BrazJOtorhinolaryngol.2015;81(4):451---453
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
CASE
REPORT
Visual
loss:
a
rare
complication
of
maxillary
sinus
mucocele
夽
,
夽夽
Perda
visual:
complicac
¸ão
rara
de
mucocele
de
seio
maxilar
Juliana
Caminha
Simões,
Francisco
Bazílio
Nogueira-Neto,
Luciano
Lobato
Gregório,
Fábio
de
Azevedo
Caparroz,
Eduardo
Macoto
Kosugi
∗RhinologyDivision,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(EPM/UNIFESP),SãoPaulo,SP,Brazil
Received26January2015;accepted16March2015 Availableonline6June2015
Introduction
Mucoceles are cystic formations lined with respiratory epithelium that contain a mucoid or mucopurulent fluid. Although benign,mucoceles arelocally expansive,due to continuousproductionandaccumulationofmucus,resulting inerosionandunderlyingboneremodeling.Thismayaffect theorbit,skullbase,orsofttissueoftheface.Frontal, eth-moidal,andfronto-ethmoidalsinusesarethemostcommon locations,while the, maxillaryandsphenoidalsinuses are lessfrequentlyaffected.Maxillarysinusmucocelesarerare, accountingforlessthan10%ofallmucocelesintheUSAand Europe.1
Orbitalsymptomsarerelativelycommoninpatientswith mucocele,duetotheexpansionofthelesionintotheorbit.1 These symptoms are usually caused by ethmoidal, sphe-noidal, and frontal mucoceles. Ophthalmologic impact is unusualfrommaxillarymucoceles.Astoorbitalsymptoms,
夽 Pleasecitethisarticleas:SimõesJC,Nogueira-NetoFB,Gregório
LL,CaparrozFA,KosugiEM.Visualloss:ararecomplicationof max-illarysinusmucocele.BrazJOtorhinolaryngol.2015;81:451---3.
夽夽Institution: Rhinology Sector, Department of
Otorhinolaryn-gology and Headand Neck Surgery,Escola Paulistade Medicina, UniversidadeFederaldeSãoPaulo(EPM/UNIFESP),SãoPaulo,SP, Brazil.
∗Correspondingauthor.
E-mail:[email protected](E.M.Kosugi).
edemaandperiorbitalpainarethemostcommonfindings. Amaurosisisthemostfearedcomplication,butfortunately itoccurswithlowfrequency,2anditsoccurrenceinmaxillary mucocelesisextremelyrare.1---5
The objective of this study is toreport a rare case of maxillarymucoceleleadingtoamaurosis.
Case
presentation
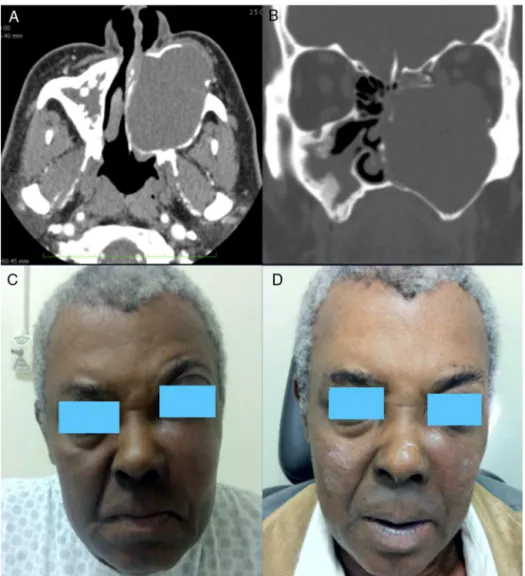
Thisreportconcernsamalepatient,67yearsofage,with proptosis and a progressive bulging in left malar region, in association with a lasting continuous ipsilateral nasal obstruction/clear rhinorrhea. In about five months, his visualacuitybegantodecrease,accompanied by progres-sive eye pain on the left side. Clinical history revealed facialtrauma 18 yearsin the past, hypertensionand dia-betes mellitus. Physical examination revealed left malar areadeformity,withpainonpalpationinassociation with ipsilateralproptosis.Nasalendoscopyshowedmedialization oftheleftlateralnasalwall,causingacompleteocclusion ofthe nasal cavity. An ophthalmologicevaluation showed decreasedleftpupillaryreflexes,visualacuity,and extraoc-ularmotility.Computedtomographyoftheparanasalsinuses showedan expansible lesioninto theleft maxillarysinus, withdensity compatiblewithsofttissue,withnocontrast enhancement,andremodelingoftheadjacentbone struc-ture,suggestiveofmaxillarymucocele(Fig.1).
