser vapo riz atio n o f the entire transfo rmatio n z o ne.
Fairley et al.,2 3 1 9 9 6 . HPV infectio n witho ut CIN * Beta-caro tene, 3 0 mg / day, taken o rally fo r o ne year.
investigato r blinding regarding which gro up each
pa-tient was allo cated to . After 12 mo nths, the autho rs
analyzed regressio n, persistence and pro gressio n and
fo und no statistical differences between the two gro ups.
Hording et al.,
221993.
In this study, the autho rs analyzed 46 wo men
with bio psy-pro ven HPV cervical infectio n with o r
with-o ut CIN I. These wwith-o men were allwith-o cated randwith-o mly twith-o a
treatment gro up (laser vapo rizatio n o f the cervix) o r
to a co ntro l gro up witho ut treatment. The autho rs did
no t repo rt the rando mizatio n metho d used and there
is no analysis o f gro up similarities after treatment
al-lo catio n. As in the two previo us studies, there was no
patient o r investigato r blinding co ncerning treatment
o r co ntro l pro cedures. No patients were lo st to fo
l-lo w-up, with mean fo ll-lo w-up o f 28 mo nths (range o f
12 to 54 mo nths). There were no significant differences
between the study gro ups.
Fairley et al.,
231996.
Co nsidering epidemio lo gical and labo rato ry
evi-dence that beta caro tene may be o f value in the
treat-ment o f pre-invasive cervical disease, these autho rs
per-fo rmed a do uble-blind clinical trial in which 117 wo men
were rando mly allo cated to receive beta caro tene (30
mg/daily) o r placebo (lecithin, 400 mg/daily) fo r o ne year.
There is no repo rt o f the rando mizatio n metho d used
but the gro ups were similar in age, marital status, smo
k-Table 5 - Progre ssion of HPV infe ction with or without CIN I
Author,
Ex perimental
Progression
Control
Progression
P-value
Follow -up
year
group (n)
n (%)
group (n)
n (%)
Diako mano lis et al.,2 0 1 9 9 0 1 4 2 8 (5 .6 %) HPV to CIN I-III 3 1 0 2 4 (7 .7 %) HPV to CIN I-III 0 .4 2 1 8 mo nths
Rug e et al.,2 1 1 9 9 2 2 5 2 (8 %) HPV-CIN I to CIN III 2 5 2 (8 %) HPV-CIN I to CIN III 0 .6 0 1 2 mo nths
Table 6 - Re gre ssion of HPV infe ction with or without CIN I
Author,
Experimental
Disappearance
Control
Disappearance
P-value
Follow -up
year
group (n)
or regression of HPV
group (n)
or regression of HPV
subclinical lesionsn (%)
subclinical lesions n(%)
Bo o thby et al.,1 9 1 9 9 0 1 5 1 (6 .7 %) 1 5 3 (2 0 %) 0 .5 2 4 mo nths
Rug e et al.,2 1 1 9 9 2 2 5 2 1 (8 4 %) 2 5 1 9 (7 6 %) 0 .4 8 1 2 mo nths
Ho rding et al.,2 2 1 9 9 3 2 3 2 1 (9 1 .3 %) 2 3 1 6 (6 9 .5 %) 0 .1 1 1 2 to 5 4 mo nths
Fairley et al.,2 3 1 9 9 6 3 3 2 0 (6 0 .6 %) 3 6 2 2 (6 1 .1 %) 0 .9 6 1 2 mo nths
Table 7 - HPV-DNA de te ction in the se le cte d studie s
Author, yea r
HPV-DN A a na lysis
Ruge et al.,2 1 1 9 9 2 HPV-1 6 DNA detected by PCR, befo re and after the study perio d. There was no difference between the success rate
of the HPV+ laser treatment group (7 8 .5 %) compared to the control group (8 0 %) in achieving HPV-1 6 -DNA disappearance. Ho rding et al.,2 2 1 9 9 3 HPV 6 ,1 1 ,1 6 ,1 8 and 3 3 detected by PCR befo re and after the study perio d. There was a sig nificant statistical
difference between the HPV+ laser treatment g ro up (1 2 / 1 3 , 9 2 %) and co ntro l g ro up (2 / 7 , 2 9 %, p = 0 .0 0 7 ). Fairley et al.,2 3 1 9 9 6 HPV-DN A detected by PCR o r Hybrid Capture. There was no difference in the detectio n o f HPV-DN A between
treatment and co ntro l g ro ups.
ing, co ntraceptive metho d, parity and number o f sexual
partners. After o ne year o f fo llo w-up no differences were
fo und between the study gro ups in terms o f lesio n
clear-ance. Thirteen per cent o f the wo men receiving
beta-caro tene no ticed yello wing o f the skin.
