Introduction
In the last decades, the world population has undergone to huge transformations, both in its population structure and in its morbidity and mortality patterns. It has been observed a reduc-tion in the fertility rate and an increase in life expectancy due to the decline in mortality induces by improvements in health conditions and quality of life1.
Associated to the process of demographic transition there is also the process of epidemiological transition. The preva-lence of infectious-contagious diseases is replaced by more complex pathological conditions and more expensive interven-tion, such as chronic degenerative diseases, mental diseases, cardiovascular diseases and cancer, which predominantly affect the population over 65 years1. Chronic diseases lean to accelerate the process of diminishing functional capacity, which already occurs in the aging process of the organism alone1. Thus, as life expectancy rates increase, there is a tendency for functional decline, and increased functional disability in the old population2,3.
Given this situation, there is a clear indication of the need of attention for this growing number of old people, since popula-tion aging has a signiicant impact on health and in the levels of independence and autonomy of the population2,3. Therefore, the focus of government health programs is on the functional improvement and well being of the aging population, rather than just healing and survival2,3.
In this way, physical activity might function as part of the strategy in the treatment and control of non-communicable diseases and injuries, which arising intensiies with increas-ing age4. Physical activity is also essential for maintaining the functions of the locomotor system, which is highly related to the performance of daily life activities and to the degree of independence and autonomy of the old people5, and directly inluence in improvement and/or maintenance of the quality of life of this population.
Thus, the regular practice of physical activity and adherence to it for prolonged periods is a fundamental aspect to improve the quality of life and to provide independent aging6. It is emphasized that the beneits of physical activity are achieved only if the ac-tivity is performed on a regular basis. When physical acac-tivity is planned, structured, repetitive and intentional, in the sense that the improvement or maintenance of one or more components of physical itness is a goal, it is referred as physical exercise7. Thereby, the adherence to exercise plays a vital role in maximizing the beneits of physical activity8. Although the literature aims to the importance and beneits of physical exercise, researchers’ efforts do not seem to be suficient to sensitize the elderly population to participate in regular exercise. People with 65 years old or older usually do not perform enough physical exercises to promote physiological adjustment, being that 60 a 70% of older are sed-entary. As a result of the deconditioning, many older people live below of their physical capacity threshold, with risk of entering in a cycle of inactivity and functional decline that can lead to total
Original article (short paper)
Perception of barriers to physical exercise in
women population over 60
Jéssica Bianca Aily
Universidade Federal de São Carlos, São Carlos, SP, Brazil
Letícia Carnaz
Universidade Sagrado Coração, Bauru, SP, Brazil
Ana Claudia Silva Farche Anielle Cristhine de Medeiros Takahashi
Universidade Federal de São Carlos, São Carlos SP, Brazil
Abstract — Aims: This study evaluated the possible barriers to the permanence of physical exercise (PE) of old women. Methods: The study population comprised 61 old women participants for at least one year of a supervised PE program, who underwent anamnesis, and applied the Barriers Questionnaire to Physical Activity Practice in the Elderly (QBPAFI). Exploratory factorial analysis was used to evaluate QBPAFI data. The analysis of principal component was applied to the 22 questions through orthogonal rotation to analyze the correlation between the questions. The Kaiser-Meyer-Olkin test was applied to evaluate the suitability of the sample size, and the Bartlett’s test to assess whether the original matrix correlation is an identity matrix. Eigenvalues greater than 1 were considered for analysis. Results: The motivational factor was the major determinant of perceived barriers (43.3%), followed by psychosocial (12.29%), facilities and appearance (8.75%), and exercise conditions (8.10%) factors. Conclusion: Knowing the beneits of
physical activity, and the main barriers that prevent the permanence of active old people to physical exercise programs, new strategies must be taken to increase the rate of adherence of this group.
dependence9,10. Thus, knowing and minimizing the barriers that have favored the abolition or insertion of old people in programs of physical activity is of great relevance.
