SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Comparative
analysis
of
pain
in
patients
who
underwent
total
knee
replacement
regarding
the
tourniquet
pressure
夽
Marcos
George
de
Souza
Leão
∗,
Gladys
Pedrosa
Martins
Neta,
Lucas
Inoue
Coutinho,
Thiago
Montenegro
da
Silva,
Yacov
Machado
Costa
Ferreira,
Waryla
Raissa
Vasconcelos
Dias
Fundac¸ãoHospitalAdrianoJorge,Manaus,AM,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16October2015 Accepted10February2016 Availableonline22September2016
Keywords:
Arthroplasty,replacement,knee Painmeasurement
Tourniquets
a
b
s
t
r
a
c
t
Objectives:Toevaluatethroughthevisualanalogscale(VAS)thepaininpatientsundergoing totalkneereplacement(TKR)withdifferentpressuresofthepneumatictourniquet.
Methods:Anobservational,randomized,descriptivestudyonananalyticalbasis,with60 patientswhounderwentTKR,dividedintotwogroups,whichwerematched:agroupwhere TKRwasperformedwithtourniquetpressuresof350mmHg(standard)andtheotherwith systolicbloodpressureplus100mmHg(P+100).Thesepatientshadtheirpainassessedby VASat48h,andatthe5thand15thdaysafterprocedure.Secondarily,thefollowingwere alsomeasured:rangeofmotion(ROM),complications,andblooddrainagevolumeineach group;thedataweresubjectedtostatisticalanalysis.
Results:Afterdataanalysis,therewasnostatisticaldifferenceregardingtheincidenceof complications(p=0.612),ROM(p=0.202),bleedingafter24and48h(p=0.432andp=0.254) orinrelationtoVAS.Nocorrelationwasobservedbetweentimeofischemiacomparedto VASandbleeding.
Conclusions:Theuseofthepneumatictourniquetpressureat350mmHgorsystolicblood pressureplus100mmHgdidnotinfluencethepain,bloodloss,ROM,andcomplications. Thereforethepressuresattheselevelsaresafeanddonotchangethesurgeryoutcomes; thetimeofischemiamustbecloselyobservedtoavoidmajorcomplications.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheFundac¸ãoHospitalAdrianoJorge,DepartamentodeOrtopediaeTraumatologia,Manaus,AM,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.G.deSouzaLeão).
http://dx.doi.org/10.1016/j.rboe.2016.09.005
Análise
comparativa
da
dor
em
pacientes
submetidos
à
artroplastia
total
do
joelho
em
relac¸ão
aos
níveis
pressóricos
do
torniquete
pneumático
Palavras-chave:
Artroplastiadojoelho Medic¸ãodador Torniquetes
r
e
s
u
m
o
Objetivos:Avaliar,pormeiodaescalavisualanalógica(EVA),adorempacientessubmetidos àartroplastiatotaldojoelho(ATJ)comdiferentespressõesdotorniquetepneumático.
Métodos: Foifeitoumestudoobservacional,descritivo,decaráteranalítico,prospectivo, randomizado,noqual60pacientesforamsubmetidosàATJ,divididosemdoisgrupos,os quaisforamcomparadosentresi:umgruponoqualaATJfoifeitacompressãodotorniquete de350mmHg(Padrão)eoutrocom100mmHgacimadapressãoarterialsistólica(P+100). EssespacientestiveramsuadoraferidapelaEVAapós48horas,noquintoeno15◦dias
apósoprocedimentocirúrgico.Secundariamente,forammedidostambémaamplitudede movimento(ADM),osangramentoviadrenosuctoreascomplicac¸õesemcadaumdos gruposestudados;osdadosforamsubmetidosàanáliseestatística.
Resultados: Apósaanálisedosdados,nãofoiconstatadadiferenc¸aestatisticamente signif-icanteemnívelde5%designificânciadapressãoemrelac¸ãoàincidênciadecomplicac¸ões (p=0,612),ADM(p=0,202),aosangramentoapós24e48h(p=0,432ep=0,254)eàEVA. Tambémnãofoiconstatadacorrelac¸ãodotempodeisquemiaemrelac¸ãoaEVAeao san-gramento.
Conclusões: Aspressõesusadasdotorniquetepneumático,350mmHgoupressãoarterial sistólica+100mmHg,nãotiveraminfluênciasobreador,aperdasanguínea,aamplitude demovimentoeascomplicac¸ões,sãopressõessegurasquenãoalteramoresultadofinal, desdequerespeitadosotempodaisquemiaeindividualizadososcasos.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Therole ofthe pneumatic tourniquet isstill controversial. However, it is widely used by orthopedic surgeons. It is believed that its use iseffective inreducing intraoperative bloodlossandcreatingabloodlessfield,whichwould theoret-icallyfacilitatesurgeryandthecementationtechnique.The useofthetourniquetisalmostindispensableinorthopedic practice.