Information extracted from the selected studies
Table 5 sho ws data extracted fro m the selected
studies co ncerning pro gressio n o f HPV infectio n
with-o ut CIN twith-o presence with-o f CIN with-o r frwith-o m HPV with CIN I twith-o
higher grades o f CIN. Table 6 sho ws data related to
dis-appearance o f subclinical HPV with o r witho ut CIN I.
Three studies included an analysis o f the
pres-ence o f HPV-DNA and its disappearance after the
ex-perimental perio d. These data are sho wn in Table 7.
DISCUSSION
Fro m the 59 studies identified, o btained and
reviewed, o nly five met the inclusio n criteria. No ne o f
these fo und any difference between treatment and
co ntro l gro ups in either pro gressio n o r regressio n o f
subclinical HPV infectio n o f the cervix. Ho wever, these
studies were limited by o ne o r mo re pro blems, such
as the sample size, difficulties in blinding patients and
investigato rs, and we do no t kno w the rando mizatio n
metho d used by fo ur o f them. These limitatio ns leave
us unsure that the treatments tested are ineffective.
o f lack o f internal validity fo r adequately testing any
fo rm o f treatment.
Altho ugh we co uld no t o btain 8 studies in their
full versio n, even after attempts using natio nal o r fo
r-eign libraries and asking the autho rs fo r them (in the
case o f studies identified in Bo o ks o f Abstracts fro m
medical meetings), assessment o f their abstracts
al-lo wed us to co nclude that they wo uld pro bably be
ex-cluded because they were no t clinical trials.
In the decisio n-making pro cess co ncerning the
use o f any therapy to treat this kind o f HPV infectio n,
we must co nsider the lack o f evidence that treatment
is better than no treatment. The use o f therapies in
which efficacy is no t pro ven can lead to unnecessary
waste o f mo ney o r can be wo rse than the illness itself,
co nsidering the physical co nseq uences o f so me o f
them and the psycho lo gical co nsequences o f trying
to treat an infectio n that can present recurrence.
Well-co nducted rando mized clinical trials can
b e expected to pro ve so me therapy to b e effective
against subclinical HPV infectio n, preferably with
pa-tient and investigato rs being blinded, and with
suffi-cient sample size with eno ugh po wer to avo id beta
erro r (i.e. saying that there is no difference between
treatment and no treatment when it actually exists and
the o nly reaso n that statistical significance was no t
achieved was because o f the small sample size).
Ho wever, applying financial reso urces to co nduct
an experiment to clarify this questio n appear unreaso
n-able to us. Given the high prevalence repo rted by so me
autho rs, varying between 13 to 20% in develo ping co
un-tries, in which Brazil is included,
76and the transient
char-acteristic o f mo st o f these infectio ns,
77the co st o f
medi-cine usage, therapeutic pro cedures o r vacmedi-cines wo uld
no t be reaso nable in the preventio n o f cervical cancer.
On the o ther hand, there is already stro ng
evi-dence o f efficacy in treatment o f pre-invasive diseases
in o rder to prevent cervical cancer. It seems to us that
it is mo re co st-effective to apply these pro cedures to
the patients that present CIN II/III, co nsidering that
they are a small pro po rtio n o f all HPV-infected wo men.
CONCLUSIONS
The evidence we fo und fo r efficacy in treatment
o f subclinical HPV infectio n o f the cervix witho ut CIN
was unsatisfacto ry. Ho wever, co nsidering the
limita-tio ns o f the selected studies, particularly in terms o f
sample size, po ssible efficacy in these treatments
can-no t be excluded.
In many o f the studies excluded fo r metho
d-o ld-o gical reasd-o ns, the authd-o rs’ cd-o nclusid-o n was clearly
in favo r o f the treatments tested, po ssibly leading to
ineffective o r even po tentially harmful therapies and
to unnecessary co sts.
Medline, LILACS and Excerpta Medica were the
mo st useful so urces o f references, and identified all
o f the studies included.
