ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Are
the
women
with
Sjögren’s
Syndrome
satisfied
with
their
sexual
activity?
Hatice
Isik
a,b,∗,
Metin
Isik
c,
Oner
Aynioglu
a,
Deniz
Karcaaltincaba
d,
Ahmet
Sahbaz
a,
Tugba
Beyazcicek
e,
Mehmet
Ibrahim
Harma
a,
Nejat
Demircan
eaBulentEcevitUniversity,SchoolofMedicine,DepartmentofObstetricsandGynecology,Zonguldak,Turkey bMevlanaUniversity,SchoolofMedicine,DepartmentofObstetricsandGynecology,Konya,Turkey
cBulentEcevitUniversity,SchoolofMedicine,DepartmentofRheumatology,Zonguldak,Turkey dGaziUniversity,SchoolofMedicine,DepartmentofObstetricsandGynecology,Ankara,Turkey eBulentEcevitUniversity,SchoolofMedicine,DepartmentofFamilyMedicine,Zonguldak,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25August2015 Accepted18May2016
Availableonline8February2017
Keywords:
Sjögren’ssyndrome Chronicdyspareunia Sexualdissatisfaction
a
b
s
t
r
a
c
t
Objective:FemaleswithSjögren’sSyndrome(SS)oftenexperiencevaginaldrynessand dys-pareunia,alongwithglandularandextraglandularsymptoms.Weaimedtoevaluatesexual functionandlifequalityinwomenwithSS.
Methods:Forty-six premenopausal women with SS and 47 age-matched controls were studied.Age,durationofthedisease,medications,andcomorbiddiseaseswerenoted. Par-ticipantscompleted36-ItemShortFormHealthSurvey(SF-36)andFemaleSexualFunction Index(FSFI).Patientswereaskedaboutvaginaldischargeanditchinginthelastmonth,andif theyinformedtheirrheumatologistsaboutanysexualproblems.Gynecologicexaminations wereperformedandvaginalsmearsweretakenoneachparticipant.
Results:ThemediantotalscoresofFSFIweresignificantlylowerintheSSgroupthanthe con-trols[17.12(2.4–27.8)and27.4(16.9–36.0),respectively,p<0.001].IntheSSgroup,37(80.4%) andinthecontrolgroup18(38.3%)ofpatientsweresexuallydissatisfied(p<0.001). Vagi-naldrynessandlubricantuseweresignificantlyincreasedinpatientswithSScompared tocontrols(p<0.001).LifequalityscoresweresignificantlylowerinpatientswithSSthan thecontrols(p<0.001).VaginaldrynesswasnegativelycorrelatedwithFSFItotal(r=−0.312,
p=0.035)andsubscoresexceptdesireandarousal.Physicalfunctioning,rolephysicaland roleemotionalscoreswerepositivelycorrelatedwithtotalFSFIscores(r=0.449,p=0.002,
r=0.371,p=0.011,r=0.299,p=0.043,respectively).
Conclusions:WomenwithSSexperiencelesssatisfactionwithsexualactivity,whichcanbe affectedbyage,vaginaldryness,physicalpain,andimpairedfunctionduetothedisease. Therefore,rheumatologistsshouldpayattentiontothesesymptomsandmanagement.
©2017ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mails:[email protected],[email protected](H.Isik).
http://dx.doi.org/10.1016/j.rbre.2017.01.002
2255-5021/©2017ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
As
mulheres
com
síndrome
de
Sjögren
estão
satisfeitas
com
sua
atividade
sexual?
Palavras-chave:
SíndromedeSjögren Dispareuniacrônica Insatisfac¸ãosexual
r
e
s
u
m
o
Objetivo: AsmulherescomsíndromedeSjögren(SS)muitasvezesexperimentamsecura vaginal e dispareunia, juntamentecom sintomas glandulares e extraglandulares.Este estudoobjetivouavaliarafunc¸ãosexualeaqualidadedevidademulherescomSS.
Métodos: Estudaram-se46mulherespré-menopáusicascomSSe47controlespareadospor idade.Avaliou-seaidade,adurac¸ãodadoenc¸a,osmedicamentosutilizadoseas comor-bidades.Asparticipantespreencheramoquestionáriodequalidadedevida36-ItemShort FormHealthSurvey(SF-36)eoFemaleSexualFunctionIndex(FSFI).Aspacientesforam questionadasquantoàpresenc¸adecorrimentoepruridovaginalnoúltimomês,esehaviam informadoseusreumatologistassobrequaisquerproblemassexuais.Realizaram-seexames ginecológicoseesfregac¸osvaginaisdetodasasparticipantes.