ThemodernpneumatictourniquethasitsrootsinRoman times(199BCto500AD),whenbronzeand leatherdevices (Fig.1)wereusedtocontrolbleedinginlimbamputations dur-ingbattles.ThetermtourniquetwascoinedbyJeanLouisPetit, beingaderivationoftheFrenchverbtourner(rotate).Withthe adventofgeneralanesthesia,in1864JosephListerwasthe firsttouseatourniquettocreateabloodlesssurgicalfield. In1904,HarveyCushingintroducedthefirstinflatable (pneu-matic)cuff,thusallowingthepressureofthetourniquettobe monitoredandcontrolledmanually.1
A disadvantage ofthe tourniquet is the morbidity that comes from its use, especially in neuromuscular injuries secondarytoneuralandmuscletissuesischemiaandto nerve-compressing direct injury. Furthermore, the hemodynamic changesthataccompanyinflationanddeflationmaydepress cardiacfunction inthe perioperativeperiod.2 Theduration
and pressure forsafe tourniquet use remain controversial, andnostrictguidelineshavebeenestablished.Asafelimit of1–3hhasbeendescribed.3Theuseofthetourniquetover
2handpressuresgreaterthan350mmHgonthelowerlimbs
Fig.1–TourniquetusedbytheRomans.Thetourniquetis madeofbronzeandiscoveredwithleathertohelpprotect thethighofthepatientandreducepain.
Source:PrintedwithpermissionoftheScienceandSociety PictureLibrary:http://www.scienceandsociety.co.uk/.
andgreaterthan250mmHgontheupperlimbsincreasethe riskofcompressionandneuropraxia.4
Themostcommonwaytoassesspainisthroughthevisual analogscale(VAS),aninstrumentthatattemptstomeasurea characteristicorattitudethatisbelievedtovaryovera con-tinuumofvaluesandthatcannotbedirectlymeasuredeasily. Forexample,theamountofpainthepatientfeelsmayrange fromnopain(0)toextremepain(10).5
Assessed for eligibility (n=71)
Exclusion (n=11)
♦Did not meet inclusion criteria (n=9) ♦Refused to participate (n=0) ♦ Other reasons (n=2)
Analyzed (n=30)
♦Exclusion Ø
Loss to follow-up Ø Group P+100 mmHg (n=30)
♦Received intervention (n=30)
Loss to follow-up Ø Group 350 mmHg (n=30)
♦Received intervention (n=30)
Analyzed (n=30)
♦Exclusion Ø
Allocation
Analysis
Follow-up
Randomization (n=60)
Recruitment
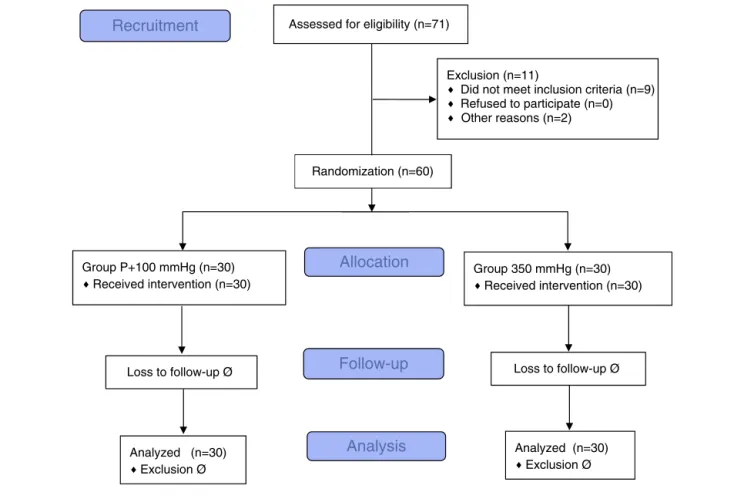
Fig.2–CONSORTflowchart.
tourniquetpressuresof350mmHg,and inthe othergroup, with 100mmHg above systolic blood pressure (SBP). Sec-ondarily,bloodloss,surgicalwoundcomplications,andthe rangeofmotion(ROM)oftheoperatedkneewere assessed. Thereafter,thesaferandmoreadvantageousmethodforthe patientswasdetermined.