1. Reid R, Stanho pe CR, Herschman BR, Bo o th E, Phibbs GD, Smith JP. Genital warts and cervical cancer: I. Evidence o f an asso ciatio n between subclinical papillo mavirus infectio n and cervical malignancy. Cancer 1982;50:377-87.
2. Guyatt GH, Sackett DL, Co o k DJ. Users’ guides to the medical literature. II. Ho w to use an article abo ut therapy o r preventio n. A. Are the results o f the study valid? JAMA 1993;270(21):2598-601.
3. Petitti DB. Meta-analysis, Decisio n analysis and co st-effectiveness analysis - metho ds fo r quantitative synthesis in medicine. Oxfo rd: Oxfo rd University Press 1994.
4. Guyatt GH, Rennie D. Users’ guides to the medical literature [edito rial]. JAMA 1993;270(17):2096-7.
5. Co hen J. A co efficient o f agreement fo r no minal scales. Educ Psycho l Measur 1960;20:37-46.
6. Bartko JJ, Carpenter WT. On the metho ds and theo ry o f reliability. J Nerv Ment Dis 1976;163(5):307-17.
7. Landis JR, Ko ch GG. The measurement o f o b server agreement fo r catego rical data. Bio metrics 1977;33:159-74.
8. Dunn G, Everitt B. Clinical bio statistics: an intro ductio n to evidence-based medicine. New Yo rk: Jo hn Wiley & So ns; 1995.
9. Go ri J, Castano R, Do minguez J, et al. Laser vapo rizatio n, cryo therapy and trichlo ro acetic acid applicatio n in the therapy o f ecto cervical co ndylo mato us lesio ns: a co mpariso n o f clinical results. Cervix 1992;10(4):217-9.
10. Madej J, Basta A, Madej Jr JG, Strama M. Co lpo sco py staging and
treatment o f papillo mavirus infectio n o f the cervix. Clin Exp Obstet Gyneco l 1992;19(1):34-9.
11. Minucci D, Cinel A, Insacco E. Diathermic lo o p treatment fo r CIN and HPV lesio ns. A fo llo w-up o f 130 cases. Eur J Gyneco l Onco l 1991;12(5):385-93.
12. Naud P, Mo nego H, Ricco L, Catalan F. O uso de nitro gênio líquido na terapêutica do papilo mavirus humano (HPV) co m co nfirmação po r hib ridização mo lecular. XV Brazilian Co ngress o f Gyneco lo gy and Obstetrics; 1989 (Bo o k o f Abstracts).
13. Pietro luo ngo A, Pereira Filho A, Levente A. Tratamento das viro ses pelo papilo mavirus humano (HPV) co m vacina BCG. XV Brazilian Co ngress o f Gyneco lo gy and Obstetrics; 1989 (Bo o k o f Abstracts).
14. Salvo A, Ro jas I, Figueiro a L, Stuardo P. Imuno terapia po r via cutanea co n dinitro clo ro benceno en infeccio n del cuello uterino po r virus papilo ma. Rev Child Obstet Gineco l 1991;56(6):460-3.
15. To rrisi A, Cinel A, Wittemberg L, Minucci D. Therapy with ß-interfero n cream in the cervical-vaginal infectio ns by Human papillo ma virus (HPV). Eur J Gyneco l Onco l 1987;7(4-5):441.
16. Tro fatter Jr. Interfero n treatment o f ano genital papillo mavirus-related diseases. Dermato l Clin 1991;9(2):343-52.
17. Ylisko ski M, Syrjänen K, Syrjänen S, Saariko ski S, Nethersell A. Systemic alpha-interfero n (Wellfero n) treatment o f genital Human papillo mavirus (HPV) Type 6,11,16 and 18 infectio ns: a do uble-blind, placebo -co ntro lled trial. Gyneco l Onco l 1991;43:55-60.
18. Wo o dman CBJ, Byrne P, Kelly KA, Hilto n C. A rando mized trial o f laser
vapo rizatio n in the management o f cervical intraepithelial neo plasia asso ciated with Human papillo mavirus infectio n. J Public Health Med 1993;15(4):327-31.
19. Bo o thby RA, Carlso n JA, Rubin M, Mo rgan M, Mikuta JJ. Single applicatio n treatment o f human papillo mavirus infectio n o f the cervix and vagina with tric hlo ro ac e tic ac id : a rand o m ize d trial. O b s te t Gyne c o l 1990;76(2):278-80.
