www.jped.com.br
ORIGINAL
ARTICLE
Quality
of
life,
school
backpack
weight,
and
nonspecific
low
back
pain
in
children
and
adolescents
夽
Rosangela
B.
Macedo
a,
Manuel
J.
Coelho-e-Silva
a,
Nuno
F.
Sousa
b,
João
Valente-dos-Santos
a,c,
Aristides
M.
Machado-Rodrigues
a,
Sean
P.
Cumming
d,
Alessandra
V.
Lima
e,
Rui
S.
Gonc
¸alves
f,
Raul
A.
Martins
a,∗aUniversidadedeCoimbra,Coimbra,Portugal
bUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
cUniversidadeLusófonadeHumanidadeseTecnologias,Lisboa,Portugal dUniversityofBath,Bath,UnitedKingdom
eUniversidadeFederaldoAcre(UFAC),RioBranco,AC,Brazil fInstitutoPolitécnicodeCoimbra,Coimbra,Portugal
Received7February2014;accepted6August2014 Availableonline7February2015
KEYWORDS
Qualityoflife; Nonspecificlowback pain;
Childrenand adolescents; Schoolbackpack
Abstract
Objectives: Todescribethedegreeofdisability,anthropometricvariables,qualityoflife(QoL),
andschoolbackpackweightinboysandgirlsaged11-17years.ThedifferencesinQoLbetween
thosewhodidordidnotreportlowbackpain(LBP)werealsoanalyzed.
Methods: Eighty-sixgirls(13.9±1.9yearsofage)and63boys(13.7±1.7yearsofage)
par-ticipated.LBPwasassessedbyquestionnaire,anddisabilityusingtheRoland-MorrisDisability
Questionnaire.QoLwasassessedbythePediatricQualityofLifeInventory(PedsQL).Multivariate
analysesofvarianceandcovariancewereusedtoassessdifferencesbetweengroups.
Results: Girlsreported higherdisabilitythanboys (p=0.01), andlowerQoLinthe domains
ofphysical(p<0.001)andemotionalfunctioning(p<0.01),psychosocialhealth(p=0.02)and
physical healthsummary score (p<0.001), andonthe total PedsQLscore(p<0.01). School
backpackweight wassimilarinbothgenders(p=0.61)andinparticipantswithandwithout
LBP(p=0.15).Afteradjustments,participantswith LBPreportedlowerphysicalfunctioning
(p<0.01),influencinglowerphysicalhealthsummaryscore(p<0.01).
夽
Pleasecitethisarticleas:MacedoRB,Coelho-e-SilvaMJ,SousaNF,Valente-dos-SantosJ,Machado-RodriguesAM,CummingSP,etal. Qualityoflife,schoolbackpackweight,andnonspecificlowbackpaininchildrenandadolescents.JPediatr(RioJ).2015;91:263---9.
∗Correspondingauthor.
E-mail:[email protected](R.A.Martins).
http://dx.doi.org/10.1016/j.jped.2014.08.011
264 MacedoRBetal.
Conclusions: GirlshadhigherdisabilityandlowerQoLthanboysinthedomainsofphysicaland
emotionalfunctioning,psychosocialhealth,andphysicalhealthsummaryscores,andonthe
totalPedsQLscore;however,similarschoolbackpackweightwasreported.Participantswith
LBPrevealedlowerphysicalfunctioningandphysicalhealthsummaryscore,yethadsimilar
schoolbackpackweighttothosewithoutLBP.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Qualidadedevida; Lombalgianão específica; Crianc¸ase adolescentes; Mochilaescolar
Qualidadedevida,pesodasmochilasescolareselombalgianãoespecíficaem crianc¸aseadolescentes
Resumo
Objetivos: Descrever ograu deincapacidade,variáveis antropométricas, qualidadedevida
(QV)epesodasmochilasescolaresemmeninosemeninascom11-17anosdeidade.Também
sãoanalisadasasdiferenc¸asnaQVentreosquerelataramounãolombalgia(LBP).
Métodos: 86 meninas (13,9±1,9 anos) e 63 meninos(13,7±1,7 anos) participaram.A LBP
foiavaliadaporumquestionárioeaincapacidadepeloQuestionárioRoland-Morris.AQVfoi
avaliadapeloQuestionárioPediátricosobreQualidadedeVida(PedsQL).Asanálisesdevariância
edecovariânciamultivariadasforamusadasparaavaliarasdiferenc¸asentreosgrupos.
