w w w . r b o . o r g . b r
Original
article
Femoropatellar
radiographic
alterations
in
cases
of
anterior
cruciate
ligament
failure
夽
Diego
Protásio
de
Vasconcelos
a,∗,
Alan
de
Paula
Mozella
b,
Pedro
Guilme
Teixeira
de
Sousa
Filho
b,
Gustavo
Cardilo
Oliveira
b,
Hugo
Alexandre
de
Araújo
Barros
Cobra
baOrthopedicsandTraumatologyService,UniversityHospital,FederalUniversityofSergipe,Aracaju,SE,Brazil bKneeSurgeryCenter,NationalInstituteofTraumatologyandOrthopedics(INTO),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8September2013 Accepted17October2013 Availableonline31January2015
Keywords:
Jointinstability
Anteriorcruciateligament Patellofemoraljoint
a
b
s
t
r
a
c
t
Objective:Tomakeacomparativeanalysisonthreefemoropatellarradiographicparameters, betweenkneeswithchronicfailureoftheanteriorcruciateligament(ACL)andnormalknees.
Methods:ThirtyvolunteerpatientswithadiagnosisofunilateralisolatedchronicACLinjury formorethanoneyearandanormalcontralateralkneewereselected.Digitalradiographs wereproducedforallthepatients,onbothkneesinabsolutelateralviewat30◦of
flex-ion,withandwithoutload-bearingononeleg,andinaxialviewofthepatellaat30◦.The
Caton–Deschampspatellarheightindex,MerchantpatellarcongruenceangleandLaurin lat-eralpatellartiltangleweremeasuredontheradiographsobtainedfromthenormalknees andkneeswithACLinjuries,andcomparativeanalysiswasperformedbetweenthesetwo groups.
Results:Thepatellarheightwasstatisticallysignificantlylower(p<0.001)inthekneeswith ACLfailurethaninthenormalknees,bothonradiographswithoutloadingandonthose withsingle-footloading.TheMerchantpatellarcongruenceanglewassignificantlysmaller (p<0.001)inthenormalkneesandthelateralpatellartiltanglewassmaller(p<0.001)inthe kneeswithACLfailure.
Conclusion: Chronic ACL failure gave rise to a statistically significant change in the femoropatellarradiographicvaluesstudied(p<0.001).Kneeswithinjuriestothisligament presentedlowerpatellarheightvalues,greatertiltandlateraldisplacementofthepatella, inrelationtothefemoraltrochlea,incomparisonwiththenormalcontralateralknees.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedattheKneeSurgeryCenteroftheNationalInstituteofTraumatologyandOrthopedics(INTO),RiodeJaneiro,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.P.deVasconcelos).
http://dx.doi.org/10.1016/j.rboe.2015.01.005
Alterac¸ões
radiográficas
femoropatelares
na
insuficiência
do
ligamento
cruzado
anterior
Palavras-chave:
Instabilidadearticular Ligamentocruzadoanterior Articulac¸ãopatelofemoral
r
e
s
u
m
o
Objetivo: Análisecomparativadetrêsparâmetrosradiográficosfemoropatelaresentre joel-hoscominsuficiênciacrônicadoligamentocruzadoanterior(LCA)ejoelhosnormais.
Métodos: Foramselecionados30pacientesvoluntárioscomdiagnósticodelesãocrônica isoladaunilateraldoLCAhaviamaisdeumanoejoelhocontralateralnormal.Todosos pacientesforamsubmetidosaradiografiasdigitaisdeambososjoelhosnasincidências emperfilabsolutoa30◦deflexão,comesemcargamonopodal,eaxialdepatelaa30◦.
Forammensurados,nasradiografiasobtidas,oíndicedealturapatelardeCaton-Deschamps, oângulodecongruênciapatelardeMerchanteoângulodeinclinac¸ãolateraldapatela, descritoporLaurin,nosjoelhosnormaisenosjoelhoscomlesãodoLCAefoifeitaanálise comparativaentreessesdoisgrupos.