Resultados: AmedianadoescoretotaldoFSFIfoisignificativamentemenornogrupoSSdo quenogrupocontrole[17,12(2,4a27,8)e27,4(16,9a36,0),respectivamente,p<0,001].Nos gruposSSecontrole,37(80,4%)e18(38,3%)daspacientesestavamsexualmenteinsatisfeitas, respectivamente(p<0,001).Apresenc¸adesecuravaginaleousodelubrificantesforam sig-nificativamentemaisfrequentesempacientescomSSemrelac¸ãoaoscontroles(p<0,001). OsíndicesdequalidadedevidaforamsignificativamentemenoresnaspacientescomSS doquenoscontroles(p<0,001).Asecuravaginalestevenegativamentecorrelacionadocom oFSFItotal(r=-0,312p=0,035)ecomtodososseussubescores,excetodesejoeexcitac¸ão. Osescoresdecapacidadefuncional,aspectofísicoeaspectoemocionalsecorrelacionaram positivamentecomapontuac¸ãototaldoFSFI(r=0,449,p=0,002;r=0,371,p=0,011;r=0,299, p=0,043,respectivamente).
Conclusões: AsmulherescomSStêmmenorsatisfac¸ãocomaatividadesexual,oquepode serafetadopelaidade,securavaginal,dorfísicaefunc¸ãoprejudicadaemrazãodadoenc¸a. Portanto,osreumatologistadevemprestaratenc¸ãoaestessintomaseseutratamento.
©2017ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Sjögren’sSyndrome(SS)isacommonmultisystemic autoim-mune disease, which mainly affects exocrine glands. The clinicalsymptomsaredrynessofthemouthandeyes(sicca symptoms), due to dysfunction of salivary and lacrimal glands.1,2Extraglandularsymptomssuchasdisablingfatigue,
interstitiallungdisease,neurologicinvolvement,and arthri-tisarelessfrequentlydescribed.3InthehistopathologyofSS,
lymphocyticinfiltrationoftheaffectedorgansisseen.3SSis
asystemicdiseaseclassifiedasprimaryor secondary,each associatedwithspecificsymptoms.Rheumatoid arthritisis themaindiseaserelatedtosecondarySS.4
TheincidenceandprevalenceratesofprimarySjögren’s Syndrome (pSS) vary in different populations.5,6 In a
sys-temic review and meta-analysis, the overall prevalence of pSSwas60.82(95%CI43.69–77.94)casesper100,000 inhabi-tantsandtheoverallageofpSSpatientswas56.16years(95% CI52.54–59.78).7 FemalesareninetimesmoreatriskforSS
thanmen.8WomenwithpSSoftenexperiencevaginaldryness
and dyspareunia, along withglandular and extraglandular symptoms.8Chronicdyspareuniamaybethefirstpresenting
symptomofSSp.9Vaginaldrynessanddyspareuniaaffectlife
qualitymorethanotherSSsymptoms.10
SS is generally seen in sexually active women, which may havea seriousimpact on the patient’s qualityoflife;
these include emotional, functional, psychological, sexual, and reproductive health matters. Sexual health impacts many aspectsofanindividual’slife,involvingsexual activ-ityandsatisfaction.11Sexualdysfunctionhasbeenreported
in 24–72% of rheumatic disorders.12,13 In these diseases,
pain, fatigue, stiffness, functional impairment, depression, treatmentsideeffects,andreducedlibidocanaffectsexual functionaswell.14Vaginaldrynessanddyspareuniamay
cre-atesexualdissatisfaction.15
Previousstudieshavelargelyfocusedonvaginalsymptoms and dyspareunia,but onlyafewstudies highlightedsexual dysfunctionanddistress inwomenwithSS.12,13,16,17 Inthis
studyweaimedtoevaluatelifequalityandsexualdysfunction inagroupofTurkishwomenwithSS.Inaddition,weaimed toassess whether social,physicalandemotionalfunctions underminesexualfunctioninthesewomen.
Materials
and
methods
ThestudywasconductedfromJanuary2014toFebruary2016 inahospitalatastateuniversity,followingapprovalofthe localethicscommittee.PatientswithSSwerebetween28and 48yearsofage,andmettheAmericanCollegeof Rheumatol-ogy(ACR)2012classificationcriteriaforSS.17Postmenopausal
causeadecrease invaginallubricationsuchas antidepres-santsordiureticswereexcludedfromthestudy.Ofeightysix womenwho werediagnosedwithSS atrheumatology out-patientclinics,46ofthemwho agreedtoparticipatetothe studycomplyingourinclusioncriteria,includedinthestudy group. Age-matched 47 healthy, non-menopausal women wereincludedasacontrolgroup.Writteninformedconsent, compliantwiththeHelsinkiDeclaration,wasobtainedfrom allparticipants.
Age, menstrualstatus, duration ofthe disease, medica-tions, and comorbid diseases were noted in the medical records.Participantswere informedabout the scopeofthe study and asked to complete two questionnaires: 36-Item ShortFormHealthSurvey(SF-36)andFemaleSexualFunction Index(FSFI).Anyunclearquestionswereexplainedbythetwo authors(H.I.andT.B.).
Patienthealthqualitywasassessedwiththe36-ItemShort FormHealthSurvey(SF-36)questionnaire,whichconsistsof 36questionsand8subgroups;itisafrequently-usedscale, developedbyWareandSherbournein1992.Koc¸yigitetal.in 1999establisheditsvalidityandreliabilityforTurkishpeople. ThedomainsoftheSF-36arephysicalfunctioning,role phys-ical,bodilypain, generalhealth, vitality,socialfunctioning, roleemotionaland mentalhealth.Subjectsansweredall36 questionswithintheallowedmaximum10-minutetime.All domainswerescored,andthesumofsubscalescoreswas cal-culated.Thelowestandhighestpossiblescoreswereassigned as0and100,respectively,withthehighestscoreindicating betterlifequality.