A very pertinent fact in adherence to physical exercise is the perceived barriers to the practice of physical activity. Santariano, Haight e Tager11 concluded that the most cited barriers for the old population (above 75 years) to start exercise were medical reasons, fear of falls, and health. On the other hand, Nascimento, Gobbi, Hirayama, Brazão12, in a study that analyzed different levels of physical activity among old people identiied the existence of dis-ease, need for rest, lack of persistence, and already active enough as the most prevalent barriers in this age group. Still in this last study, the authors indicate that the level of physical activity of old people might modulate the perception of barriers. From what is usually observed in studies with sedentary older or with low level of physical activity, and knowing that the practice of physical exercise prevents diseases and maintains levels of functionality of old people, it can be evidenced a difference between perceived barriers to initiate physical exercise and perceived barriers by those who have been active for at least a year.
There are few studies that investigate the identiication of the main barriers that could lead to drop out of physical exercise by the old population. Once the main barriers to exercise are characterized, strategies can be drawn both to reduce barriers and to propose and develop programs of physical activaities that are more stimulating and enjoyable for the old people13. In this way, promoting greater adherence and maintenance of physical activity, aiming at positive relexions in the health, economic-social, and individually contributing to the quality of life of this old person. Thus, the main objective of this study was to evaluate the perception of barriers to the permanence of the physical exercise of old women participants for at least one year of a supervised physical exercise program.
Methods
Sample
This was an observational cross-sectional study, and data were collected in women from a community-dwelling of São Carlos-SP, Brazil, from December 2012.
This study was performed with old women aged over 60 years, and who had participated for at least 1 year in a supervised multimodal exercise program. The volunteers were invited to participate by lyers and local media. The classes were held three times a week, lasting 50 minutes, and included exercises for muscle strengthening, lexibility, aerobic conditioning, and coordinating abilities (balance, agility and rhythm), following the recommendations of American College Medicine Sports14.
Ethical aspects
The Human Research and Ethics Committee of Federal University of São Carlos (UFSCar), opinion 151.377/2012, approved this
project. After clarifying all the experimental procedures, the volunteers signed an informed consent form.
Inclusion criteria
Inclusion criteria were old women over 60 years, who had par-ticipated for at least 1 year in a supervised multimodal exercise program, and agreed to participate.
Experimental procedure
It was performed an anamnesis, raising data such as: name, age, address, marital status, total length of permanence in the exercise program, and number of years of study. In order to characterize individuals in relation to cognition and depressive symptoms, the Montreal Cognitive Assessment (MoCA) questionnaire was used (version translated and validated to Brazilian old people15), considering 25 points as a cut-off score and an addition of 1 point in the total cut score for every 10 years of study15, and Depression Scale Geriatric (GDS), considering 5 points as indicative of depression.
The Barriers Questionnaire to Physical Activity Practice in the elderly (QBPAFI), adapted by Nascimento, Gobbi, Hirayama, Brazão12, was used to assess barriers to physical activity. The QBPAFI is composed of 22 items or barriers accompanied by a ive-point Likert scale (never, rarely, sometimes, often and always). In this questionnaire, the participants must identify the frequency with which a certain barrier interferes in their deci-sions regarding the practice of physical activity. A previously trained evaluator applied the questionnaire.
Statistical analysis
Every statistical analyzes were performed using SPSS 17.0. The exploratory factorial analysis was used to evaluate data from the Barriers Questionnaire to Physical Activity Practice in the Elderly (QBPAFI). The principal component analysis was applied to the 22 questions through an orthogonal rotation (varimax) to analyze the correlation between the questions. The questions with p-values less than correlation matrix determinant were excluded from the analysis (question 2 “already active”, 3 “lack of company”, 6 “illness or injury”, 7 “poor health”, 20 “violence”, 21 “bad weather” and 22 “urinary incontinence”). The Kaiser-Meyer-Olkin test was applied to evaluate the adequacy of the sample size (values greater than 0.7), and the Bartlett’s test to evaluate if the original matrix correlation is an identity matrix. Eigenvalues greater than 1 were considered for analysis (Kaiser criterion).
Results
69.3 years, mean length of permanence in the physical exercise program of 6.61 years, and mean of 10.32 years of study.