Materials
and
methods
Thiswas a randomized clinical study;the main investiga-torwas blindedtothe pressure that wouldbe usedinthe tourniquet.ThisstudywasconductedfromSeptember2014to September2015,including60patientsundergoingTKA.The studyfollowedtherulessetforthbytheConsolidated Stan-dardsofTestingReports(CONSORT,whichwasdevelopedby aninternationalgroupofclinical,statisticians, epidemiolo-gists,andbiomedicaljournalspublishersinordertoimprove therecordingofrandomizedclinicaltrialsandthusallow read-erstounderstandthe study design,behavior analysis,and interpretationthroughfulltransparency)(Fig.2).6,7
Aprotocolwascreatedforthestudy.Patientswhomet eli-gibilitycriteriaforTKAinthisstudywererandomlyassigned, regardlessofage,sex,anddeformity,intotwogroups,through simple drawing by one of the authors, who did not par-ticipate insurgery. Inthe first group, Standard, tourniquet pressure on the thigh root was 350mmHg; in the second group,P+100,utilizingtourniquetpressures100mmHgabove
the last SBP measured beforeentering the operating room (process doneinthe recoveryroom). Thegroupswere ran-domized as follows: 60 Post-it®(3M doBrasil, Sumaré,SP) sheets, 101mm×101mm,ofthesame color,were used.On 30ofthem,theword“Standard”waswritten;ontheother30, “P+100.”Thesheetsweretwicefoldedandplacedintoacloth bag.Then,sheetsweredrawnasthepatientswereoperated; if thesurgerywassuspendedforany reason,sheetswould bereturnedtothebag.Thus,theStandardgroupconsisted of30patients,sevenmalesand23females,mean65.4years, standard deviation(SD)±8.6years.In the groupP+100, 30 patientswereincluded,eightmaleand22female,withamean ageof66years(SD±7years).Varusdeformitywaspresentin 83.3%ofcases;valgusdeformitywasobservedin16.7%ofall patients.
The study included patients regularly registered in the institution where the study was performed, who met the classical indication for TKR, namely: medial or lateral impingement with obliteration of the joint space; varus femorotibial alignment greater than 15◦; valgus
femorotib-ial alignment greater than 10◦; tibiofemoral subluxationin
thefrontalplanegreaterthan10mm;anteriorizationofthe tibiarelativetothefemurintheprofileX-ray;severe impair-ment oftwo ofthe threejoint compartments ofthe knee (medialtibiofemoral,lateraltibiofemoral,orpatellofemoral),8
Table1–Bruner’stenrulesforthesafeuseofthe tourniquet(asrecommendedbyKuttyandMcElwain).11
Application Onlyinhealthylimbs,orwithcautionin involvedlimbs.
Sizeofthetourniquet Arm10cm;thigh15cmorlargerinlarger thighs.
Applicationsite Proximalarm;proximalthigh. Padding Atleasttwolayersoforthopediccotton. Skinpreparation Avoidsoakingthecotton(thetourniquet
shouldbeoccluded).
Pressure 50–100mmHgabovesystolicforthearm;
doublesystolicforthethigh;or 200–250mmHgonthearm; 250–350mmHgonthethigh. Time(duration) Maximum3h(recoversin5–7days);
generally,donotexceed3h.
Temperature Avoidheating;coldiffeasible;thesurgical fieldshouldbekeptmoist.
Documentation Durationandpressure. Calibration Atleastweekly,withamercury
manometer.
Maintenance Quarterly.
agewasnottakenintoaccount,butrathertherealdamageto thekneejoint:patientshadtohaveadiagnosisofmoderate ormoreseverearthrosis(ÄhlbackmodifiedbyKeys≥III).9,10
Exclusioncriteriacomprisedpatientswithdecompensated diabetesmellitus(fastingbloodglucose >140mg/dL), uncon-trolled hypertension (SBP>200mmHg), peripheral vascular disease,previousthromboembolism,activeneoplasia, infec-tion, rheumatoid arthritis, obese with a body mass index greaterthan35kg/m2,orthosewithahighsurgicalrisk
(Amer-icanSocietyofAnesthesiologists[ASA]score>III);thosewho evolvedwithseverecomplications;andthosewhorefusedto signordidnotunderstandtheinformedconsentform.
For the application oftourniquet, Bruner’sten rules for thesafeuseofthetourniquet(arecommendedbyKuttyand McElwain),showninTable1,werefollowed.11Thetourniquet
usedinallpatientswasa12.5-cmwideScandmedElectronic Tourniquet600-20®(ScandmedAB,Stockholm,Sweden).