The19-itemFSFIevaluatedthepatient’ssexualfunction, asreportedbyRosenetal.,18andvalidatedforTurkishpeople
byOksuz etal.in2005.19 Sexualfunctionismeasuredin6
subdomains:desire,arousal,orgasm,lubrication,satisfaction, andpain.Eachsubdomainiscalculated,withthesumyielding thetotalFSFI,rangingfrom2to36.19Acut-offscoreof<26
isseenassexualdysfunctionintheTurkishversion,20 with
higherscoresindicatingbettersexualfunction.
Patientswereaskedaboutvaginaldischargeanditchingin thelastmonth,oratexaminationtime,andaskediftheyhad informedtheirrheumatologistsaboutanysexualproblems. Gynecologicexaminationswereperformed oneach partici-pant,withvaginalsmearstakenatthesametime.Treatment wasgivenforanyinfections.
Statisticalanalysis
StatisticalanalyseswereperformedwithSPSS18.0software (SPSS Inc., Chicago,IL, USA). The distribution ofdata was determined viathe Shapiro–Wilk test.Categoricalvariables werepresentedasfrequencyandpercentagesand continu-ousvariableswerepresentedasmeanfollowedbystandard deviationandmedianwithmaximum–minimum.Continuous variableswereexpressedasmean±standarddeviation,and categoricalvariables were expressedasfrequencyand per-cent.Forstatisticalanalysis,independentsamplesttestand Mann–WhitneyUtestwereusedtocomparethecontinuous variablesandPearsonChi-squaretestwasusedtocompare categorical variables. Spearman’s Rho correlation test was used to evaluate the relationship between FSFI score, life
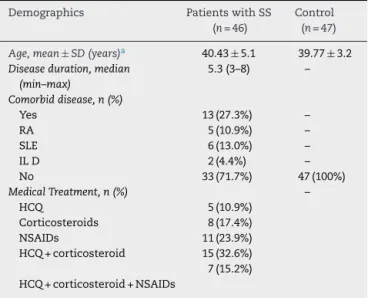
Table1–Demographicanddiseasecharacteristicsofthe patients.
Demographics PatientswithSS (n=46)
Control (n=47)
Age,mean±SD(years)a 40.43±5.1 39.77±3.2 Diseaseduration,median
(min–max)
5.3(3–8) –
Comorbiddisease,n(%)
Yes 13(27.3%) –
RA 5(10.9%) –
SLE 6(13.0%) –
ILD 2(4.4%) –
No 33(71.7%) 47(100%)
MedicalTreatment,n(%) –
HCQ 5(10.9%)
Corticosteroids 8(17.4%)
NSAIDs 11(23.9%)
HCQ+corticosteroid 15(32.6%)
HCQ+corticosteroid+NSAIDs
7(15.2%)
RA,rheumatoidarthritis;SLE,systemiclupuserythematosus;ILD, interstitiallungdisease;HCQ,hydroxychloroquine;NSAIDs, nons-teroidanti-inflammatorydrugs.
a p=0.674.
quality domains, and vaginal symptoms such as dryness, infectionanditching.
Results
DemographicanddiseasecharacteristicsareshowninTable1. There was no difference between the mean ages of SS patientsandthecontrols(40.43±5.1and39.77±3.2, respec-tively, p=0.674). The median disease duration was 5 (3–8) years.Approximatelythree-fourthsofSSpatientswerefree ofcomorbiddisease(71.7%).Rheumatoidarthritis,systemic lupuserythematosus(SLE),andinterstitiallungdisease(ILD) werecoexistingdiseaseswithSSin13(27.3%)ofthepatients.
Sexualfunctionevaluation
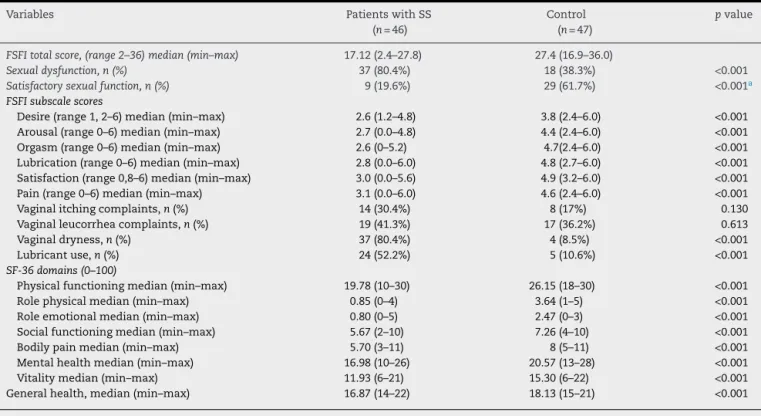
ThemediantotalscoreofFSFIwas17.12(2.4–27.8)intheSS group and 27.4 (16.9–36.0) inthe control group which was significantly lower in the SS group (p<0.001) (Table 2). In the SS group,37 (80.4%)ofpatientswere sexually dissatis-fiedand9(19.6%)weresatisfiedand,inthecontrolgroup18 (38.3%)ofpatientswere sexuallydissatisfiedand29(61.7%) weresatisfiedwithsexualfunctions(p<0.001).Moreover,all FSFIsubscores(desire,arousal,orgasm,lubrication satisfac-tionandpain)incontrolgroupweresignificantlyhigherthan thesubscoresofpatientswithSS(p<0.001).Vaginalitching waspresent in14(35%)patients,andvaginalleucorrheaor infectiouscomplaintswerepresentin19(45%)patientsinSS patients.Therewerenostatisticallysignificantdifferencein thefrequenciesofvaginalleucorrheaorinfectiouscomplaints betweenSSpatientsandcontrols(p=0.613).