Principal component analysis (PCA) was conducted on the 22 items of the questionnaire by an orthogonal rotation (varimax). Seven of the evaluated questions (2, 3, 6, 7, 20, 21 and 22) were removed from the model because they presented values lower than 0.5 for Kaiser-Meyer-Olkin (KMO) individual analysis. The general Kaiser-Meyer-Olkin (KMO) test revealed the suitability of the sample for the analysis, KMO = 0.748 (good sample size according to Field, 2009), and every KMO values for each ques-tion were greater than 0.609, which is above from acceptable limit of 0.5 (FIELD, 2009). The Barlett X² test (120) = 622.283, p <0.0001, indicated that correlations between the questions were large enough for PCA analysis. An initial analysis was performed to obtain the eigenvalues for each analyzed question. Four components presented eigenvalues greater than 1 (Kaiser
criterion) and in combination explained 72.5% of the variance. These components were identiied as factors: motivational, psychosocial, facilities and appearence and exercise conditions.
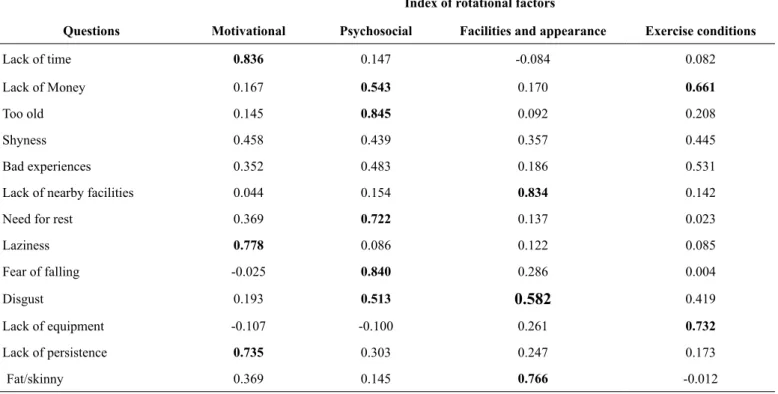
Motivational factor (43.30%) was the factor that most explained the perception of barriers, and the signiicant issues related to this factor were lack of time, laziness, lack of persis-tence, and lack of energy. The second factor that best explains the perception of barriers was psychosocial factor (12.29 %), where the questions, too old, need for rest and fear of falling showed greater prominence. The facilities and appearance factor that involved lack of nearby facilities, fat/skinny and disbelief in beneits and presented 8.75% of variance. Finally, the exercise conditions factor was the one that least explained the percep-tion of barriers and presented 8.10% of variance, where lack of equipment was the barrier most prominent. Table 2 showed the indexes of the factors after the rotation.
Table 1. Clinical characteristics of volunteers
Subjects (n=61)
Age (years) 69.27±5.84
Scholarity (years) 10.32± 5.61
Length of Permanence in Program 6.61± 1.62
MoCA 25.02± 2.09
GDS 1.84± 1.86
Table 1. Data presented on average ± standard deviation. MoCA = Montreal Cognitive Assessment, GDS = Depression Scale Geriatric.
Table 2. Summary of the results of the exploratory factor analysis for the Barriers Questionnaire to Physical Activity Practice in the Elderly.
Index of rotational factors
Questions Motivational Psychosocial Facilities and appearance Exercise conditions
Lack of time 0.836 0.147 -0.084 0.082
Lack of Money 0.167 0.543 0.170 0.661
Too old 0.145 0.845 0.092 0.208
Shyness 0.458 0.439 0.357 0.445
Bad experiences 0.352 0.483 0.186 0.531
Lack of nearby facilities 0.044 0.154 0.834 0.142
Need for rest 0.369 0.722 0.137 0.023
Laziness 0.778 0.086 0.122 0.085
Fear of falling -0.025 0.840 0.286 0.004
Disgust 0.193 0.513 0.582 0.419
Lack of equipment -0.107 -0.100 0.261 0.732
Lack of persistence 0.735 0.303 0.247 0.173
Discussion
Until now, in our knowledge, this is one of the few studies that evaluated the perception of barriers to physical activity in old women participants of a physical exercise program for at least 1 year. Most of the studies focus on sedentary old people and their perception of barriers to initiate physical activity12,16-18 or in old people, participants of physical activity programs, with time less than one year19,20.
The main inding of this study shows that for old women, already engaged in structured and supervised physical exercise programs for at least one year, the motivational factor was the major determinant for perceived barriers. In this way, questions as “lack of time”, “lack of energy”, “laziness” and “lack of persistence” were the most prevalent.