Thepatientunderwentmaxillarymucocele marsupializa-tionthrough nasal endoscopyby a widemaxillary middle
http://dx.doi.org/10.1016/j.bjorl.2015.03.008
452 SimõesJCetal.
Figure1 (A)Computedtomography (CT)(axialsection),showinganexpansivelesionoccupyingtheentireleftmaxillarysinus andpromoting remodelingofbonelimits. (B)CT(coronalsection),showinganextensionofthelesiontotheorbitalcone.(C) Preoperativepictureshowingbulgingofthemalarareaandproptosis(leftside).(D)Postoperativephotographyshowingaclear improvementofbulgingandproptosis.
meatal antrostomy, resulting in a profuse draining of a yellow-citrinefluid.Intheimmediatepostoperativeperiod (IPP),thecase evolvedwithsignificant reductionof facial deformityandresolutionofvisualcomplaints.An ophthal-mologic examination in the IPP revealed full recovery of visualacuityandextrinsicocularmotility;afewdayslater the patient showed improvement of pupillary reflex. A one-yearfollow-upshowedthatthepatientremains asymp-tomatic,withamildresidualfacialasymmetryandnoother complaints.
Discussion
Amaurosisis the most serious orbital complicationof any mucocele.Thelargestpublishedseriesofcasesof mucoce-leswithorbitalinvolvementshowedanincidenceof18.8% ofamaurosis,whenonly patientswithorbitalinvolvement wereconsidered.2 Smaller serieshave demonstrated vari-ationfrom 6.7% to40% for amaurosis, always considering onlypatientswithorbitalinvolvement.2---5Whenallcasesof mucocelewereconsidered,loweroccurrenceofamaurosis hasbeenreported,approximately5%.2
Almost 30% of all mucoceles may erode toward the orbit, and the fronto-ethmoidal mucoceles are primarily responsible for this extension, followed by frontal and ethmoidal mucoceles.1 Maxillary mucoceles, in addition to being rare, seldom invade the orbit.1---5 Even in the faceof aninvasion,usuallytheonlyorbitalsymptomsare eye pain,3,5 proptosis,3 or diplopia.3 A reportof amauro-sis caused by maxillary mucocele occurred in a patient who had been subjected toskeletal surgery (Le Fort III), where this previous procedure, by fracturing the orbital floor and sinus, could have facilitated both the devel-opment of the mucocele and its extension toward the orbit.4 The patient of the present maxillary mucocele reportwasnotinvolved withprevious surgery,thus revea-ling a case of atypical development of a relatively rare disease.
Final
considerations
Visualloss:ararecomplicationofmaxillarysinusmucocele 453
loss.Earlydiagnosisfollowedbyanappropriateandprompt treatmentcanleadtoimmediaterecoveryofvision.
Conflict
of
interests
Theauthorsdeclarenoconflictofinterests.
References
1.Scangas GA, GudisDA, Kennedy DW. The natural history and clinicalcharacteristicsofparanasalsinusmucoceles:aclinical review.IntForumAllergyRhinol.2013;3:712---7.
2.KimYS,KimK,LeeJG,YoonJH,KimCH.Paranasalsinus mucoce-leswithophthalmologicmanifestations:a17-yearreviewof96 cases.AmJRhinolAllergy.2011;25:272---5.
3.Loo JL, Looi AL, Seah LL. Visual outcomes in patients with paranasal mucoceles. Ophthal Plast Reconstr Surg. 2009;25:126---9.
4.PatelPA,WarrenSM,McCarthyJG.Maxillarymucocelewith prop-tosisand visual impairment:a latecomplicationofLeFortIII distraction.JCraniofacSurg.2013;24:2000---2.