Table2–Sexualfunction,vaginalcomplaintsandlifequalityofthepatientswithSjögrenSyndromeandhealthycontrols.
Variables PatientswithSS
(n=46)
Control (n=47)
pvalue
FSFItotalscore,(range2–36)median(min–max) 17.12(2.4–27.8) 27.4(16.9–36.0)
Sexualdysfunction,n(%) 37(80.4%) 18(38.3%) <0.001 Satisfactorysexualfunction,n(%) 9(19.6%) 29(61.7%) <0.001a FSFIsubscalescores
Desire(range1,2–6)median(min–max) 2.6(1.2–4.8) 3.8(2.4–6.0) <0.001
Arousal(range0–6)median(min–max) 2.7(0.0–4.8) 4.4(2.4–6.0) <0.001
Orgasm(range0–6)median(min–max) 2.6(0–5.2) 4.7(2.4–6.0) <0.001
Lubrication(range0–6)median(min–max) 2.8(0.0–6.0) 4.8(2.7–6.0) <0.001
Satisfaction(range0,8–6)median(min–max) 3.0(0.0–5.6) 4.9(3.2–6.0) <0.001
Pain(range0–6)median(min–max) 3.1(0.0–6.0) 4.6(2.4–6.0) <0.001
Vaginalitchingcomplaints,n(%) 14(30.4%) 8(17%) 0.130
Vaginalleucorrheacomplaints,n(%) 19(41.3%) 17(36.2%) 0.613
Vaginaldryness,n(%) 37(80.4%) 4(8.5%) <0.001
Lubricantuse,n(%) 24(52.2%) 5(10.6%) <0.001
SF-36domains(0–100)
Physicalfunctioningmedian(min–max) 19.78(10–30) 26.15(18–30) <0.001
Rolephysicalmedian(min–max) 0.85(0–4) 3.64(1–5) <0.001
Roleemotionalmedian(min–max) 0.80(0–5) 2.47(0–3) <0.001
Socialfunctioningmedian(min–max) 5.67(2–10) 7.26(4–10) <0.001
Bodilypainmedian(min–max) 5.70(3–11) 8(5–11) <0.001
Mentalhealthmedian(min–max) 16.98(10–26) 20.57(13–28) <0.001
Vitalitymedian(min–max) 11.93(6–21) 15.30(6–22) <0.001
Generalhealth,median(min–max) 16.87(14–22) 18.13(15–21) <0.001
a Chi-squaretest.
inflammatoryandof30(63.8%)werenormal.Morethanhalfof thepatients(n=24,52.2%)inSSreporteduseoflubricantsdue tovaginaldrynessbeforesexualintercourseinthedetailed questioningon medications.Vaginal drynessand lubricant useweresignificantlyincreasedinpatientswithSScompared tocontrols(p<0.001). Patientswho usedlubricants experi-encedthatsexualsatisfactionwasimprovedwithlubricant use,buttherestofthemwereunawareofthelubricants.Of thepatientswho usedlubricants,9(37.5%)hadsatisfactory sexualscores,howevernoneofthewomenwhodidnotuse thelubricantshadsatisfactoryFSFIscores.
Qualityoflifeassessment
Alllifequalityscores–physical,emotionalandsocial func-tions,bodilypain,generalhealth,vitality,mentalaspectand functionalcapacity–weresignificantlylowerinpatientswith SSthanthelifescoresofthecontrolpatients(Table2).