The motivational factor stands out in regard to “lack of time”, “lack of energy”, and “laziness”. Although most old are retired, they do not know how to schedule their free time, or they are often too busy caring for their grandchildren or sick partners, leading them to give up physical exercise. Franco, Tong, Howard, Sherrington, Ferreira, Pinto 13, analyzed that some old people reported having little or none time to perform physical activity. In addition, some of them felt that caring for fragile partners and grandchildren was more important than exercise13. According to Nascimento, da Silva, Saggioratto, Vargas, Schopf, Klunk 21, one of the hypotheses for such prevalence of exercise abandonment would be the poor ability to manage time, or a rational excuse for lack of motivation. However, timely availability may vary according to family role that the old person assumes, needing to take care of the family (partner or grandchildren) for periods of the day or week22.
In addition, lack of persistence also was identiied in the motivational factor. According to Nascimento, Gobbi, Hirayama, Brazão12 lack of persistence may be linked to issues such as
self-eficacy, which can be deined as a belief that the individual has in his/her own ability to perform a task23, may be a consistent
factor for maintaining the practice of physical exercise by old people20. Although the present study did not directly evaluate
this variable, Santarém24shows that elderly people who have a
greater sense of self-eficacy are more motivated, improve their physical itness levels and decrease the probability of develop-ing chronic diseases.
Regarding psychosocial factor, mourning and abandonment are one of the main causes of depression in old people, and they are directly related to loss of quality of life and social isolation25.
Picorelli, Pereira, Pereira, Felício26, emphasized in their study
that psychological factors such as depression and loneliness
were associated with low adherence. In addition, in this same study, Picorelli, Pereira, Pereira, Felício26, said that this group
of people requires even more encouragement, afirmation and feedback. Thus, the perception of barriers “disgust”, character-ized by the absence of happiness, annoyance and sadness, may be related to this aspect of depressive origin. From this, we can note a signiicant importance of the psychosocial approach in physical exercise programs aimed at the elderly, where in most cases these aspects are not taken into account.
Still on the psychosocial factor, Booth, Bauman, Owen27
observed that “too old” and “need for rest” are some of the main barriers to the physical activity, supporting the indings of the present study. Furthermore, Nascimento, Gobbi, Hirayama, Brazão12, and Takahashi, Carnaz, Farche, Rossi, Aily6suggested
that it is common to encounter discourses related to inadequacies of physical practice associated with old age condition, as “I’m too old” or “I need to rest” related to their work throughout life. Regarding to “fear of falling”, it is emphasized that approximately 30% to 40% of people aged 65 years and older who live in the community fall28. In a study with 839 older people, which
evalu-ated risk for falls, was observed that 43.1% to participants reported fear of falling29. Thus, the “fear of falling” can be considered
a barrier to falls during the physical exercise practice, as well as to falls during the route to the place of the physical exercise.
In this context, “lack of nearby facilities” was identiied in the facilities and appearance factor as an important barrier. According to recent review study30 old people feel unit and unable to use public transport, mainly when they need to catch multiple buses. Moreover, old people feel vulnerable when hav-ing to walk in busy or unsafe neighborhoods that demand more of their attention30. Still, most of old people depend of relatives to take them to physical exercise program when the place is far away from their homes 30.
In the facilities and appearance factor, we also founded that the perceived barriers were “fat/skinny” and “disbelief in beneits”. Kulavic, Hultquist, McLester31showed that physical
appearance is one of the most motivations to physical exercise practice. On the other hand, the present study observed that for old women who participated for at least 1 year in a supervised multimodal exercise program, the physical appearance (fat or skinny) might be a great problem. Concerning to “disbelief in beneits”, Franco et al.30 showed that older people report that
physical activity could not slow the natural process of aging and they believe that exercise are unnecessary for old people and may even be harmful.
The exercise conditions factor also has a contribution share, but of a lower magnitude for the sample. Thus, “lack of
Lack of energy 0.791 0.034 0.365 -0.023
Disbelief in beneits 0.136 0.261 0.725 0.335
Eigenvalues 6.929 1.967 1.401 1.297
equipment” and “lack of money” were also highlighted in the perception of barriers to exercise by old women active for over a year. In accordance with the present study, a systematic re-view30 demonstrated that from all studies included in the review, 55% of them pointed that the programs of physical exercise has unavailable equipment. In addition, costs associated with physical exercise program can be associated with transportation, appropriate clothes and healthy food 32.