Resultados: Asmeninasrelatarammaiorincapacidadequeosmeninos(p=0,01)emenorQVnos
domíniosdefuncionamentofísico(p<0,001)eemocional(p<0,01),noescoresumáriodesaúde
psicossocial(p=0,02)esaúdefísica(p<0,001)enoescoretotalnoPedsQL(p<0,01).Opesodas
mochilasescolareserasemelhanteparaambosossexos(p=0,61)eparaosparticipantescom
esemLBP(p=0,15).Apósajustes,osparticipantescomLBPrelatarammenorfuncionamento
físico(p<0,01),influenciandoummenorescoresumáriodesaúdefísica(p<0,01).
Conclusões: AsmeninastiverammaiorincapacidadeemenorQVqueosmeninosnosdomínios
defuncionamentofísicoeemocional,nosescoressumáriosdesaúdepsicossocialefísicaeno
escoretotalnoPedsQL;contudo,foirelatadoumpesosemelhantedasmochilasescolares.Os
participantescomLBPrevelarammenorfuncionamentofísicoeescoresumáriodesaúdefísica,
mesmocarregandomochilasescolaresdemesmopesoqueaquelessemLBP.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
Qualityoflife(QoL)takesintoaccountsubjective interpre-tationsandtheprocessin whicheachindividualcompares his current life with some identified criteria.1 Studies
investigating gender differences in QoL have produced
some equivocal results, with some reporting lower QoL2
infemales,whileothershavenotobservedanydifference
betweenmalesandfemales.3Accordingly,theeffectof
gen-deruponQoLremainsunclear.Thissubjectiveconceptcould
alsobe influencedby several health conditions, including
nonspecific low back pain (LBP).3 Among adults, LBP is a
commonsymptom,with7%to80%ofthepopulation
expe-riencingat leastoneepisodeintheir lifetime,and80% to
85%ofcasesareconsideredasnonspecificLBP.4Inchildren
andadolescents,theprevalenceofLBPisquitesimilarwith
thatobservedinadults.5Thus,theprevalenceofLBPin
chil-drenandadolescentsremainshigh,varyingbetween30-70%,
dependingonthepaindefinition,populationage,andtype
ofresearchdesignofthestudy.6
Health professionals and parents have highlighted the
regularwearingof backpacks,for the purposeof carrying
schoolmaterialsandsupplies,asapotentialriskfactorfor
LBPin children and adolescents.7 Despitethe absence of
reference-values for the weight of school backpacks, the
increasedloadisseenasanimportantfactorfavoringback
pain,8andmostresearchersandhealthpractitionersagree
withalimitfortheweightofabackpackwhichshouldnot
exceed 10% of the student’s body mass, and the weight
shouldbeequallydistributedacrossbothshoulders.8
Over 10% to 40% of adolescents have reported that
theirdailyactivitiesarebeingsomewhatlimitedbyLBP.9,10
Further research has revealed that LBP experienced in
childhood is associated with chronic LBP in adulthood.8
However,few studieshave specificallyusedvalidated and
standardizedinstrumentstoexaminetheLBPandits
poten-tial effect on QoL.11 Similarly, the overall health status
of adolescentswho usually report LBP is unknown and it
seemstobedifficulttodefinetheboundariesofanunique
experience,or the painasa health problem.7 The use of
standardizedQoLinstrumentsmaydisclosethehealthstatus
amongdifferent generalpopulations, individuals suffering
pain,andsubgroupsof childrenandadolescentsreporting
LBP.
Inthecontextofthesetrends,thepresentstudyaimed
todescribethedegree ofdisability,anthropometric
varia-bles,QoL,andschoolbackpackweightinboysandgirlsaged
differencesin QoLbetween children andadolescentswho
didordidnotreportLBP.
Methods
Studydesignandparticipants
The study had a cross-sectional design. The sample was recruitedfrom12classesintwoschoolsof thecityof Rio Branco,Brazil;a totalof324 studentswereinitially eligi-ble toparticipatein this study.However, only a groupof 149(86 femalesand63 males;age11-17 years)remained andagreedtotakepartintheinvestigation,after consider-ingtheinclusioncriterionasa‘yes’answertothefollowing question: ‘‘Duringthe last year,did youfeel anyepisode ofdiscomfortinthelowback,extendingtothelegs?’’.The exclusioncriteriacomprisedidiopathicscoliosis,spondylitis, andherniaofintervertebraldiscus.