Parametersrelatedtosexualdysfunction
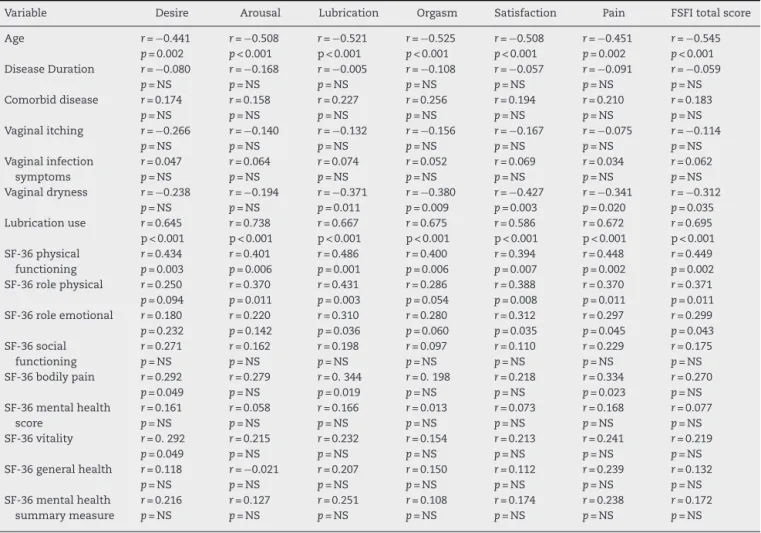
AgewasnegativelycorrelatedwithtotalFSFIscore(r=−0.545,
p<0.001)andsubscoresinpatientswithSS.Vaginal itching andinfectioussymptomswereunrelatedtototalFSFIscore andsubscores.Vaginaldrynesswasnegativelycorrelatedwith totalFSFI (r=−0.312, p=0.035)and subscores exceptdesire andarousal (Table3).Lubricationuse was positively corre-latedwithtotalFSFIscores(r=0.695,p<0.001),desire(r=0.645,
p<0.001), arousal (r=0.738, p<0.001), lubrication (r=0.667,
p<0.001), orgasm (r=0.675, p<0.001), satisfaction (r=0.586,
p<0.001)and painscores(r=0.672,p<0.001).Physical func-tioning,rolephysicalandroleemotionalscoreswerepositively
correlatedwithtotalFSFIscores(r=0.449,p=0.002;r=0.371,
p=0.011;r=0.299,p=0.043)(Table3).
Whenpatientswereaskedaboutwhetherornotthey dis-cussed their vaginalsymptomsor sexual dysfunctionwith their rheumatologists,26 (56.5%)womentoldthattheydid nottalkaboutsexualdysfunctionwiththeirrheumatologists because they did not think sexual dysfunction was being assessed.Only8(17.3%)mentionedabouttheirvaginal symp-tomstotheirphysicians.Therest12(26.2%)triedtotalkabout theirvaginaldrynessbuttheywereashamedtotalk.
Discussion
WomenwithSSoftenexperience vaginaldrynessand dys-pareuniawhichcanleadtosexualdysfunction.8Wefoundthat
patientswithSShadlowersexualfunctionscorescompared toage- matchedcontrolsand 80.4%ofthem weresexually dissatisfiedaccordingtopreviouslydeterminedcut-offvalues (FSFIscoreof<26).19,20Alldomainsofsexualfunction,
Table3–Relationshipbetweensexualdysfunction,patientcharacteristicsandpatients’clinicalpropertiesinstudygroup (patientswithSjögren’sSyndrome).
Variable Desire Arousal Lubrication Orgasm Satisfaction Pain FSFItotalscore
Age r=−0.441
p=0.002
r=−0.508 p<0.001
r=−0.521 p<0.001
r=−0.525 p<0.001
r=−0.508 p<0.001
r=−0.451 p=0.002
r=−0.545 p<0.001 DiseaseDuration r=−0.080
p=NS
r=−0.168 p=NS
r=−0.005 p=NS
r=−0.108 p=NS
r=−0.057 p=NS
r=−0.091 p=NS
r=−0.059 p=NS Comorbiddisease r=0.174
p=NS
r=0.158 p=NS
r=0.227 p=NS
r=0.256 p=NS
r=0.194 p=NS
r=0.210 p=NS
r=0.183 p=NS Vaginalitching r=−0.266
p=NS
r=−0.140 p=NS
r=−0.132 p=NS
r=−0.156 p=NS
r=−0.167 p=NS
r=−0.075 p=NS
r=−0.114 p=NS Vaginalinfection
symptoms
r=0.047 p=NS
r=0.064 p=NS
r=0.074 p=NS
r=0.052 p=NS
r=0.069 p=NS
r=0.034 p=NS
r=0.062 p=NS Vaginaldryness r=−0.238
p=NS
r=−0.194 p=NS
r=−0.371 p=0.011
r=−0.380 p=0.009
r=−0.427 p=0.003
r=−0.341 p=0.020
r=−0.312 p=0.035 Lubricationuse r=0.645
p<0.001
r=0.738 p<0.001
r=0.667 p<0.001
r=0.675 p<0.001
r=0.586 p<0.001
r=0.672 p<0.001
r=0.695 p<0.001 SF-36physical
functioning
r=0.434 p=0.003
r=0.401 p=0.006
r=0.486 p=0.001
r=0.400 p=0.006
r=0.394 p=0.007
r=0.448 p=0.002
r=0.449 p=0.002 SF-36rolephysical r=0.250
p=0.094
r=0.370 p=0.011
r=0.431 p=0.003
r=0.286 p=0.054
r=0.388 p=0.008
r=0.370 p=0.011
r=0.371 p=0.011 SF-36roleemotional r=0.180
p=0.232
r=0.220 p=0.142
r=0.310 p=0.036
r=0.280 p=0.060
r=0.312 p=0.035
r=0.297 p=0.045
r=0.299 p=0.043 SF-36social
functioning
r=0.271 p=NS
r=0.162 p=NS
r=0.198 p=NS
r=0.097 p=NS
r=0.110 p=NS
r=0.229 p=NS
r=0.175 p=NS SF-36bodilypain r=0.292
p=0.049
r=0.279 p=NS
r=0.344 p=0.019
r=0.198 p=NS
r=0.218 p=NS
r=0.334 p=0.023
r=0.270 p=NS SF-36mentalhealth
score
r=0.161 p=NS
r=0.058 p=NS
r=0.166 p=NS
r=0.013 p=NS
r=0.073 p=NS
r=0.168 p=NS
r=0.077 p=NS SF-36vitality r=0.292
p=0.049
r=0.215 p=NS
r=0.232 p=NS
r=0.154 p=NS
r=0.213 p=NS
r=0.241 p=NS
r=0.219 p=NS SF-36generalhealth r=0.118
p=NS
r=−0.021 p=NS
r=0.207 p=NS
r=0.150 p=NS
r=0.112 p=NS
r=0.239 p=NS
r=0.132 p=NS SF-36mentalhealth
summarymeasure
r=0.216 p=NS
r=0.127 p=NS
r=0.251 p=NS
r=0.108 p=NS
r=0.174 p=NS
r=0.238 p=NS
r=0.172 p=NS
FSFI:FemaleSexualFunctionIndex;NS,non-significant;r:correlationcoefficient.