Patients underwent spinal anesthesia according to the protocols of the anesthesiology service of the institution (anesthesiologistswereblindedtothepurposeofthestudy). Afteranesthesia,thepneumatic tourniquetwasappliedon thethighrootofthelimbtobeoperatedoveralayerof ortho-pediccotton,inordertoprotecttheskin.Surgicaltechnique usedwasthestandardforTKR,withjointaccessviatheclassic trans-quadricepsapproachandpatellareversion.Theroutine intheserviceistheuseofintramedullaryguidesforfemoral cutsandextramedullaryguidesfortibialcuts.Thedecision ofwhether or nottospare the posteriorcruciate ligament (PCL)wasmadeinaccordancewiththeintraoperative find-ings,deformities,andsofttissuebalance.Patellarresurfacing afterlocaldenervationandsynovectomyisaroutinepractice inthisserviceinordertoavoidclunksyndrome;thecasesin whichthepatellawasnotresurfacedwereduetothe thick-ness(<18mm),butthesewereeburnated,neurotized,anda lateralfacetectomywasperformed.Theprosthesisusedwas theModularIII®(MDT,RioClaro,SP,Brazil),eitherPCL-sparing
ornot.Portovacsuctiondrainsof3.2-mmdiameterwereused, allocatedintraarticularlyand deeplyintothe subcutaneous
Moderate Mild
Visual analogue scale – VAS
Intense
Fig.3–Visualanalogscale(VAS).
tissue;afterthesutures,aninguinal-malleolarcompressive occlusiveRobertJonesdressing wasmade.Ifsurgerylasted over twohours, thetourniquet wasdeflated;subsequently, hemostasiswasassessed,andaprocesssimilartothe pre-vious was performed (drainsand dressings).Mean timeof ischemiawas118.5miningroupP+100mmHgand110min intheStandardgroup.Surgerieswere alwaysperformedby theprincipalinvestigatororunderhisdirectassistance.
At 24 and 48h postoperatively, the outputs of the suc-tiondrainswereassessed;dressingswerechangedanddrains were removed 48hafter the procedure bythe author who did notdraw the groups. Subsequently, pain wasassessed using the VAS (Fig. 3)with no joint manipulation; passive ROM and the surgical wound were assessed. According to theirclinicalconditions,patientsreceivedthesame analge-siaprotocol(tenoxicam20mgevery12h,tramadol50mgIV every 8h, dipyrone1gIVevery 6h),and rehabilitation. On thefifthday,patientswereassessedagainforpain,ROM,and surgical woundappearance; theywere dischargedas toler-atedandreferredtothephysiotherapyservice.Onthe15th day,thesestandardswerere-assessedinanoutpatient con-sultationandrecordedintheprotocol.Allpatientsreceived thromboprophylaxis with dabigatranat a dose adjustedto ageandrenalfunctionfor15days(220mgor15mg/day).All patientsreceivedprophylaxisforsurgicalsiteinfectionwith cefazolinsodiumatadoseof1gevery 8hforfivedays.
Thedatawerepresentedingraphsandtables,inwhichthe simpleandrelativeabsolutefrequencieswerecalculatedfor categoricaldata.Intheanalysisofquantitativedata,themean, standarddeviation(SD),and95%confidenceintervals(95%CI) werecalculated.However,whentheassumptionofdata nor-malitywasrejectedbytheShapiro–Wilktestatasignificance levelof5%(p<0.05),itwasdecidedtocalculatethemedianand quartiles(Qi).Whencomparingthemeansfortheparametric data,Student’st-testwasused.Inthemediananalysis,the nonparametricMann–Whitneytestwasused.Thesignificance levelwassetat5%.
Epi-Infosoftware,version7.4forWindows,wasusedfor statisticalanalysis.
Allpatientsreadandsignedtheinformedconsentform; the study was submitted to the Research Ethics Commit-tee(REC)oftheinstitution,withaCertificateofPresentation for Ethical Assessment (CAAE): 36658014.2.0000.0007, and receivedRECopinionNo.869.472.
Results
Table2–Summaryofpatientassessments.