All participants agreed to take part of this study and theirparents/guardiansprovidedwritteninformedconsent, consistent with the Declaration of Helsinki. All methods andproceduresofthisinvestigationwereapprovedbythe InstitutionalScientific Boardof theUniversityof Coimbra, Portugal.Clinicaldatawererecordedusingstructured ques-tionnaires, which were administered by trained research assistants.
Aftertherecruitmentperiod,participantswereinvited toapreliminarymeetinginwhichtheywereinformedabout thenature,benefits,andrisksof thestudy.Inthesecond part of this meeting, participants completed the Roland-Morris Disability Questionnaire (RMDQ), and the Pediatric Quality of LifeInventory(PedsQL). Asecond meeting was thenscheduledfortheassessmentofanthropometric varia-bles.Theweightofeachparticipant’sschoolbackpackwas measuredonthreeseparatedayswithinaweekandthena meanvalueacrossallthreedayswascalculated.
LBP
ThepresenceofLBPinthepastmonthwasevaluatedwith thefollowingdirectquestionatthetimeoftheassessment: ‘‘Inthepastmonth,haveyouhadlowbackpainwhichlasted foronedayorlonger?’’.Incaseofapositiveresponse, par-ticipantswereinstructedtoindicatethesiteofpainusinga picture.11Participantswerealsoaskedtocompleteaversion
oftheRMDQwhichhadbeenadaptedandvalidated
specifi-callyfortheBrazilianpopulationbySardáJúnioretal.12The
RMDQisasimpleinstrumentconsistingof24questionswith
dichotomous responses (yes/no)and measures thedegree
ofdisabilityexperiencedbytheparticipant.Thefinalscore
ontheRMDQrepresentsthesumofpositiveanswers,with0
correspondingtoapersonwithoutanycomplaints,while24
correspondstoapersonwithveryseverelimitations.
Schobertest
ParticipantswerealsoaskedtocompletetheSchobertest, whichisusedtomeasurethemobilityofthelumbarspine, and was first described by Schober.13 The test is carried
out in standing position and in maximum forward trunk
flexion,keepingthekneesextended.Withtheparticipantin
theorthostaticposition,parallelhorizontallinesaredrawn
10cmaboveand5cmbelowthelumbosacraljunction.The
testwasconsiderednormalwhentherewasvariationofat
least5cmbetweenthemeasuresinorthostaticpositionand
trunkflexion.
Health-relatedqualityoflife(HRQoL)
TheHRQoLwasassessedbyaversionofthePedsQL14 that
wasadaptedandvalidated fortheBrazilian populationby
Klatchoianetal.15Thisquestionnairecanbeusedtoassess
HRQoL in healthy children and adolescents, and in those
withacuteand chronic health conditions, andconsists of
23itemscomprisingfourmultidimensionalscales:i)
physi-calfunctioning(eightitems);ii)emotionalfunctioning(five
items);iii) socialfunctioning (fiveitems);iv) school
func-tioning(five items).The fourmultidimensional scales are
grouped in three summary scores: i) psychosocial health
summaryscore(15items);ii)physicalhealthsummaryscore
(eightitems);iii)totalPedsQoLscore(23items).Itemsare
reverse scored and linearly transformed to a 0-100 scale
(0=100; 1=75; 2=50; 3=25; 4=0), so that higher scores
indicatebetterHRQoL.
Anthropometricsandschoolbackpackweight
Staturewasmeasuredto0.1cm,usingastandard stadiome-ter,withthe participants in theupright position, without shoes.Bodyweightwasmeasuredbarefootinlightclothing onacalibrateddigitalbalance-beamscale(FilizolaPL200, Filizola®,São Paulo, Brazil)withprecision to thenearest 100g.Bodymass index(BMI)wasdeterminedby calculat-ingtheratioofthebodymassinkgbystatureinm2.The
anthropometricmeasurementswereconductedinseparate rooms,toensuretheparticipants’privacy.Schoolbackpack weightwasmeasuredatthreeseparateoccasionsduringthe weekwiththesamedigitalscale(FilizolaPL200,Filizola®, SãoPaulo,Brazil).
Statisticalanalysis
266 MacedoRBetal.
effects, respectively. Translated into partial eta squared, valuesof 0.01, 0.06, and 0.14 were considered as small, moderate,andlargeeffects,respectively.