Resultados: Aalturapatelarfoiinferior,deformaestatisticamentesignificante(p<0,001), nosjoelhoscominsuficiênciadoLCAemcomparac¸ãocomosjoelhosnormais,tantonas radiografiassemcargaquantonascomcargamonopodal.Oângulodecongruênciapatelar deMerchantfoisignificativamentemenor (p<0,001)nosjoelhosnormaiseoângulode inclinac¸ãolateraldapatelafoiinferior(p<0,001)nosjoelhoscominsuficiênciadoLCA.
Conclusão: AinsuficiênciacrônicadoLCAalteroudeformaestatisticamentesignificante (p<0,001)osvaloresdosparâmetrosradiográficosfemoropatelaresestudados.Joelhoscom lesãodesseligamentoapresentarammenoresvaloresdealturapatelar,maiorinclinac¸ãoe deslocamentolateraisdapatelaemrelac¸ãoàtrócleafemoralcomparadoscomosjoelhos contralateraisnormais.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Anteriorcruciateligament(ACL)injuriesareamongthe com-monest knee injuries, with growing incidence due to the increasinglylarge numberofindividuals involvedinsports activities.1Failureofthisligamentcausesanteriorand
rota-tional instability of the knee, characterized by recurrent episodes ofanterior and rotational(i.e. internal rotational) subluxationofthetibiaoverthefemur.2Theseepisodesmay
causefunctionallossesandlimitsportspracticesandcertain activitiesofdailyliving.3
Significantbiomechanicalandkinematicalterationshave beenrecognizedoverrecentdecades,inkneeswithACL fail-ure. Laboratory studies on gait analysis have shown that knees with ACL injuriespresent greater internalrotation,4
less external rotation5 and increased medial translation
of the tibia over the femur,6 in comparison with normal
knees,duringthestance and swingphases ofgait.Several authors7–10 havestatedthatACLfailuregivesrisetolossof
tibiofemoralkinematicbalanceandcausesabnormal biome-chanicalbehavior,whichputsthekneeatriskofsecondary injuries.
Despitethelargenumberofstudiesthathaveexaminedthe effectsofACLinjuriesontibiofemoralkinematics,fewhave analyzedfemoropatellaralterationsinpatientswithfailure ofthisligament.9Baugheretal.11demonstratedthatpatients
withACLfailurepresentedirreversibleatrophyofthe quadri-cepsmuscleandwarnedofthepossibleconsequencesofthis forthepatellofemoraljoint.
According toHsiehet al.,12,13 alterations totibiofemoral
kinematicsthatresultfromACLinjuriesaffectthekinematics ofthepatellofemoraljointandcauseimbalanceofthe exten-sormechanismandabnormaldistributionofforcesbetween the patella and the femoral trochlea. These authors12,13
showedthattherewere increasesinlateraltranslation and lateralinclinationofthepatellainrelationtothefemur,after resectionoftheACLinthekneesofcadavers.Invivo,Vande Veldeetal.14demonstratedthatACLfailurealtersthecontact
areaandfemoropatellartracking.
Femoropatellarradiographicparametersmayaidin diag-nosingalterationsofthepatellofemoraljoint.Inthepresent study,wemadeacomparativeanalysisonthree femoropatel-lar radiographic parameters that are commonly used in clinicalpractice,withtheaimofdetectingdifferencesinthese parametersbetweenkneeswithchronicACLfailureand nor-malknees.
Methods
Table1–Inclusionandexclusioncriteriaofthesample.
Inclusioncriteria
1.Skeletallymatureindividualsundertheageof60years 2.DiagnosisofsingleunilateralACLinjurythathadoccurred morethan12monthsearlier
2.1.Anteriortranslationofthetibiaoverthefemurgreater than5mm,withoutanendpointinrelationtothe
contralateralknee,usingKT-1000.