Tourniquetpressure(mmHg)
Variables(n=60) P+100 350
fi % fi % Total p
Sex 0.766a
Female 22 48.9 23 51.1 45
Male 8 53.3 7 46.7 15
Age(years) 0.794b
Mean±SD 66.0±7.0 65.4±8.6
Complications 0.612c
Yes 1 3.3 3 10.0 4
No 29 96.7 27 90 56
VAS2ndPOD 0.625d
Median 2.0 2.0
Q1–Q3 0.5–3.0 0.5–4.0
VAS5thPOD 0.571d
Median 2.0 1.0
Q1–Q3 1.5–3.0 0.5–3.0
VAS15thPOD 0.195d
Median 2.0 3.0
Q1–Q3 1.0–3.0 1.5–5.0
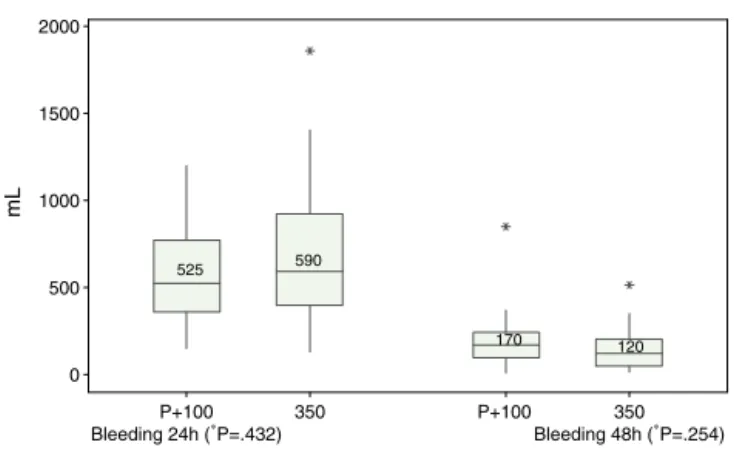
Bleeding24h 0.432d
Median 525.0 590.0
Q1–Q3 380–760 450–900
Bleeding48h 0.254d
Median 170.0 120.0
Q1–Q3 105–240 55–180
fi,simpleabsolutefrequency;SD:standarddeviation;Qi,quartile;VAS,visualanalogscale;TKA,totalkneearthroplasty. a Pearson’schi-squaredtest.
b Student’st-test.
c Fisher’sexacttest.
dMann–Whitneytest.
Standard group, with no statistically significant difference (p=0.612).TheVASinthesecond,fifth,and15thpostoperative days(POD)alsoshowednostatisticallysignificantdifferences (p=0.625; 0.571; 0.195; respectively). Bleeding through the suction drain at 24 and 48h also showed no statistically significant differencesin bothgroups, ascalculated bythe Mann–Whitneytest(Table2).TheVASand bleedingresults arebetterrepresentedintheboxplotsinFigs.4and5, respec-tively. ROM was not significantly different in both groups (Table3).Nocorrelationwasobservedbetweenischemiatime
and the following variables:VAS on the second, fifth, and 15thPOD,andbleedingat24and48h(Table4),showingno statisticalsignificance.
Discussion
Thehistoryofasurgicalspecialtyislargelywrittenaround the recordsofits technicaladvances.Comparedwithother paraphernaliainthemodernsurgicalarsenal,thepneumatic
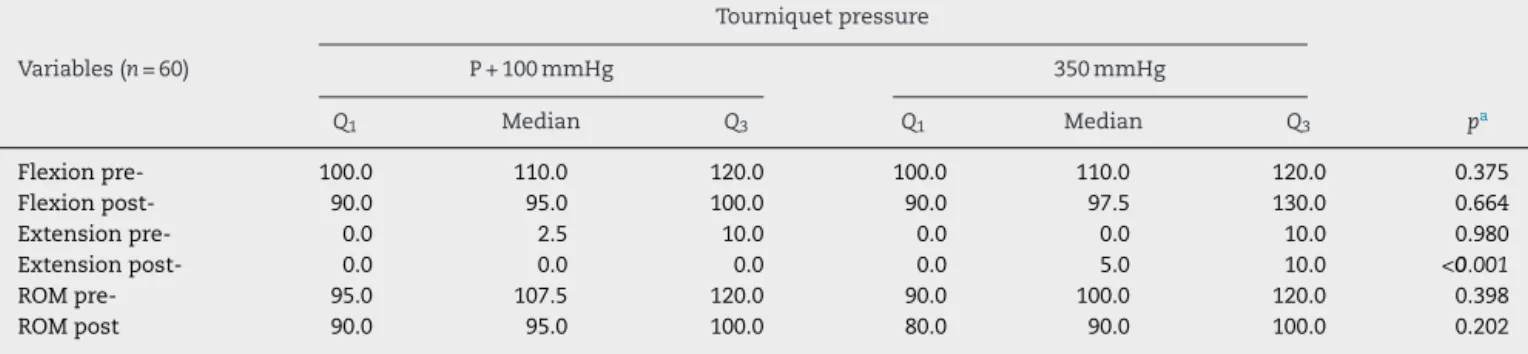
Table3–Distributionaccordingtothemedianofflexion,extension,andROMregardingtourniquetpressureinpatients undergoingTKA.
Tourniquetpressure
Variables(n=60) P+100mmHg 350mmHg
Q1 Median Q3 Q1 Median Q3 pa
Flexionpre- 100.0 110.0 120.0 100.0 110.0 120.0 0.375
Flexionpost- 90.0 95.0 100.0 90.0 97.5 130.0 0.664
Extensionpre- 0.0 2.5 10.0 0.0 0.0 10.0 0.980
Extensionpost- 0.0 0.0 0.0 0.0 5.0 10.0 <0.001
ROMpre- 95.0 107.5 120.0 90.0 100.0 120.0 0.398
ROMpost 90.0 95.0 100.0 80.0 90.0 100.0 0.202
p-Valueinbolditalicsindicatesstatisticaldifferenceofthemediansat5%significancelevel.