Results
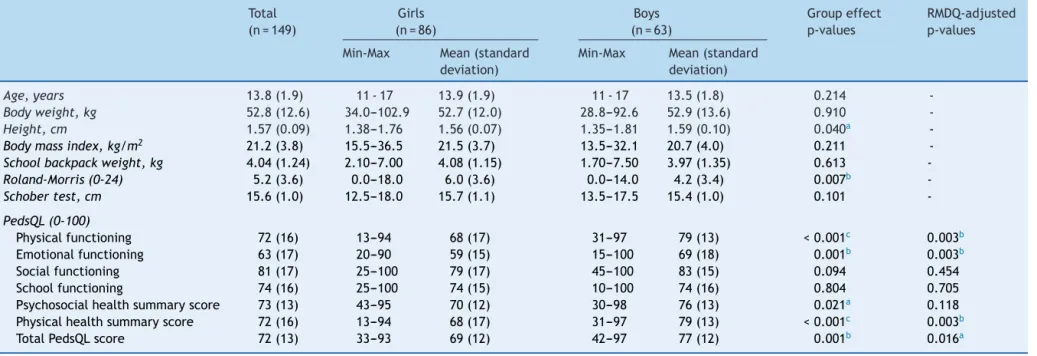
The characteristics of the participants are described in
Table 1. Both boys and girls aged between 11-17 years
reportedsimilarmeanvaluesforage(p=0.214).Mean
val-uesfor bodymass(p=0.910)andBMI(p=0.211)werealso
similarinboysandgirls,thoughboysweretallerthangirls
(1.59±0.10cmversus1.56±0.07cm).Compared toboys,
girlsreportedhigherlevelsofdisabilityasassessedbythe
RMDQ(p=0.007).GirlsalsoreportedlowerlevelsofHRQoL
thanboys,asmeasuredbythePedsQL,andalsointermsof
thedomainsof‘physicalfunctioning’(p=0.003),‘emotional
functioning’ (p=0.003), ‘physical health summary score’
(p=0.003),and‘totalPedsQLscore’(p=0.016).Theselower
scoresonHRQoLreportedbythegirlswereindependentof
degreeofdisability.
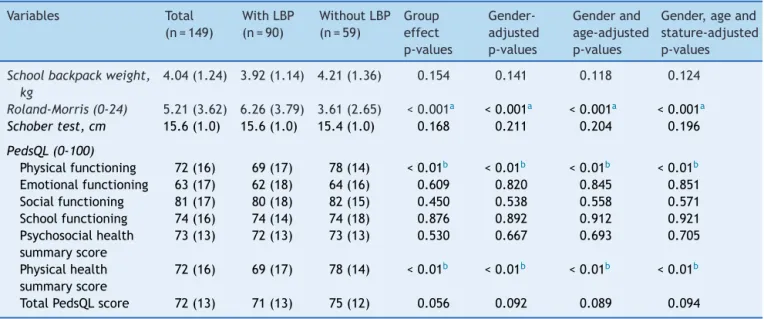
Table2highlightscomparisonsbetweenparticipantswith
LBPin thepast month (n=90; 55 girls and 35 boys),and
without LBP in the past month (n=59; 31 girls and 28
boys).ThemeanvalueforHRQoLwashigherinthose
with-outLBP(p<0.001),specificallyinthedomainsof‘physical
functioning’(p<0.01),and‘physicalhealthsummaryscore’
(p<0.01).The ‘totalPedsQLscore’ alsoshowedthesame
trendofdifferences,butwithamarginalvalue(p=0.056).
In participants with LBP, the lower HRQoL mean score is
similarafter controlling for potential confoundingeffects
ofgender,age,andstature.Nodifferenceswereobserved
betweenparticipantswithLBPandwithoutLBP,particularly
interms ofschool backpackweight, onthe Schobertest,
andinthePedsQLscalesof‘emotionalfunctioning’,‘social
functioning’,‘schoolfunctioning’,and‘psychosocialhealth
summaryscore’.
Discussion
Thisstudyaimedtodescribeandtocompare anthropomet-ricvariables,QoL,andschoolbackpackweightinboysand girlsaged11-17years,withandwithoutnon-specificLBPin thepast month. Boysweretallerthan thegirls (Table1),
whilethebodyweightandtheBMIweresimilarinbothboys
andgirls.Ofnote,differencesinstaturebetweengenders
increasefrom10yearsofage;16thisprocessisrelatedtothe
onsetofadolescence,whichhasbeenexplainedbyhormonal
influencesthataffectfemalesbeforemales.17Thepubertal
growthspurt thatoccurs laterand at greater intensity in
malesthaninfemalescontributestothehigherstatureand
bodyweightobservedinboysafterpuberty.18
The Schober test has been widely used by several
authors19 to assess the extent of lumbar flexion.