2.2.Lachman,AnteriorDrawerandPivot-Shifttests positive
2.3.Otherligamentandmeniscustestsnegative
2.4.Magneticresonanceimaging(MRI)showingsingleACL injury
3.Contralaterallowerlimbandkneewithoutalterationson physicalexamination
4.Individualswhoagreedtoparticipateandsignedthefree andinformedconsentstatementofthestudy
Exclusioncriteria
1.Presenceofalterationsofanyorigin(congenital, traumatic,metabolic,inflammatoryordegenerative)that weregeneticallyinheritedoracquired,ineitherofthelower limbs,otherthanasingleACLinjuryinoneoftheknees 2.Presenceofadeformityofvarus,valgus,antecurvatum, recurvatumortorsionalnatureineitherofthelowerlimbs 3.Previoussurgeryineitherofthelowerlimbs
4.Pregnantwomen
lengthoftimewiththeACLinjurywas32months,ranging from14to70.
All the patients underwent digital radiography on both knees:thekneewithACLfailureandthenormalcontralateral knee.Five radiographswereproducedoneach patient:two (oneoneachknee)inabsolutelateralviewwithflexionof30◦, withoutloadingonthelowerlimb,performedwiththepatient inlateraldecubitusontheradiographictable;two(oneoneach knee)inabsolutelateralviewwithflexionof30◦,performed inanuprightstandingpositionwiththebodyweightborneon onefootonthesideradiographed;andoneaxialradiographof thepatella,coveringbothkneesinaccordancewiththe tech-niqueofMerchantetal.,15 butwiththekneesflexedat30◦,
insteadof45◦.
Allthe150digitalradiographsobtainedwereanalyzedby thesame examiner,usingtoolsformeasuringdistancesin millimetersand angles,withinthe DicomViewer® software
(Microdata,RiodeJaneiro,Brazil).
Thevaluesofthreefemoropatellarradiographic parame-terswererecorded:thepatellarheight,whichwasmeasured onthelateral-viewradiographsofthekneebymeansofthe methoddescribedbyCaton–Deschamps16(Fig.1);Merchant’s
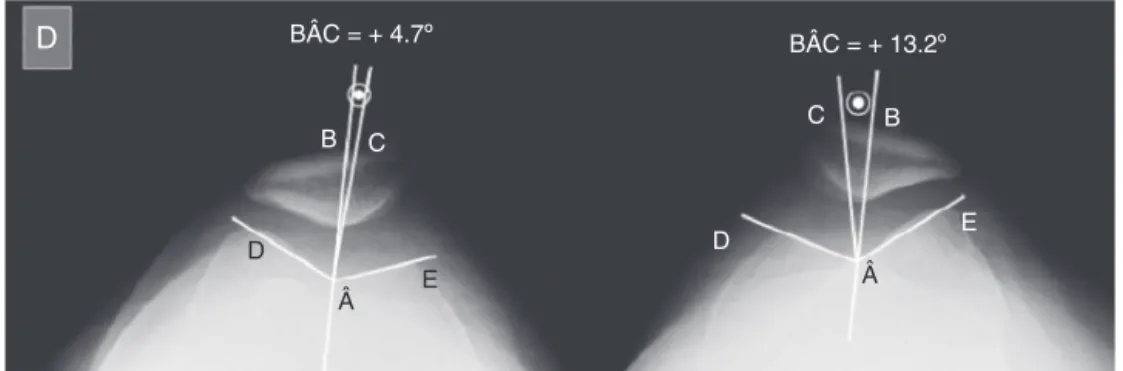
angleofpatellarcongruence,measuredonaxialradiographs ofthepatellaasdescribedbyMerchantetal.15(Fig.2);andthe
angleoflateralinclinationofthepatella,measuredin accor-dancewiththetechniqueofLaurinetal.17(Fig.3),onaxial
radiographsofthepatella.