20. Diako mano lis E, Ro do lakis A, Simiakaki H, Frango po ulo u E, Efstratiado u M. Rando mized co ntro l trial o f laser vapo rizatio n in the management o f Human papillo mavirus infectio n in the uterine cervix. Rec Adv Cerv Patho l Co lpo sc, 1990;3:505-10.
21. Ruge S, Felding C, Sko uby SO, Lundvall F, Ho rding U, No rrild B. CO2 laser vapo rizatio n in the treatment o f cervical Human papillo mavirus infectio n in wo men with abno rmal Papanico lao u smears. Gyneco l Obstet Invest 1992;33(3):172-6.
22. Ho rding U, Rygaard C, Ruge S, Felding C, Lundvall F, Junge J. Cervical ko ilo cyto sis and high risk HPV types: the benefit o f laser vapo rizatio n. Eur J Obstet Gyneco l Repro d Bio l 1993;51(2):125-30.
23. Fairley CK, Tabrizi SN, Chen S, et al. A rando mized trial o f beta-caro tene vs. placebo fo r the treatment o f cervical HPV infectio n. Int J Gyneco l Cancer 1996;6:225-30.
24. Ali SW, Evans AS, Mo naghan JM. Results o f CO2 laser cylinder vapo rizatio n o f cervical intraepithelial disease in 1234 patients. An analysis o f failures. Br J Obstet Gyneco l 1986:93(1):75-8.
25. Baggish MS. Treating viral venereal infectio n with the CO2 laser. J Repro d Med 1982;27(12):737-42.
26. Benrubi G, Nuss RC, Ho lmes K, Lammert N. Efficacy o f cryo therapy in the treatment o f human papillo mavirus infectio n o f the uterine cervix. J Fla Med Asso c 1986;73(3):188-91.
27. Benrubi GI, Shanno n J, Glazer J, Nuss RC. Cervical human papillo ma virus infectio n: is treatment po ssible? J Fla Med Asso c 1988;75(12):799-800.
28. Bo o thby RA, Benrubi GI, Nuss RC, Lammert N. Laser treatment o f Human papillo mavirus infectio ns o f the uterine cervix. Co lpo sc Gyneco l Laser Surg 1986;2(1):25-9.
29. Bro dman M, Do ttino P, Friedman Jr F, Heller D, Bleiweiss I, Sperling R Human papillo mavirus-asso ciated lesio ns o f the vagina and cervix. Treatment with a laser and issueal 5-fluo ro uracil. J Repro d Med 1992;37(5):453-6.
30. Caballero F, Baez J, Tro ya CI. La crio terapia en el tratamiento de las lesio nes premalignas del cervix uterino . Rev Med Caja Seguro So cial 1985;17(2):140-3.
31. Cinel A, Wittenberg L, Minucci D. ß-interfero n issueal treatment in lo w and high-risk cervical lesio ns. Clin Exp Obstet Gyneco l 1991;18(2):91-7.
32. Co sta S, Po ggi MG, Palmisano L, Syrjänen S, Ylisko ski M, Syrjänen K. Intramuscular ß-interfero n treatment o f Human papillo mavirus lesio ns in the lo wer female genital tract. Cervix 1988;6:203-12.
33. das Do res GB, Martins NV, Fo cchi J, et al. Tratamento da infecção cérvico -vaginal po r papilo mavirus humano HPV co m quatro fármaco s. J Bras Gineco l 1993;103(6):205-10.
34. das Do res GB, Ribalta JCL, Martins NV, et al Tratamento da infecção do co lo uterino po r papilo mavirus humano co m interfero n gel. Rev Paul Med 1991;109(4):179-83.
35. Davila GW, Shro yer KR. Issueal 5-fluo ro uracil in the treatment o f cervical Human papillo mavirus infectio n. Gyneco l Obstet Invest 1996;41(4):275-7.
36. Diako m ano lis E, Ro d o lakis A, Dailianas S, Kalp akts o gio u K, Sakellaro po ulo s G, Aravantino s D. Lo ng term results o f CO2 laser treatment o f lo w-grade squamo us intraepithelial lesio ns. Cervix 1995;13:149-52.
37. Evans AS, Mo naghan JM, Beattie AB. Carbo n dio xide laser treatment o f cervical warty atypias. Gyneco l Onco l 1984;17:296.
38. Gal D, Friedman M, Mitrani-Ro senbaum S. Transmissibility and treatment failures o f different types o f human papillo mavirus. Obstet Gyneco l
1989;73(3 Pt 1):308-11.