AgewasnegativelycorrelatedwithsexualfunctioninSS group,whichwassimilarwiththepreviousstudies.13,21
Any-fantietal.evaluated557patientswithrheumatologicdisease andfoundthatolderagewasthe onlypredictive factorfor sexualdysfunction.21Theyreportedthatagecouldalsoaffect
physicalandpsychologicalattitudes,inturncausingsexual dysfunction.21 Even if the age affects negatively onsexual
functions in our study, SS patients had lower FSFI scores andmoresexualdysfunctioncomparinghealthyage-matched controlswhichshowsSShasprominentnegativeimpacton sexualfunctionsafteradjustingage.
Infectiousvaginalcomplaints,leucorrheaanditchingwere notcorrelatedwithsexualfunctioninourstudy,inagreement withvanNimwegenetal.13Therewerenodifferencebetween
leucorrheaanditchingsymptomsbetweenstudyandcontrol group.Evenifratesofinflammatorychangesandatrophyin vaginalsmearswerehigherinSSpatients,theywerenot sta-tisticallysignificant.
Vaginal dryness was present almost ten times more in SSpatientsthan thecontrols.Likewise,lubricantuseinSS patientswas5timesmore.Lubricantsarerecommendedby theInternationalMenopauseSocietyandtheNorthAmerican MenopauseSocietyinthepostmenopausalperiod.22,23Inthis
studyweshowedthatSSwomenmayneedlubricantsalsoin theperimenopausalperiodduetovaginaldryness.Patients
whousedlubricantsexperiencedthatsexualsatisfactionwas improvedwithlubricantuse,soitcanbeadvisedtoSSpatients bytheirphysicianeveniftheyarepremenopausal.Moreover inourstudywomenwhoreportedmorevaginalmoisturethan otherparticipantshadlesssexualpainandbettersexualpain scores(r=−0.341,p=0.020,Table3).Jozkowskietal.assessed women’s’ perceptionsabout lubricants and why they were moreinclinedtousethem.Theirfindingsshowedthatfemale preferredlubricantstofeelmorewetduringintercourse.They concludedthatlubricantuserecommendationsfromhealth professionalsandsexeducatorscouldbehelpful.24
Comorbidrheumatologicdiseasewasfoundin27.3%ofour studygroup.However,thepresenceofRAorSLEwithSSwas notcorrelatedwithsexualdysfunctioninourstudy.Anyfanti et al. evaluatedcardiovascular riskfactors ascreating sex-ualdysfunctioninpatientswithrheumatologicdisease;they reportedthattraditionalcardiovascularriskfactorsfailedto explaintheincreasedprevalenceofsexualdysfunction.21Our
samplesizeisrelativelysmallbutweincludedcomparatively young, premenopausal women in our study. We excluded womenwithseveresystemicdiseasesandcomplications,and patientswhowereusingantidepressantsordiureticsto elim-inatetheunfavorableeffectofthemonthesexualfunction.
countries.OurFSFIscoresbothinSSpatients[17.12(2.4–27.89)] andcontrolgroup[27.4(16.9–36.0)]werelowerthanprevious studies,9,12,16whichmaybeexplainedbyculturaldifferences.
VanNimwegenetal.reportedmedianFSFIscoreof20.6inthe SSpatientsand30.3inthecontrols.13Priorietal.reporteda
meanFSFIscoreof19.1±7.33intheSSpatients.Priorietal, alsosuggestedthatbothpremenopausalandpostmenopausal women with SS have worse sexual quality of life which issimilar to finding ofour study.16 Ferreira et al.reported
theprevalenceofsexualdysfunctionas18.4%in rheumato-logicpatientswiththemeanageof40.4years.Patientswith fibromyalgiaandSShadthehighestsexualdysfunction(33%) whichwaslowerthanourfindingofsexualdysfunctionrate of80.4% inSS patients in the similar age group.12 Sexual
attitudescanvaryamongculturesforsocialand psychoso-cialissues,sofunctionscoresvaryaccordingly.9,15,16Thisis
thefirststudyperformedinTurkeyonsexualfunctionofSS patients.Sexualdysfunctionincidenceofhealthywomenwas foundas28.6–48.3%instudiesperformedindifferentcities ofTurkey.25,26Inourstudysexualdysfunctionratewas38.3%
inthecontrolgroupwhichwascompatiblewiththeprevious reports.