Thevaluesofthefemoropatellarradiographicparameters obtainedfromthe kneeswithACL failure(case group)and fromthenormalcontralateralknees(controlgroup)were sub-jectedtotheKolmogorov–SmirnovandShapiro–Wilknormal distributiontests,andwerecomparedusingthepaired Stu-dent’sttesttoevaluatethestatisticalsignificance(p<0.05). Pearson’scorrelationtestwasusedtoassessthecorrelations
Left
A/B = 1.07
A B
Fig.1–Caton–Deschampspatellarheightindex(A/B)from radiographsofthekneeinabsolutelateralview:(A) distancebetweentheanteriormarginofthejointsurfaceof thetibiaandthelowerlimitofthejointsurfaceofthe patella;(B)distancebetweentheupperandlowerlimitsof thejointsurfaceofthepatella.
between thetime elapsedsinceACL injury andthe values forthepatellarheight,Merchant’scongruenceangleandthe lateralinclinationangleofthepatella.
Results
Among the 30 volunteers, 57% (n=17) were men and 43% (n=13)werewomen.Themeantimethathadelapsedsince theligamentinjurywas32±14months,witharangefrom14 to70.Thesubjects’meanagewas28±7.6years,rangingfrom 17to46.TheACLinjuriesweredistributedequallyonthetwo sides:50%(n=15)intherightkneeand50%(n=15)intheleft knee.Thetraumamechanismthatcausedtheligamenttear wasindirectin83%(n=25)anddirectin17%(n=5).The com-monestcausesweresoccerpractice(57%,n=17),fallsfroma height(16.5%,n=5),trafficaccidents(16.5%,n=5)andmartial artspractice(10%,n=3).
Themeanvaluesforthepatellarheightinthetwogroups, withoutweight-bearingonthelowerlimbandwith weight-bearingonasinglefoot,areshowninFigs.4and5.Thepatellar heightvalueswerestatisticallysignificantlysmaller(p<0.001) intheknees withACL failure(casegroup)than inthe nor-malknees(controlgroup),bothontheradiographswithout weight-bearingandinthosewithweight-bearingonasingle foot.Single-footweight-bearinggaverisetoastatistically sig-nificanceincrease(p<0.001)inthepatellarheightvaluesin thetwogroupsinasimilarmanner(Fig.5).
BÂC = + 4.7º BÂC = + 13.2º
B
D
 Â
D
E
D E
C C B
Fig.2–Merchant’spatellarcongruenceangle(BÂC).LineCbisectstheangleDÂE,whichistheangleofthetrochlearsulcus. LineBjoinsthevertexoftheangleDÂEtothelowestpointofthepatellarcrest.BÂC=+4.7◦inthenormalkneeand
BÂC=+13.2◦intheleftkneewithananteriorcruciateligamentinjury.
 = 10.4º  = 6.9º
D
Fig.3–Lateralinclinationangle(Â)ofthepatellaasdescribedbyLaurinetal.,17formedbyalinethatjoinstheanterior limitsofthemedialandlateralfemoralcondylesandanotherlinetangentialtothelateralfacetofthepatella.Â=10.4◦in
thenormalrightkneeandÂ=6.9◦intheleftkneewithananteriorcruciateligamentinjury.
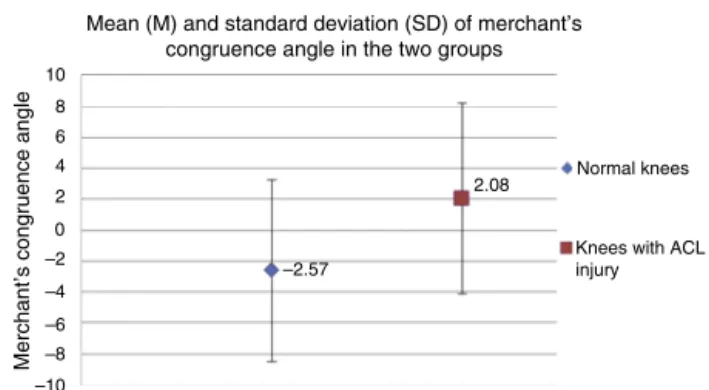
kneeswas−2.57◦±5.86◦.Thisvaluewasstatistically
signifi-cantlylower(p<0.001)thanthatofthekneeswithACLfailure (+2.08◦±6.16◦),asshowninFig.6.