39. Gall SA, Co nstantine L, Ko uko l D. The rapy o f pe rsiste nt hum an papillo mavirus disease with two different interfero n species. Am J Obstet Gyneco l 1991;164(1):130-4.
40. Go nzalez-Sanchez JL, Celis C, Ro driguez-de-Santiago JD, Pena-Sando val M, Menendez-Velasquez J. Tratamiento del virus del papilo ma humano (VPH) del cervix co n crio cirugia. Gineco l Obstet Mex 1991;59:164-8.
41. Husseinzadeh N, Guo th JG, Jayawardena DS. Subclinical cervico vaginal human papillo mavirus infectio ns asso ciated with cervical co ndylo mata and dysplasia. Treatment o utco mes. J Repro d Med 1994;39(10):777-80.
42. Klutke JJ, Bergman A. Interfero n as an adjuvant treatment fo r genital co ndylo ma acuminatum. Int J Gyneco l Obstet 1995;49:171-4.
43. Lira Neto JB, Santo s JF, Vieira IM. Infecção gineco ló gica pelo vírus do co ndilo ma. Co ntribuição ao diagnó stico e terapêutica. J Bras Gineco l 1984;94:295.
44. Luesley MD, Cullimo re J, Redman CWE, et al. Lo o p diathermy excisio n o f the cervical transfo rmatio n zo ne in patients with abno rmal cervical smears. BMJ 1990;300:1690-3.
45. Maldo nado P, Christo Jr WG, Mannarino MPB. Ensaio terapêutico co m Thuya o ccidentalis em pacientes po rtado ras de infecção pelo HPV no trato genital inferio r. Annals o f the IX Brazilian Co ngress o f Cervical Patho lo gy and Co lpo sco py; 1992.
46. Maldo nado P, Christo WG, Co sta CM, Po llastri CE, Cavalcanti RMVF, Pereira NA. Co nduta nas infecçõ es cervico vaginais pelo HPV no IG UFRJ. Femina 1991;19:324.
47. Malviya VK, Deppe G, Pluszczynski R, Bo ike G. Trichlo ro acetic acid in the treatment o f human papillo mavirus infectio n o f the cervix witho ut asso ciated dysplasia. Obstet Gyneco l 1987;70:72-4.
48. Marko wska J, No wak M, Niecewicz R, Brebo ro wicz J, Wiese E, Zengteler G. Results o f issueal treatment o f HPV infectio n in the uterine cervix using interfero n beta, 13-cis-retino ic acid and TFX. Eur J Gyneco l Onco l 1994;15(1):65-9.
49. Menendez-Velazquez JF, Go nzalez-Sanchez JL, Ro driguez-de-Santiago JD, Muno z-Reyes R, Bailo n-Uriza R. Tratamiento de la infeccio n cervical po r el virus del papilo ma humano (VPH) co n acido triclo ro acetico . Gineco l Obstet Mex 1993;61:48-51.
50. Merkur H, Baird PJ. Papillo mavirus infectio n o f the female genital tract befo re and after treatment: a cyto lo gical, co lpo sco pic and histo lo gical study. Aust N Z J Obstet Gyneco l 1989;29(3 Pt 1):185-8.
51. Milla-Villeda RH, Gurro la-Medrano T. Tratamiento de la infeccio n cervical subclinica po r el virus del papilo ma humano (VPH) co n asa diatermica. Eficacia a co rto plazo . Gineco l Obstet Mex 1995;63:293-6.
52. Mitchell H, Medley G. Evidence against diathermy as a beneficial treatment fo r HPV infectio n o f the cervix. Aust N Z J Obstet Gyneco l 1989;29(4):439-42.
53. Mo hanty KC, Lo we JW. Cryo therapy in the management o f histo lo gically diagno sed sub clinical HPV infectio n o f the cervix. Br J Clin Pract 1990;44(12):574-7.
54. Mo hanty KC, Lo we JW. Co ld co agulatio n therapy in the treatment o f histo lo gically diagno sed subclinical human papillo mavirus infectio n o f the cervix. Br J Clin Pract 1991;45(2):102-4.
55. Nieminen P, Aho M, Lehtinen M, Vesterinen E, Vaheri A, Paavo nen J. Treatment o f genital HPV infectio n with carbo n dio xide laser and systemic interfero n alpha-2b. Sex Transm Dis 1994;21(2):65-9.