Consis-tent withprevious research,19 participants of the current
studywithLBPobtainedsimilarvaluesintheSchobertest
when compared with participants without LBP,
indepen-dently of gender, age, and stature (Table 2). However,
somestudieshavefoundincreasedmobilitytobeassociated
with decreased LBP.20 The majority of students obtained
more than 15 centimeters in the Schober test, which is
a positive performance. The lack of differences in that
test across groups could be associatedwith
methodologi-cal procedures (e.g., those assessments were conducted
duringphysical educationclasses).Consequently, students
mayhavealreadybeenengagedinactivity,and,thus,had
improvedtheirmusculartemperature19leadingto
enhance-mentsinflexibility. Infact,flexibilityhasalsobeenshown
to vary during the day, and differences in the time of
assessmentmayhaveinfluencedthecomparisonofresults
betweenstudentswithandwithoutLBPinthepresentstudy,
corroboratingresultsofpreviousstudies.21
Schoolbackpackswereregularlyusedbythemajorityof
studentswhoparticipatedinthecurrentstudy(99%);these
results areconsistent withlevels of useobserved by
oth-ersauthors.19Someauthors22havesuggestedthatincreasing
theweightoftheschoolbackpackisassociatedwithhigher
prevalenceofLBP,andtherefore,causingtemporaryor
per-manent postural maladaptation, muscle contracture, and
inflammation. Findings from the present study revealed
that128students(86%)hadatleastoneepisodeofLBPin
theirlives attributabletothedailytransportof the
back-packs, which is consistent with values reported in other
studies.9 At the moment of the evaluation, 60% of the
present participants (n=90) had reported LBP in the last
month, nevertheless all participants had experienced at
leastoneepisodeofdiscomfortinthelowbackduringthe
previousyear;however,nodifferenceswerefoundbetween
groups withand without LBP. Despite the fact that these
results are in line with some previous studies,9,23 others
have found associations between LBP and the weight of
theschoolbackpack,24particularlywhenasymmetrical
load-ingwasconsidered(carryingononlyoneshoulder), which
is associated with higher incidence of dorsal and lumbar
pain.25Infact,theabsenceofdifferencesbetween
partic-ipantswithandwithoutLBPinthepresentstudycouldbe
explained, at least in part, because only 18% of students
carry school backpacks on one shoulder, while 78% use it
bilaterally;theremaining4%of thestudentsusebagwith
wheelsandotherkindsofschoolbags.
Anothersource of variationis the timespent between
home and school, and the type of transportation. Prista
et al.26 observed thatLBP appears in home-school routes
longer than 30minutes. The majority of participants of
the present study (89%) usually travel by car between
home and school. The remaining 11% of students, who
usually go to school by walking, do it in a short time,
limitingthetimeofbearingweightontheback(34%walk
for less than15minutes;35%between 15-30minutes; 31%
over30minutes).Thiscertainly contributedtoexplainthe
lack of association between LBP and theschool backpack
weight.
Althoughthisstudydoesnotprovidesupportforbackpack
weightasriskfactorforshort-termLBP,itcouldnotexclude
itslong-termeffects.Infact,the long-termconsequences
of carrying heavy backpacks include discomfort and back
pain.27Therefore,Bauer&Freivalds28statethattheweight
ofthebackpackshouldnotexceed10%ofthebodyweight
and,therefore,couldpositivelycontributetoavoidfuture
healthproblems.Inthepresentstudy,themeanvaluesfor
backpacks weightwas4.04±1.24kg, andfor bodyweight
was52.8±12.6kg,whichfallswithinthelimits,and
proba-blyalsocontributestotheabsenceofsignificantdifferences
of
life,
school
backpack
weight,
and
nonspecific
low
back
pain
in
children
267
Table1 Participants’characteristicsanddifferencesbetweengenderscalculatedwithmultivariateanalysis,adjustedfortheRoland-MorrisDisabilityQuestionnaire(RMDQ).