The mean value of the lateral inclination angle of the patella in the group of knees with ACL injuries was 6.70◦±4.86◦,andthisvaluewassignificantlylower(p<0.001)
than thatofthenormalknees (11.25◦±4.54◦),asshown in
Fig.7.Table3presentsthemean,standarddeviationand max-imumandminimumvaluesofthelateralinclinationangleof thepatellaineachgroup.
2
1.5
Mean (M) and standard deviation (SD) of the patellar height without weight-bearing on the lower limbs in the two groups (p<0.001)
0.5
1.05
0.97 Normal knees
Knees with ACL injury
Patellar height without weight-bearing 0 1
Fig.4–Meanandstandarddeviationofthepatellarheight withoutweight-bearingonthelowerlimbsinthetwo groups.
Pearson’scorrelationtestdidnotshowanysignificant cor-relation(r=0.14)betweenthetimethathadelapsedsincethe ligamentinjuryandthevaluesforthepatellarheight, Mer-chant’spatellarcongruenceangleandthelateralinclination angleofthepatellainthekneeswithACLfailure.
Discussion
TheeffectsofACLfailureontibiofemoralkinematicsarewell documented in the literature. Rotational alterations4,5 and
translationalalterations6tothetibiofemoraljointduringthe
2
1.5
Mean (M) and standard deviation (SD) of the patellar height with weight-bearing on one foot only in the two groups (p<0.001)
0.5
1.11
1.03
Normal knees
Knees with ACL injury
Patellar height without weight-bearing 0 1
10 8 6 4 2 –2 –4 –6 –8 –10
Mean (M) and standard deviation (SD) of merchant’s congruence angle in the two groups
–2.57
2.08 Normal knees
Knees with ACL injury
Merchant’s congruence angle
0
Fig.6–MeanandstandarddeviationofMerchant’s congruenceangleinthetwogroups.
18 15 12 9 6 3 –3
Mean (M) and standard deviation (SD) of the lateral inclination angle of the patella in the two groups
11.25
6.70
Normal knees
Knees with ACL injury
Lateral inclination angle of the patella
0
Fig.7–Meanandstandarddeviationofthelateral inclinationangleofthepatellainthetwogroups.
stance and swing phasesof gait havebeen demonstrated. AccordingtoHsiehetal.,13alterationstotibiofemoral
kine-maticsinevitablycause changestothefemoropatellarjoint andmodifyitsnormalfunctioning.
Usingradiographicparametersthatarecommonlyapplied in clinical practice, we sought to detect these possible femoropatellaralterationsinkneeswithchronicACLinjuries alonethathadoccurredmorethan12monthsearlier.Forthis,
Table2–Mean,standarddeviation(SD)andminimum
andmaximumvaluesforMerchant’spatellar
congruenceangleinthetwogroups.
Merchant’spatellarcongruenceangle
Mean SD Min Max
Normalknees −2.57 5.86 −13.90 7.80
KneeswithACLinjuries 2.08 6.16 −13.20 13.20
Table3–Mean,standarddeviation(SD)andminimum
andmaximumvaluesforthelateralinclinationofthe patellainthetwogroups.
Lateralinclinationangleofthepatella
Mean SD Min Max
Normalknees 11.25 4.54 0.00 21.00
KneeswithACLinjuries 6.70 4.86 −4.80 14.80
weusedthenormalcontralateralkneeofthecamepatientas thecontrol.
Inanalyzingthepatellarheight,wefoundasignificantly lowervalue(p<0.001)inthegroupofkneeswithACLinjuries thaninthegroupofnormalknees.Ontheradiographswithout weight-bearing,theCaton–Deschampspatellarheightindex forthekneeswithACLinjurieswas0.97±0.11,whileitwas 1.05±0.09forthe normalknees(Fig.4).These valueswere verysimilartothoserecordedbyLinetal.,18whocompared
thepatellarheightwithoutweight-bearingonthelowerlimbs usingtheInsall-Salvatipatellarheightindex,inkneeswith ACL injury(0.99±0.11)and withoutACLinjury(1.05±0.12). Furthermore,theseauthors,andalsoAgliettietal.,19found
significantlylowerpatellarheightvaluesinmalepatientswith ACLinjuriesandconcludedthatalowpatellaisariskfactorfor ligamentinjury.Inoursample,wedidnotobserveany statis-ticallysignificantdifference(p>0.05)inpatellarheightvalues betweenmenandwomen.Moreover,sinceweusedthe con-tralateralnormalkneeofthesamepatientasthecontrol,we cannotsaywhetherthelowervaluesforpatellarheightthat wefoundinthekneeswithACLinjuryareariskfactorfor lig-amentinjury,orwhethertheyareaconsequenceofchronic injury.