Oneoftheaimsofourstudywastoassesslifequalityand itseffectsonsexualfunctioninpatientswithSS.Wefound thatphysicalfunction scoresinlifequality testspositively correlatedwithsexualfunctionscores.Ifapatienthasa bet-terphysicalfunctionandlessphysicalrestriction,shetends tohavemoresatisfaction.Socialfunctioningwasnotlinked tosexualfunction.Mentaldomainscores,whenthemental healthscore and emotionalscore were summed, were not correlatedwithFSFIscores(Table3).Psychologicalaspectsof sexualfunctionwereevaluatedinpreviousstudies.Anyfanti etal.statedthatinrheumatologicpatients,mentaldistress andsexualdysfunctionareextremelycommon.20Researchers
concludedthatdepressionandanxietywererelatedtosexual dysfunctioninrheumatologicdisease,aswellasinpatients with SS13,27; van Nimwegen et al. reported depression as
beingthemostimportantpredictorofsexualdysfunctionin patientswithSS.13 Wefounddecreasedroleemotionaland
mentalhealthscoresinSSpatientswhencomparedto con-trolssimilartootherstudiesintheSSpopulation.13,20Inthis
study we onlyevaluated psychologicalcharacteristics with onlythesubscalesoftheSF-36questionnaire(roleemotional andmentalhealth)whichcouldnotbesufficientfordetailed evaluation.Wedidnotevaluateddepressionoranxietywith morespecificquestionnaires,whichmaybethelimitationof ourstudy.Evenifemotionaldysfunctionwerelinkedto sex-ualdysfunction inourstudy,wecould notfindcorrelation betweenmentalhealthscoresandFSFIscores.
Inaddition, weaskedwomeniftheyhaddiscussed sex-ual activities or problems with their rheumatologists. We found out that only eight (17.3%) of them talked about vaginal complaints. Women rarely talk about these topics withtheirphysicians,asthe medicalfield tendstoneglect sexualdysfunctioninrheumatologicdisease.ManyTurkish women are also hesitant to discuss sexual problems. We talkedwithpatientsinperson.Wefeltsometimesthatthey mightbeembarrassedtoanswer questions aboutsexuality duetosocialpressure.Vaginaldrynessisoneofthe symp-tomsofSS,so rheumatologistsshouldbringup anyissues
regardingtheirpatients’intimaterelationships.Womencould then be referred togynecologists or sexologists. Psychoso-cialsupportmay begiventowomen andtheir partnersto improvetheirrelationship,asdisabilitiesincommunication andinterrelationmayincreasesexualdysfunctionand phys-ical complaints. On the other hand,for women who have decreased performanceinsexuality duetovaginaldryness or other vaginalsymptoms, lubricants orestrogens canbe recommended.
Inconclusion,womenwithSSexperiencedlowsatisfaction withsexualactivity,whichcouldbeaffectedbyage,increased vaginaldrynessandimpairedphysicalandemotional func-tion duetothe disease.Lubricantuse wasassociatedwith better sexual satisfaction and increase in FSFI total and subscores. Therefore, lubricants should beconsidered as a symptomatictreatmentinSS.Thisstudyemphasizes com-monSSsymptoms,whichhavetypicallybeenunderestimated byrheumatologists.Furthertrialswithlargerstudygroupsare necessaryforthesupportofourresults.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Weallthanktoparticipantswhoagreedtocompletethe ques-tionnaires.Nofoundationwastakenfromanycompany.
r
e
f
e
r
e
n
c
e
s
1.KassanSS,MoutsopoulosHM.Clinicalmanifestationsand
earlydiagnosisofSjögrensyndrome.ArchInternMed.
2004;164:1275–84.
2.Ramos-CasalsM,TzioufasAG,FontJ.PrimarySjögren’s
syndrome:newclinicalandtherapeuticconcepts.Ann
RheumDis.2005;64:347–54.
3.KabasakalY,KitapciogluG,TurkT,OderG,DurusoyR,MeteN,
etal.TheprevalanceofSjögren’ssyndromeinadultwomen.
ScandJRheumatol.2006;35:379–83.
4.SerorR,TheanderE,BootsmaH,BowmanSJ,TzioufasA,
GottenbergJE,etal.OutcomemeasuresforprimarySjögren’s
syndrome:acomprehensivereview.JAutoimmun.
2014;51:51–6.
5.ValimV,ZandonadeE,PereiraAM,deBritoFilhoOH,Serrano
EV,MussoC,etal.PrimarySjögren’ssyndromeprevalencein
amajormetropolitanareainBrazil.RevBrasReumatol.
2013;53:24–34.