56. Puttemans P, van Pelle Y, De Muylder E. Carbo n dio xide laser vapo rizatio n o f cervical subclinical papillo maviral infectio n neo plasia: sho rt-term effectiveness. Eur J Obstet Gyneco l Repro d Bio l 1986;23:167-80.
58. Riva JM, Sedlacek TV, Cunnane MF, Mangan CE. Extended carbo n d io xid e las e r vap o rizatio n in th e tre atm e n t o f s u b c lin ic al papillo mavirus infectio n o f the lo wer genital tract. Obstet Gyneco l 1989;73(1):25-30.
59. Ro gstad KE, Dixo n CA, Ahmed IH. The management o f subclinical wart virus infectio n o f the cervix in a genito urinary clinic. Geniturin Med 1992;68(5):307-8.
60. Ruge S, Fe lding C, Sko ub y SO, Lundvall F, Ho rding U. CO2 lase r vap o rizatio n o f hum an p ap illo m avirus (HPV)-ind uc e d ab no rm al cervical smears. A simple and effective so lutio n to a recurrent clinical pro blem. Clin Exp Obstet Gyneco l 1991;18(2):99-101.
61. Schneider A, Papendick U, Gissmann L, De Villiers E-M. Interfero n treatment o f human genital papillo mavirus infectio n: impo rtance o f viral type. Int J Cancer 1987;40:610-4.
62. Semprini AE, Stillo A, Marco zzi S, Castagna C, Fio re S, Radaelli U. Treatment with interfero n fo r genital HPV in po sitive and HIV-negative wo men. Eur J Obstet Gyneco l Repro d Bio l 1994;53(2):135-7.
63. Sesti F, De-Santis L, Farne C, Mantenuto L, Piccio ne E. Efficacy o f CO2 laser surgery in treating squamo us intraepithelial lesio ns. An analysis o f clinical and viro lo gic results. J Repro d Med 1994;39(6):441-4.
64. Stefano n D. Activity o f interfero n-ß in small co ndylo mato us lesio ns o f the uterine cervix. Cervix 1983;1:23-6.
65. Stentella P, Frega A, Di-Renzi F, Palazzetti PL, Pachi A. Issue and systemic administratio n o f natural alpha interfero n in the treatment o f female and male HPV genital infectio ns. Clin Exp Obstet Gyneco l 1996;23(1):29.
66. Strand A, Wilander E, Zehbe I, Rylander E. High risk HPV persists after treatment o f genital papillo mavirus infectio n but no t after treatment o f ce rvical intrae pithe lial ne o plasia. Acta Ob ste t Gyne co l Scand 1997;76(2):140.
67. Surwit EA, Grahan V, Dro egemueller W, et al. Evaluatio n o f issueally applied trans-retino ic acid in the treatment o f cervical intraepithelial
lesio ns. Am J Obstet Gyneco l 1982;143(7):821-3.
68. Villani C, No bili F, Stentella P, Pace S. The viral lesio n (HPV) o f the lo wer genital tract in teenagers: clinical and therapeutic aspects. Eur J Gyneco l Onco l 1989;10(4):267-71.
69. Villani C, Vecchio ne A, Pace S, Carenza L. The ratio nale fo r treatment o f c e rvic al le s io n s ( HPV + / - CIN) . Clin Exp O b s te t Gyn e c o l 1989;16(1):44-7.
70. Ward BG, Tho mas IL. Rando mized pro spective interventio n study o f Human ce rvical wart virus infe ctio n. Aust N Z J Ob ste t Gyne co l 1994;34(2):182-5.
71. Weck PK, Buddin DA, Whisnant JK. Interfero n in the treatment o f genital Human papillo mavirus infectio ns. Am J Med 1988;85(Suppl 2A):159-64.
72. Wince slaus SJ, Bro wn C, Go h BT. Managing wo m e n with hum an p ap illo m avirus c hang e s in c e rvic al c yto lo g y. Ge nito urin Me d 1988;64(4):259-62.
73. Ylis ko s ki M, Saariko s ki S, Syrjäne n K, Syrjäne n S, Cas tré n O . Cryo therapy and CO2 laser vapo rizatio n in the treatment o f cervical a n d va g in a l HPV in fe c tio n s . Ac ta O b s te t Gyn e c o l S c a n d 1989;68(7):619-25.