Weight-bearingonasinglefootstatisticallysignificantly increasedthepatellarheightvaluesinbothgroups(p<0.01) (Fig. 5). Yiannakopouloset al.20 observedthat there was a
meanincreaseintheCaton–Deschampspatellarheightindex of0.11whenbodyweightwasbornebynormalknees.These authors suggested that the increasein patellar heightdue to proximal translation of the patella through contraction ofthequadricepswhenweightisbornebythelowerlimbs mightbegreaterinkneeswithligamentfailure.VandeVelde etal.14detectedrelativestretchingofthepatellartendonin
knees with ACL injury, which could theoretically cause an evengreaterincreaseinpatellarheightintheseknees dur-ingquadricepscontraction.However,inourstudy,themean increase in patellarheight was the same (0.06)in the two groups.
Merchant’spatellarcongruenceanglereflectstheposition ofthe patellainrelationtothe trochlearsulcus.Itsvalues canbenegative,whichindicatesthatthecrestofthepatella islocatedmediallytothetrochlearsulcus;orpositive,when the crest ofthe patella islocatedlaterally tothe trochlear sulcus.15Thus,themorepositivethevalueoftheangleis,the
greaterthelateraldisplacementofthepatellainrelationtothe femoraltrochleawillbe;andthemorenegativeitis,thegreater themedialdisplacementwillbe.Inourstudy,themeanvalue ofthisangleinthenormalkneeswas−2.57◦±5.86◦,versus
+2.08◦±6.16◦(p<0.001)inthekneeswithACLfailure,which
indicatesthatthepositioningofthepatellawasmorelateralin relationtothetrochlearsulcusinthegroupofkneeswith liga-mentlesions.Thisfindingisconcordantwithwhatwasfound byVandeVeldeetal.,14whorecordedgreaterlateral
displace-mentofthepatellainmillimeters,inrelationtothetrochlear sulcus,inkneeswithACLinjuriesatflexionsbetween0◦and
30◦.Onaverage,thelateraldisplacementofthepatellafound
bytheseauthors14was1.7mmgreater(p<0.001)inkneeswith
ACLfailurethaninnormalknees.Hsiehetal.13alsorecorded
 = – 4.8º  = + 5.9º
D
Fig.8–Negativelateralinclinationangle(Â)ofthepatella(Â=−4.8◦)intherightkneewithACLinjuryandpositiveangle (Â=+5.9◦)inthenormalleftknee.
flexionsbetween0◦ and 90◦, inthe kneesofcadaverswith
ligamentinjuries.