350 (∗
P=.195) P+100 VAS
15th POD 350
(∗ P=.571) P+100 VAS
5th POD 350
(∗ P=.625) P+100
VAS 2nd POD 9 8 7 6 5 4 3 2 1 0 Score 2 2 1 2 3 2
∗ Mann-Whitney test
Fig.4–BoxplotofthemedianVASinrelationtotourniquet pressureinpatientsundergoingTKA.VAS,visualanalog scale;TKA,totalkneearthroplasty;POD,postoperativeday.
350 Bleeding 48h (∗
P=.254) P+100
350 P+100
Bleeding 24h (∗ P=.432) 2000 1500 1000 500 0 mL 590 525 120 170
∗Mann-Whitney test
Fig.5–Boxplotofthemedianbleeding(24and48h)in relationtotourniquetpressureinpatientsundergoingTKA. TKA,totalkneearthroplasty.
tourniquet isa simple instrument. However,it has played animportantrole inimproving the accuracyoforthopedic surgery.Despitebeingarelativelysimpledevice,the tourni-quet leads to many potential dangers and its application shouldbeentrustedonlytoexperiencedprofessionals.12
In1995,Abdel-SalamandEyres13statedthatthe
complica-tionsrateinTKAswithouttheuseofatourniquetwaslower
Table4–CorrelationofischemiaandVAS2ndPOD,VAS 5thPOD,VAS15thPOD,andbleeding.
Ischemiatime
Variables(n=60) R pa
VAS2ndPOD −0.18 0.174
VAS5thPOD 0.21 0.102
VAS15thPOD 0.13 0.318
Bleeding24h −0.02 0.882
Bleeding48h −0.08 0.558
R,correlationcoefficient;VAS,visualanalogscale;POD, postopera-tiveday.
a t-Testforcorrelation.
than whensurgeryutilizedischemia,inwhichtherewasa significant reductioninpostoperative pain andfaster knee recovery.Thenon-useofatourniquetinTKAshowedno ben-efit,exceptaslightlyfasterrecoveryfrompostoperativepain. Whenusingatourniquetinthissurgery,surgeonsshould carefullyconsideritsefficacyandsafety.Inflatingthe tourni-quetonlyduringcementationorforalimitedtimemightbe anoption.Furtherwell-designedrandomizedcontrolled tri-alsareneededtoclarifytherolesandcomparetheeffectsof differentmethodsoftourniquetapplicationinTKAs.14
Worlandetal.15reachedsimilarconclusions,butwitha
dif-ferentmethodthanthatofthepresentstudy;thoseauthors recommendedthe useofthe tourniquetwithapressureof 100mmHgabovethesystolicbloodpressureforTKA,which wassuitableforcreatingabloodlesssurgicalfieldandresulted inless post-operative pain,data thatare supported bythe presentstudy.
In 2012,Taiet al.,16 in aprospective,randomized,
well-controlled study,concluded that the use ofthe tourniquet inTKAreducessurgicaltimeandbloodloss;italsoprevents inflammationandexcessivemuscledamage.
Thegreatcurrentcontroversyisaboutwhetherornotto usethetourniquet.Inarecentmeta-analysis,Nikolaouetal.17
concludedthattheanswer tothisdilemmaisstilldifficult, despitetheextensiveresearchonthesubject.Clearly,several issuesconcerningtheuseofatourniquetarise;theyrelate,for example,thebesttimetoreleasethepressureandthe opti-malphasesofthesurgeryforitsinflation.Inameta-analysis, Zhangetal.18showedthatthenon-useofatourniquetinTKA
improvedclinicaloutcomesregardingtheincidenceof com-plicationsandROMintheimmediatepostoperativeperiod.In thepresentstudy,therewasnosignificantdifferencebetween groupsregardingtheactualbloodloss.Therefore,theefficacy andsafetyofuseofthetourniquetinTKAneedstobe con-sidered,andsurgeonsshoulduseitprudently.However,the dataassessedinthepresentstudydidnotdisclosedifferences regardingbloodloss.