6.GøranssonLG,HaldorsenK,BrunJG,HarboeE,JonssonMV,
SkarsteinK,etal.Thepointprevalenceofclinicallyrelevant
primarySjögren’ssyndromeintwoNorwegiancounties.
ScandJRheumatol.2011;40:221–4.
7.QinB,WangJ,YangZ,YangM,MaN,HuangF,etal.
EpidemiologyofprimarySjögren’ssyndrome:asystematic
reviewandmeta-analysis.AnnRheumDis.2015;74:1983–9.
8.FoxRI.Sjögren’ssyndrome.Lancet.2005;366:321–31.
9.MulherinDM,SheeranTP,KumararatneDS,SpeculandB,
LuesleyD,SitunayakeRD.Sjögren’ssyndromeinwomen
presentingwithchronicdyspareunia.BrJObstetGynaecol.
1997;104:101923.
10.BelenguerR,Ramos-CasalsM,Brito-ZerónP,delPinoJ,Sentís
parametersonthehealth-relatedqualityoflifeofpatients
withprimarySjögren’ssyndrome.ClinExpRheumatol.
2005;23:3516.
11.StephensonKR,MestonCM.Theconditionalimportanceof
sex:exploringtheassociationbetweensexualwellbeingand
lifesatisfaction.JSexMaritalTher.2015;41:2538.
12.FerreiraCdeC,daMotaLM,OliveiraAC,deCarvalhoJF,Lima
RA,SimaanCK,etal.Frequencyofsexualdysfunctionin
womenwithrheumaticdiseases.RevBrasReumatol.
2013;53:3546.
13.vanNimwegenJF,ArendsS,vanZuidenGS,VissinkA,Kroese
FG,BootsmaH.TheimpactofprimarySjögren’ssyndromeon
femalesexualfunction.Rheumatology(Oxford).
2015;54:1286–93.
14.ØstensenM.Newinsightsintosexualfunctioningand
fertilityinrheumaticdiseases.BestPractResClinRheumatol.
2004;18:219–32.
15.TristanoAG.Theimpactofrheumaticdiseasesonsexual
function.RheumatolInt.2009;29:853–60.
16.PrioriR,MinnitiA,DermeM,AntonazzoB,BrancatisanoF,
GhiriniS,etal.Qualityofsexuallifeinwomenwithprimary
SjögrenSyndrome.JRheumatol.2015;42:1427–31.
17.ShiboskiSC,ShiboskiCH,CriswellL,BaerA,ChallacombeS,
LanfranchiH,etal.AmericanCollegeofRheumatology
classificationcriteriaforSjögren’ssyndrome:adata-driven,
expertconsensusapproachintheSjögren’sInternational
CollaborativeClinicalAlliancecohort.ArthritisCareRes
(Hoboken).2012;64:475–87.
18.RosenR,BrownC,HeimanJ,LeiblumS,MestonC,ShabsighR,
etal.TheFemaleSexualFunctionIndex(FSFI):a
multidimensionalself-reportinstrumentfortheassessment
offemalesexualfunction.JSexMaritalTher.2000;26:191–208.
19.OksuzE,MalhanS.Kadincinselfonksiyonindeksi:Türkc¸e
uyarlamasiningec¸erlilikvegüvenilirlikanalizi.Sendrom.
2005;17:54–60.
20.AnyfantiP,PyrpasopoulouA,TriantafyllouA,TriantafyllouG,
GavriilakiE,ChatzimichailidouS,etal.Associationbetween
mentalhealthdisordersandsexualdysfunctioninpatients
sufferingfromrheumaticdiseases.JSexMed.
2014;11:2653–60.
21.AnyfantiP,PyrpasopoulouA,TriantafyllouA,DoumasM,
GavriilakiE,TriantafyllouG,etal.Theimpactoffrequently
encounteredcardiovascularriskfactorsonsexual
dysfunctioninrheumaticdisorders.Andrology.2013;1:
556–62.
22.2013positionstatementofTheNorthAmericanMenopause
SocietyManagementofsymptomaticvulvovaginalatrophy.
Menopause.2013;20:888–902,quiz903–4.
23.SturdeeDW,PanayN,InternationalMenopauseSociety
WritingGroup.Recommendationsforthemanagementof
postmenopausalvaginalatrophy.Climacteric.2010;13:509–22.
24.JozkowskiKN,HerbenickD,SchickV,ReeceM,SandersSA,
FortenberryJD.Women’sperceptionsaboutlubricantuseand
vaginalwetnessduringsexualactivities.JSexMed.
2013;10:484–92.
25.ÖksüzE,MalhanS.Prevalenceandriskfactorsforfemale
sexualdysfunctioninTurkishwomen.JUrol.2006;175:654–8,
discussion658.
26.DemirÖ,ParlakayN,GökG,EsenAA.Sexualdysfunctionina
femalehospitalstaff.Andrology.2007;33:156–60.
27.MaddaliBongiS,DelRossoA,OrlandiM,Matucci-CerinicM.
Gynaecologicalsymptomsandsexualdisabilityinwomen
withprimarySjögren’sSyndromeandsiccasyndrome.Clin