Total
(n=149)
Girls
(n=86)
Boys
(n=63)
Groupeffect
p-values
RMDQ-adjusted p-values
Min-Max Mean(standard
deviation)
Min-Max Mean(standard
deviation)
Age,years 13.8(1.9) 11-17 13.9(1.9) 11-17 13.5(1.8) 0.214
-Bodyweight,kg 52.8(12.6) 34.0---102.9 52.7(12.0) 28.8---92.6 52.9(13.6) 0.910
-Height,cm 1.57(0.09) 1.38---1.76 1.56(0.07) 1.35---1.81 1.59(0.10) 0.040a
-Bodymassindex,kg/m2 21.2(3.8) 15.5---36.5 21.5(3.7) 13.5---32.1 20.7(4.0) 0.211
-Schoolbackpackweight,kg 4.04(1.24) 2.10---7.00 4.08(1.15) 1.70---7.50 3.97(1.35) 0.613
-Roland-Morris(0-24) 5.2(3.6) 0.0---18.0 6.0(3.6) 0.0---14.0 4.2(3.4) 0.007b
-Schobertest,cm 15.6(1.0) 12.5---18.0 15.7(1.1) 13.5---17.5 15.4(1.0) 0.101
-PedsQL(0-100)
Physicalfunctioning 72(16) 13---94 68(17) 31---97 79(13) <0.001c 0.003b
Emotionalfunctioning 63(17) 20---90 59(15) 15---100 69(18) 0.001b 0.003b
Socialfunctioning 81(17) 25---100 79(17) 45---100 83(15) 0.094 0.454
Schoolfunctioning 74(16) 25---100 74(15) 10---100 74(16) 0.804 0.705
Psychosocialhealthsummaryscore 73(13) 43---95 70(12) 30---98 76(13) 0.021a 0.118
Physicalhealthsummaryscore 72(16) 13---94 68(17) 31---97 79(13) <0.001c 0.003b
TotalPedsQLscore 72(13) 33---93 69(12) 42---97 77(12) 0.001b 0.016a
PedsQL,PediatricQualityofLifeInventory. a p<0.05.
b p<0.01. c p<0.001.
268 MacedoRBetal.
Table2 Multivariateanalysisbetweengroups,adjustedforgender,age,andstature.
Variables Total
(n=149)
WithLBP
(n=90)
WithoutLBP
(n=59)
Group effect p-values
Gender-adjusted p-values
Genderand
age-adjusted p-values
Gender,ageand
stature-adjusted p-values
Schoolbackpackweight, kg
4.04(1.24) 3.92(1.14) 4.21(1.36) 0.154 0.141 0.118 0.124
Roland-Morris(0-24) 5.21(3.62) 6.26(3.79) 3.61(2.65) <0.001a <0.001a <0.001a <0.001a
Schobertest,cm 15.6(1.0) 15.6(1.0) 15.4(1.0) 0.168 0.211 0.204 0.196
PedsQL(0-100)
Physicalfunctioning 72(16) 69(17) 78(14) <0.01b <0.01b <0.01b <0.01b
Emotionalfunctioning 63(17) 62(18) 64(16) 0.609 0.820 0.845 0.851
Socialfunctioning 81(17) 80(18) 82(15) 0.450 0.538 0.558 0.571
Schoolfunctioning 74(16) 74(14) 74(18) 0.876 0.892 0.912 0.921
Psychosocialhealth summaryscore
73(13) 72(13) 73(13) 0.530 0.667 0.693 0.705
Physicalhealth summaryscore
72(16) 69(17) 78(14) <0.01b <0.01b <0.01b <0.01b
TotalPedsQLscore 72(13) 71(13) 75(12) 0.056 0.092 0.089 0.094
PedsQL,PediatricQualityofLifeInventory. ap<0.001.
b p<0.01.
Significantdifferencesbetween-subjectseffects.
In the present study,girls reportedlower mean values for HRQoLthan boysin ‘physical functioning’, ‘emotional functioning’,‘psychosocialhealthsummary score’, ‘physi-calhealthsummaryscore’,and‘totalPedsQLscore’.After controlling for the degree of disability, those differences weremaintainedwithexceptionforthe‘psychosocialhealth summary score’(Table 1). The lower HRQoL exhibitedby
thegirlscouldbepartiallyexplainedthroughthedifferent
recreationalactivities; boys have more leisure time than
girls,whilefemaleadolescentsareprobablymorefocused
helpingtheir mothersin householdchores. Another
possi-bleexplanationis relatedtothe onsetof pubertyand its
associationstophysiquechanges;infact,femalesfacegreat
challenges,because,forexample,theonsetofmenstruation
causesfrequentcomplaints,previouslyobservedbyKolip.29
Furthermore,individualdifferencesinbiologicalmaturation
havebeenshowntoaccountfortheagerelateddeclinesin
HRQoLinUK adolescent females.30 The hormonal
fluctua-tionsthatoccurinteenage girlsmayfurthercontributeto
changesinpsychologicalwell-being.2
A person with symptoms of LBP is often partially and
temporarily diminished in the performance of everyday
activities,whichnegativelyimpactsQoL,andlegitimizesper
setheimportanceofquantifyingthesubsequentfunctional
disability.10 However, this is not a consensus with others
authors.11TheRMDQwasusedinthepresentstudytoassess
thedegreeoffunctionaldisability,revealing,asexpected,
higherdisabilityinthosewhoreferredLBP,independentlyof
thegender,age,andstature(Table2).Ofnote,participants
withLBPhadlower HRQoL,butonly in thedimensions of
‘physicalfunctioning’and‘physicalhealthsummaryscore’;
thesedifferencesweremaintainedaftercontrollingforthe
effectsofthegender,age,andstature.Thesefindings
high-lightthenegativeimpactoftheLBPonthephysicaldomain
oftheHRQoLinyouth.