74. Zarco ne R. Treatment o f genital HPV-infectio ns with natural alpha interfero n fro m no rmal human leuko cytes. Clin Exp Obstet Gyneco l 1995;22(1):14-9.
75. Zarco ne R, Be llini P, Cardo ne G, Cardo ne A. Tre atme nt o f ce rvix co ndylo mata with alpha-IFN leuco cytar. Clin Exp Ob stet Gyneco l 1995;22(4):326-9.
76. Bo s c h FX, Mano s MM, Muno z N e t al. Pre vale nc e o f hum an papillo mavirus in cervical cancer: a wo rldwide perspective. J Natl Cancer Inst, 1995;87:796-802.
77. Villa LL. Human papillo maviruses and cervical cancer. Adv Cancer Res, 1997;71:321-41.
r e s u m o
CON TEXTO:
O tratamento da infecção subclínica pelo papilo mavírus humano (HPV) no co lo uterino é co ntro verso .OBJETIVO:
Avaliar a eficácia de alg uma terapia para infecção pelo HPV no co lo uterino sem neo plasia intraepitelial.M ÉTO DO :
Rea liz a mo s uma revisã o sistemá tic a c o m uma b usc a abrangente de estudos no Medline, LILACS, Excerpta medica, AIDSLINE, Po pline, Co chrane Library e listas de referências de o utro s auto res para identificar estudo s experimentais so bre terapia para a infecção subclínica pelo HPV sem neo plasia intraepitelial no co lo uterino . Para identificar artigo s não publicado s, também co ntactamo s especialistas da área, reg istro s de ensaio s clínico s, indústrias farmacêuticas, instituiç õ es g o verna menta is e de fo mento à pesq uisa . Ta mb ém pro curamo s po r estudo s através da Internet e em livro s de abstracts de alguns evento s médico s. O s estudo s identificado s fo ram mascarado s e selecio nado s po r critério s de inclusão que auxiliaram a garantir sua validade interna. O s dado s so bre regressão o u pro gressão da infecção pelo HPV fo ram extraído s do s estudo s incluído s.RESULTADOS
: Identificamos 6 7 estudos relacionados ao tratamento da infecção subclínica pelo HPV sem neoplasia intraepitelial do colo uterino (N IC). Apenas cinco ensaios clínicos atenderam aos critérios de inclusão e nenhum demonstrou diferenças significativas entre o grupo em teste e o grupo-controle no que se refere a regressão da infecção pelo HPV (com ou sem NIC I) ou progressão para graus mais altos de NIC.CON CLUSÃO:
As evidências de eficácia de alg uma terapia para infecção subclínica pelo HPV sem neo plasia intraepitelial no co lo uterino enco ntradas na literatura médica fo ram insatisfató rias.PALAV RAS-CH AV E:
HPV. N e o p la sia Intra e p ite lia l C e rvic a l. Tratamento . Revisão sistemáticaAcknowle dge me nt
To Francisco Xavier Bo sch, who kindly revised the manuscript and co ntributed to its reinfo rcement.
Fábio Russomano, MSc. Department o f Gyneco lo gy, Instituto Fernandes Figueira, Fundação Oswaldo Cruz, Rio de Janeiro , Brazil.
Aldo Re is, PhD. Clinical Epidemio lo gy Pro gram at UFRJ, Rio de Janeiro , Brazil.
Maria José de Camargo, MSc. Department o f Gyneco lo gy, Instituto Fernandes Figueira, Fundação Oswaldo Cruz, Rio de Janeiro , Brazil.
Maria Virgínia Pe ixoto Dutra, MSc. Epidemio lo gy Service, Instituto Fernandes Figueira, Fundação Oswaldo Cruz, Rio de Janeiro , Brazil.
Sandra Costa Fonse ca, MSc. Leila Diniz Obstetric Unit (Brazilian Health Ministry), Rio de Janeiro , Brazil.
Je an Ande rson, MD. The Jo hns Ho pkins University AIDS Service, Baltimo re, Maryland, USA.
Source s of funding: No t declared
Conflict inte re st: No t declared
Last re ce ive d: 03 January 2000
Acce pte d: 03 January 2000
Addre ss for corre sponde nce :
Fábio Russo mano
Av. Jo ão Carlo s Machado , 380/308 - Barra da Tijuca Rio de Janeiro /RJ - Brasil - CEP 22620-080 E-mail: fabio russo mano @ mo ntreal.co m.br