Complicationshavealwaysbeenpresentwiththeuseof tourniquets.OdinssonandFinsen19observedacomplication
rate similartothat ofthe 1970s.Castropilet al.20 reported
acaseoffemoralnerveinjuryinwhichthepressureofthe tourniquet was withinthe indicatedrange, and it had not been re-inflated.Thisdemonstratesthat evenwhenall the inflationparameters described assuitableforknee surgery are followed,thereisstillariskforcomplications. Numeri-cally,thegroupinwhichthepressureofthetourniquetwas 350mmHgpresentedmorecomplications,butwithout statis-ticalsignificance(p=0.612).
Olivecronaetal.21usedatechniquecalled“occlusion
Noordinetal.1andSharmaandSalhotra4gavean
excel-lent explanationabout the use oftourniquets, withfuture guidelines, and summarized that higher pressures on the tourniquet are associated with a higher associated risk of nervedamage.IshiiandMatsuda22recommendedapressure
of100mmHgabovesystolicpressure,insteadofthe conven-tional350mmHg,inordertoobtainasufficiently bloodless surgicalfieldandminimizepotentialcomplications,factsthat wereobservedinthestudy,inwhichsurgerywasperfectly fea-siblewithlowerpressuresandtherewasageneralperception offasterrecoverywithnoevidenceofmajorbleeding.
Souza Leão et al.,23 in a national publication, assessed
onlythe bloodlosswiththe releaseofthetourniquetafter cementationorpreparationofdressings,withouttakinginto accounttheinsufflationpressure.Theyconcludedthatthere werenostatisticallysignificantdifferencesregarding hema-timetriclevelsandbloodlossfromthesuctiondrain;when differentcuffpressureswerecompared,therewasno differ-enceinbloodloss,asdemonstratedinthepresentstudy.
Wakankaret al.24 concludedthatthe use ofthe
tourni-quetissafeandthatthepracticecanbemaintained.There wasnosignificantdifferenceinoperativetime,postoperative pain,needforanalgesia,volumecollectedinthedrains, post-operativeedema,and incidenceofwoundcomplicationsor deepveinthrombosis;similarresultsintheevaluated param-eterswereobservedinthepresentstudy.Itissurgicalskill thatconsiderablyreducessurgicaltimeandconsequentlythe tourniquet use; furthermore, lower complication rates are observed.
Unveretal.25showedthattheapplicationofthetourniquet
withlowerinflationpressurecanminimizethecomplications ofitsuseandthatpatientsregainfunctionalmobilityfaster. TheirdatawascorroboratedbyPapaliaetal.,26whoindicated
thattheuseofthetourniquetdoesnotleadtoasignificant increaseintheriskofmajorcomplications,butwithnoclinical differenceinthemedium-termresults.
TheVASisavalidinstrumentformeasuringpainata spe-cificpointintime. However,paininVAS isnotlinear,and receptivitycanvary dependingonthepeculiaritiesofpain. Consequently,minimallyimportantclinicaldifferenceseither alterthescoresingeneraloroverestimatethetruechange.27
Limiting factors ofthe present study include the short patientfollow-upaftersurgery,eventoassessother compli-cationssuchasdeepveinthrombosis,whichusuallyappears within30days,but the patientswere nolongerentered in thestudyprotocol;andtheabsenceofmusclestrengthtests, asassessingtherealdamagecausedbythetourniquet,joint function,andtheresultofthesurgerythroughspecificscores forthispurposewerenotamongthestudyobjectives.Finally, itmaybeoccasionallydifficulttoassesspainusingtheVAS, aspatientsmayhavedifficultyunderstandingwheretolocate themselvesinordertoquantifytheirpain.
Conclusions
Withthepresentdata,nodifferenceswere observedinthe groupsstudied regardinglevel ofpain byVAS, the volume of bleeding through the suction drain, and knee ROM; it was alsonotpossibleto correlatethese variables withthe
ischemiatime.Thecomplicationratewasnumericallyhigher inthegroupinwhichthepressureofthepneumatic tourni-quetwas350mmHg,butwithoutstatisticalsignificance.Thus, pressuresofupto350mmHginthetourniquetaresafe;ifthe surgeonchoosestouselowerpressures,thesewillnot hin-der thesurgerynorgenerateanymajorbleeding.Pressures shouldbeindividualizedforpatients;complicationsaremuch morerelatedtosurgeon’sexperiencethantothetourniquet pressuresused,aslongastheappropriateparametersare fol-lowed.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.NoordinS,McEwenJA,KraghJFJr,EisenA,MasriBA.Surgical tourniquetsinorthopaedics.JBoneJointSurgAm.
2009;91(12):2958–67.
2.TetroAM,RudanJF.Theeffectsofapneumatictourniqueton bloodlossintotalkneearthroplasty.CanJSurg.
2001;44(1):33–8.
3.PedowitzRA.Tourniquet-inducedneuromuscularinjury.A recentreviewofrabbitandclinicalexperiments.ActaOrthop ScandSuppl.1991;245:1–33.