Inthecurrentstudy,participantswithandwithout LBP
carried similar school backpack weight, which seems to
suggestthattheweightofthebackpacks,ifwithinthe
rec-ommendedvalues,isnotariskfactorforLBP.Inaddition,
findings suggest that girls have higher levelsof disability
than boys, and lower HRQoL, particularly in the domains
of physical and emotional functioning, which impacts the
totalHRQoLscore.Finally,thepresentstudysuggeststhat
participantswithLBPreportlowerperceivedHRQoL,
specif-icallyinthephysicalfunctioningdomain.Collectively,these
findingsareofimportance,especiallytoencourageparents
and teachers to be aware of risk factors associated with
LBP. Moreover, LBP tends to be of low intensity and
fre-quency,andadultsshouldbeawarethatchildrenshouldnot
beexposedtoexcessiveloadsarisingfromschoolsupplies,
tocontributetoabetterQoLduringyouth.
Inconclusion,girlsreportedhigherdisabilitylevels,and
lowerQoLin thedomainsofphysical andemotional
func-tioning,psychosocialhealthsummaryscore,physicalhealth
summary score,andin thetotalPedsQL score,comparing
withboys.Theschoolbackpackweightwassimilarinboth
genders,waswithintherecommendedvalues,andwas
unre-lated toLBP. After controlling for potential confounders,
participantswithLBPhavelowerHRQoL,specificallyinthe
domainsofphysical functioning,andlowerphysicalhealth
summaryscore.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
of Medicine, Department of Landscape Architecture and UrbanPlanning,CollegeofArchitecture3137TAMUCollege Station, Texas 77843-3137 USA, for the construction of a standardized instrument for HRQoLand permission for its useinthisstudy.
References
1.TrineMR.Physicalactivityandqualityoflife.In:RippeJM, edi-tor.Lifestylemedicine.Malden,MA:BlackwellScience;1999. p.989---97.
2.O’SullivanPB,BealesDJ,SmithAJ,StrakerLM.Lowbackpain in17yearoldshassubstantialimpactandrepresentsan impor-tantpublichealthdisorder:across-sectionalstudy.BMCPublic Health.2012;12:100.
3.Gold JI, Mahrer NE, Yee J, Palermo TM. Pain, fatigue, and health-relatedqualityoflifeinchildrenandadolescentswith chronicpain.ClinJPain.2009;25:407---12.
4.Burton AK, Balagué F, Cardon G, Eriksen HR, Henrotin Y, LahadA, et al. Chapter2. European guidelines for preven-tioninlowbackpain:November2004.EurSpineJ.2006;15: S136---68.
5.KjaerP,WedderkoppN,KorsholmL,deLeboeuf-YC.Prevalence andtrackingofbackpainfromchildhoodtoadolescence.BMC MusculoskeletDisord.2011;12:98.
6.JeffriesLJ,MilaneseSF,Grimmer-SomersKA.Epidemiologyof adolescentspinalpain:asystematicoverviewoftheresearch literature.Spine(PhilaPa1976).2007;32:2630---7.
7.Balagué F, Dudler J, Nordin M. Low-back pain in children. Lancet.2003;361:1403---4.
8.CottalordaJ1,BourelleS,GautheronV,KohlerR.Backpackand spinaldisease: myth or reality? RevChir Orthop Reparatrice ApparMot.2004;90:207---14.
9.WatsonKD,PapageorgiouAC,JonesGT,TaylorS,SymmonsDP, SilmanAJ,etal.Lowbackpaininschoolchildren:theroleof mechanicalandpsychosocialfactors.ArchDisChild.2003;88: 12---7.