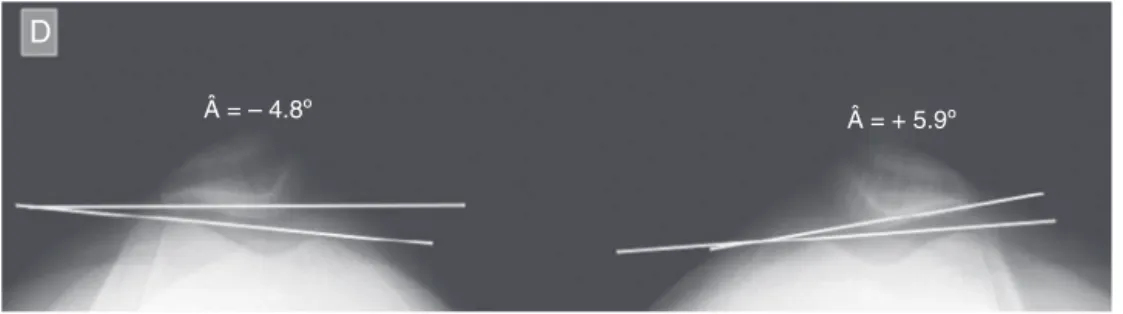
As the patella tilts laterally, there is a decrease in the lateralinclinationangleofthepatella,asdescribedby Lau-rinetal.17Thisoccursbecausethelinethatistangentialto
thelateralfacetofthepatellabecomesmoreparalleltothe linethat joinsthe anteriorlimitsofthe medialand lateral femoralcondyles.Incasesofseverelateraltilting,inversion of this angle may occur, thus becoming negative through medialopening,instead ofthrough lateral opening(Fig. 8). Inoursample,this inversionoftheangleonlyoccurred in two knees with ACL injuries (−2.2◦ and −4.8◦) and it was
notrecorded inany ofthe normalknees. Themean value ofthe lateral inclinationangle ofthe patella in the knees withACLinjurieswas6.70◦±4.86◦,whichwas significantly
smaller (p<0.001) than what was measured in the normal knees (11.25◦±4.54◦). These results reveal that there was
greater lateral tilting of the patella inthe knees withACL injuries,whichwasonaverage4.55◦greaterthaninthe
nor-malknees.SimilarvalueswerealsoreportedbyVandeVelde etal.,14whorecordedameanincreaseinlateraltiltingof5.2◦,
forthepatellaeofkneeswithACLinjuriesoverthefirst30◦of
flexion.
Thereisnoconsensusintheliteratureregardingwhether femoropatellar alterationsmightbe reversiblethroughACL reconstruction.Inthekneesofcadavers,Hsiehetal.12,13found
thatafterACLreconstruction, thepatellartilt,contactarea andfemoropatellarcontactpressurereturnedtovaluesclose tothoseofnormalknees.Ontheother hand,inaninvivo
study,VandeVeldeetal.14documentedthatthesealterations
persistedevenafterligamentreconstruction,whichsuggested thatthis procedure alone wouldnot becapableof correct-ingthem.Furtherresearchwillbeneededinordertoconfirm thesehypotheses.
Small changes to patella orientation in relation to the femoral trochlea may cause significant changes to femoropatellar biomechanics.14 According to some
authors,14,21,22 thegreater displacement and greater lateral
inclination ofthe patella found in knees with ACL failure mightberelated tothe appearanceofanterior paininthe kneeandfemoropatellararthrosis.
Webelievethatfemoropatellaralterationsinkneeswith ACLinjuriesorinthosethatundergoreconstructionofthis ligament are oftenunderdiagnosed in clinical practice. An appropriateradiological examinationwithdetailed analysis onthefemoropatellarradiographicparametersmightaidin
recognizingthesealterationsandenablerationaltherapeutic approaches.
Conclusion
In oursample,chronicACLfailurestatisticallysignificantly alteredthevaluesofthefemoropatellarradiographic param-etersevaluated(p<0.001).Kneeswithchronicinjuriestothis ligamentpresentedlowervaluesforpatellarheight,greater tiltingandgreaterlateraldisplacementofthepatellain rela-tiontothefemoraltrochlea,incomparisonwiththenormal contralateralknees.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.RistanisS,GiakasG,PapageorgiouCD,MoraitiT,StergiouN, GeorgoulisAD.Theeffectsofanteriorcruciateligament reconstructionontibialrotationduringpivotingafter descendingstairs.KneeSurgSportsTraumatolArthrosc. 2003;11(6):360–5.
2.DennisDA,MahfouzMR,KomistekRD,HoffW.Invivo determinationofnormalandanteriorcruciate ligament-deficientkneekinematics.JBiomech. 2005;38(2):241–53.
3.BuckwalterJA,LaneNE.Athleticsandosteoarthritis.AmJ SportsMed.1997;25(6):873–81.
4.GeorgoulisAD,PapadonikolakisA,PapageorgiouCD,Mitsou A,StergiouN.Three-dimensionaltibiofemoralkinematicsof theanteriorcruciateligament-deficientandreconstructed kneeduringwalking.AmJSportsMed.2003;31(1):75–9.