4.SharmaJP,SalhotraR.Tourniquetsinorthopedicsurgery. IndianJOrthop.2012;46(4):377–83.
5.WewersME,LoweNK.Acriticalreviewofvisualanalogue scalesinthemeasurementofclinicalphenomena.ResNurs Health.1990;13(4):227–36.
6.TheCONSORTGroupConsolidatedStandardsofReporting Trials–CONSORT.Availablein: http://www.consort-statement.org[accessed02.12.14].
7.SchulzKF,AltmanDG,MoherD.CONSORTGroup2010 statement:updatedguidelinesforreportingparallelgroup randomizedtrials.AnnInternMed.2010;152(11):726–32.
8.CamanhoGL,OliviR,CamanhoLF.Artroplastiatotaldejoelho empacientesidososportadoresdeosteoartrose.RevBras Ortop.1998;33:271–4.
9.AhlbäckS.Osteoarthrosisoftheknee.Aradiographic investigation.ActaRadiolDiagn(Stockh).1968;Suppl. 277:7–72.
10.KeyesGW,CarrAJ,MillerRK,GoodfellowJW.Theradiographic classificationofmedialgonarthrosis.Correlationwith operationmethodsin200knees.ActaOrthopScand. 1992;63(5):497–501.
11.KuttyS,McElwainJP.Paddingundertourniquetsintourniquet controlledsurgery:Bruner’stenrulesrevisited.Injury. 2002;33(1):75.
12.KlenermanL.Thetourniquetinsurgery.JBoneJointSurgBr. 1962;44-B:937–43.
13.Abdel-SalamA,EyresKS.Effectsoftourniquetduringtotal kneearthroplasty.Aprospectiverandomisedstudy.JBone JointSurgBr.1995;77(2):250–3.
14.TaiTW,LinCJ,JouIM,ChangCW,LaiKA,YangCY.Tourniquet useintotalkneearthroplasty:ameta-analysis.KneeSurg SportsTraumatolArthrosc.2011;19(7):1121–30.
15.WorlandRL,ArredondoJ,AnglesF,Lopez-JimenezF,Jessup DE.Thighpainfollowingtourniquetapplicationin
simultaneousbilateraltotalkneereplacementarthroplasty.J Arthroplasty.1997;12(8):848–52.
kneearthroplasty:arandomizedcontrolledtrial.JBoneJoint SurgAm.2012;94(24):2209–15.
17.NikolaouVS,ChytasD,BabisGC.Commoncontroversiesin totalkneereplacementsurgery:currentevidence.WorldJ Orthop.2014Sep18;5(4):460–8.
18.ZhangW,LiN,ChenS,TanY,Al-AidarosM,ChenL.The effectsofatourniquetusedintotalkneearthroplasty:a meta-analysis.JOrthopSurgRes.2014;9(1):13.
19.OdinssonA,FinsenV.Tourniquetuseanditscomplicationsin Norway.JBoneJointSurgBr.2006;88(8):1090–2.
20.CastropilW,BitarAC,BrottoMWI,D’EliaCO,SchorB,Luques IU.Neurapraxiadofemoralpelousodogarrote:relatode caso.RevBrasOrtop.2008;43(11/12):513–5.
21.OlivecronaC,PonzerS,HambergP,BlomfeldtR.Lower tourniquetcuffpressurereducespostoperativewound complicationsaftertotalkneearthroplasty:arandomized controlledstudyof164patients.JBoneJointSurgAm. 2012;94(24):2216–21.
22.IshiiY,MatsudaY.Effectoftourniquetpressureon perioperativebloodlossassociatedwithcementlesstotal
kneearthroplasty:aprospective,randomizedstudy.J Arthroplasty.2005;20(3):325–30.
23.SouzaLeãoMG,SouzaHAP,FerreiraYMC.Avaliac¸ãodaperda sanguíneaapósaliberac¸ãoprecoceoutardiadaisquemiaem pacientessubmetidosàartroplastiatotaldojoelho.RevBras Ortop.2013;48(2):152–8.
24.WakankarHM,NichollJE,KokaR,D’ArcyJC.Thetourniquet intotalkneearthroplasty.Aprospective,randomisedstudy.J BoneJointSurgBr.1999;81(1):30–3.
25.UnverB,KaratosunV,TuncaliB.Effectsoftourniquet pressureonrehabilitationoutcomesinpatientsundergoing totalkneearthroplasty.OrthopNurs.2013;32(4):217–22.
26.PapaliaR,ZampognaB,FranceschiF,TorreG,MaffulliN, DenaroV.Tourniquetinkneesurgery.BrMedBull. 2014;111(1):63–76.