10.Roth-Isigkeit A, Thyen U, Stöven H, Schwarzenberger J, Schmucker P.Pain among children and adolescents: restric-tionsindailylivingandtriggeringfactors.Pediatrics.2005;115: 152---62.
11.PelliséF,BalaguéF,RajmilL,CedraschiC,AguirreM,Fontecha CG,etal.Prevalenceoflowbackpainanditseffecton health-relatedqualityoflifeinadolescents.ArchPediatrAdolescMed. 2009;163:65---71.
12.SardáJúniorJJ,NicholasMK,PimentaCA,AsghariA,Thieme AL.Validac¸ãodoQuestionáriode IncapacidadeRolandMorris paradoremgeral.RevDor.2010;11:28---36.
13.Schober Von P.Lendenwirbelsäule und Kreuzschmerzen (The lumbarvertebralcolumnandbackache).MunchMed Wochen-schr.1937;84:336---8.
14.VarniJW,SeidM,KurtinPS.PedsQL4.0:reliabilityandvalidity ofthePediatricQuality ofLifeInventory version4.0generic
core scales in healthy and patient populations. Med Care. 2001;39:800---12.
15.KlatchoianDA,LenCA,TerreriMT,SilvaM,ItamotoC,Ciconelli RM,etal.QualityoflifeofchildrenandadolescentsfromSão Paulo:reliabilityandvalidityoftheBrazilianversionofthe Pedi-atricQualityofLifeInventoryversion4.0GenericCoreScales. JPediatr(RioJ).2008;84:308---15.
16.SilvaDA,PelegriniA,PetroskiEL,GayaAC.Comparisonbetween thegrowthofBrazilianchildrenandadolescentsandthe refer-ence growthcharts: datafrom a BrazilianProject. JPediatr (RioJ).2010;86:115---20.
17.WellsJC.Sexualdimorphism ofbodycomposition.BestPract ResClinEndocrinolMetab.2007;21:415---30.
18.Malina RM, BouchardC,Beunen G. Human growth.Selected aspectsofcurrentresearchonwell-nourishedchildrenAnnRev Anthropol.1988;17:187---219.
19.FeldmanDE, ShrierI, Rossignol M,Abenhaim L. Risk factors for thedevelopmentof lowbackpainin adolescence.AmJ Epidemiol.2001;154:30---6.
20.JonesMA,StrattonG,ReillyT,UnnithanVB.Biologicalrisk indi-catorsforrecurrentnon-specificlowbackpaininadolescents. BrJSportsMed.2005;39:137---40.
21.Adams MA. Biomechanics of back pain. Acupunct Med. 2004;22:178---88.
22.HeuscherZ, GilkeyDP,PeelJL,KennedyCA.Theassociation ofself-reported backpackuseand backpackweightwithlow backpainamongcollegestudents.JManipulativePhysiolTher. 2010;33:432---7.
23.Kaspiris A, Grivas TB, Zafiropoulou C, Vasiliadis E, Tsadira O. Nonspecific lowback painduring childhood: a retrospec-tiveepidemiologicalstudyof riskfactors.JClinRheumatol. 2010;16:55---60.
24.OzgülB,AkalanNE,KuchimovS,UygurF,TemelliY,PolatMG. Effectsofunilateralbackpackcarriageonbiomechanicsofgait in adolescents: a kinematicanalysis. ActaOrthop Traumatol Turc.2012;46:269---74.
25.KorovessisP,KoureasG,ZacharatosS,PapazisisZ.Backpacks, backpain,sagittalspinalcurvesand trunkalignment in ado-lescents: a logistic and multinomial logistic analysis. Spine (PhilaPa1976).2005;30:247---55.
26.PristaA, BalaguéF,NordinM,SkovronML.Low backpainin Mozambicanadolescents.EurSpineJ.2004;13:341---5. 27.AkdagB1,CavlakU,CimbizA,CamdevirenH.Determinationof
painintensityriskfactorsamongschoolchildrenwith nonspe-cificlowbackpain.MedSciMonit.2011;17:PH12---5.
28.BauerDH,FreivaldsA.Backpackloadlimitrecommendationfor middleschoolstudentsbasedonphysiologicaland psychophys-icalmeasurements.Work.2009;32:339---50.
29.KolipP.Genderdifferencesinhealthstatusduringadolescence: aremarkableshift.IntJAdolescMedHealth.2011;9:9---18. 30.CummingSP,GillisonFB,SherarLB.Biologicalmaturationasa