5.AndriacchiTP,DyrbyCO.Interactionsbetweenkinematics andloadingduringwalkingforthenormalandACLdeficient knee.JBiomech.2005;38(2):293–8.
6.DeFrateLE,PapannagariR,GillTJ,MosesJM,PathareNP,LiG. ThesixdegreesoffreedomkinematicsofthekneeafterACL deficiency:anin-vivoimaginganalysis.AmJSportsMed. 2006;34(8):1240–6.
7.AndriacchiTP,MundermannA,SmithRL,AlexanderEJ,Dyrby CO,KooS.Aframeworkfortheinvivopathomechanicsof osteoarthritisattheknee.AnnBiomedEng.2004;32(3):447–57.
itscorrelationwithcartilage-to-cartilagecontact.Clin Biomech(Bristol,Avon).2005;20(7):736–44.
9. LiG,DeFrateLE,ZayontzS,ParkSE,GillTJ.Theeffectof tibiofemoraljointkinematicsonpatellofemoralcontact pressuresundersimulatedmuscleloads.JOrthopRes. 2004;22(4):801–6.
10.VandeVeldeSK,DeFrateLE,GillTJ,MosesJM,PapannagariR, LiG.Theeffectofanteriorcruciateligamentdeficiencyonthe invivoelongationofthemedialandlateralcollateral ligaments.AmJSportsMed.2007;35(2):294–300.
11.BaugherWH,WarrenRF,MarshallJL,JosephA.Quadriceps atrophyintheanteriorcruciateinsufficientknee.AmJSports Med.1984;12(3):192–5.
12.HsiehYF,DraganichLF,HoSH,ReiderB.Theeffectsof removalandreconstructionoftheanteriorcruciateligament onpatellofemoralkinematics.AmJSportsMed.
1998;26(2):201–9.
13.HsiehYF,DraganichLF,HoSH,ReiderB.Theeffectsof removalandreconstructionoftheanteriorcruciateligament onthecontactcharacteristicsofthepatellofemoraljoint.Am JSportsMed.2002;30(1):121–7.
14.VandeVeldeSK,GillTJ,DeFrateLE,PapannagariR,LiG.The effectofanteriorcruciateligamentdeficiencyand
reconstructiononthepatellofemoraljoint.AmJSportsMed. 2008;36(6):1150–9.
15.MerchantAC,MercerRL,JacobsenRH,CoolCR.
Roentgenographicanalysisofpatellofemoralcongruence.J BoneJointSurgAm.1974;56(7):1391–6.
16.CatonJ,DeschampsG,ChambatP,LeratJL,DejourH.Patella infera:aproposof128cases.RevChirOrthopReparatrice ApparMot.1982;68(5):317–25.
17.LaurinCA,LevesqueHP,DussaultR,LabelleH,PeidesJP.The abnormallateralpatellofemoralangle:adiagnostic Roentgenographicsignofrecurrentpatellarsubluxation.J BoneJointSurgAm.1978;60(1):55–60.
18.LinCF,WuJJ,ChenTS,HuangTF.Comparisonofthe
Insall-Salvatiratioofthepatellainpatientswithandwithout anACLtear.KneeSurgSportsTraumatolArthrosc.
2005;13(1):8–11.
19.AgliettiP,InsallJN,CerulliG.Patellarpainandincongruence. I:Measurementsofincongruence.ClinOrthopRelatRes. 1983;(176):217–24.
20.YiannakopoulosCK,MataragasE,AntonogiannakisE.The effectofquadricepscontractionduringweight-bearingon fourpatellarheightindices.JBoneJointSurgBr.
2008;90(7):870–3.
21.ØiestadBE,HolmI,EngebretsenL,AuneAK,GundersonR, RisbergMA.Theprevalenceofpatellofemoralosteoarthritis 12yearsafteranteriorcruciateligamentreconstruction.Knee SurgSportsTraumatolArthrosc.2013;21(4):942–9.