When we look for tools to evaluate barriers to exercise, we found a lack of instruments. Thus, it is necessary to develop more speciic instruments that can be used to monitor the per -ception of barriers. This is extremely important because once the barriers presented by old people to physical exercise are identiied, interventions and ways of minimizing them tend to become more effective.
The study limitations were: the sample was composed only by women who had participated for at least 1 year in a supervised multimodal exercise program, which prevents the generalization of the results for the entire old population (both sexes); the preva-lence of high level of education of this population; and failure to track the level of self-eficacy of the individuals evaluated. Thus, more studies including men at the sample should be carried out to identify if the perceived barriers founded in the present study are similar or different between sexes. In addition, new tools to detect barriers to physical exercise should be implemented.
Thus, knowing the beneits of physical activity, and the main barriers that prevent the permanence of active old women to physical exercise programs, new strategies must be taken in order to increase the adherence rate of this group. One of these aspects is the need to hire trained professionals who work with older in a differentiated way and who value a good relationship with the participants, in order to minimize the barriers and increase the motivation of old people to practice physical exercise. In addition, the presence of multiprofessional group, with the participation of psychologists, occupational therapists, physiotherapists and physical educators, in order to minimize perceptions of moti-vational, psychosocial, and exercise conditions barriers can be a great motivator for the practice of physical exercise, since old people will be seen for different aspects. Finally, but not least, implementation of government subsidies to minimize individual costs to the practice of physical exercise should be considered in order to increase physical activity adherence.
Conclusion
It was concluded that the main perceptions of barriers to the continuity of physical exercise by active older women can be better explained by the motivational factor. Furthermore, the psychosocial, facilities and appearance, and exercise conditions factors were also highlighted in the perceptions of barriers, but to a lesser extent. Thus, the participation of a multiprofessional team (psychologists, occupational therapists, physiotherapists and physical educators) can minimize the perceptions of barriers to physical exercise; furthermore, physical exercise programs can be molded to increase the permanence of active old population participating in supervised physical exercise programs.
References
1. World Health Organization. “Ageing well” must be a global priority. Avaiable from: http://www.who.int/mediacentre/news/ releases/2014/lancet-ageing-series/en/. [Accessed 22th December 2015]
2. Quinn TJ, McArthur K, Ellis G, Stott DJ. Functional assessment in older people. BMJ. 2011; 343:4681. doi: 10.1136/bmj.d4681 3. Ellis G, Whitehead MA, Robison D, Neill DO, Langhorne, P.
Comprehensive geriatric assessment for older adults admit-ted to hospital: meta-analysis of randomised controlled trials. BMJ. 2011; 343 doi: 10.1136/bmj.d6553
4. Kemmler W, von Stengel S. Exercise frequency, health risk fac-tors, and diseases of the elderly. Arch Phys Med Rehabil. 2013; 94(11): 2046-53. doi: 10.1016/ j.apmr.2013.05.013.
5. Halaweh H, Willen C, Grimby-Ekman A, Svantesson U. Physical Activity and Health-Related Quality of Life Among Community Dwelling Elderly. J Clin Med Res. 2015; 7(11):845-52. doi: 10.14740/jocmr2307w
6. Takahashi ACM, Carnaz L, Farche ACS, Rossi PG, Aily JB. Motivation, adherence and dropout of physical exercise in older adults. In Physical Exercises: An Important Tool for Physical Therapy. New York, Nova Science Publishers; 2015. P245-254. 7. Caspersen CJ, Powell KE, Christenson GM. Physical Activity,
Exercise and Physical Fitness: Deinitions and Distinctions for Health-Related Research. Public Health Reports. 1985;100(2): 126–131.
8. Hong S, Hughes S, Prohaska T. Factors Affecting Exercise Attendance and Completion in Sedentary Older Adults: A Meta Analytic Approach. J Phys Act Health. 2008; 5: 385-397. doi: 10.1123/jpah.5.3.385
9. Nelson ME, Rejeski J, Blair SN, Duncan PW, Judge JO, King AC, et al. Physical Activity and Public Health in Older Adults. Circulation. 2007;116:1094-1105. doi: 10.1249/ mss.0b013e3180616aa2
10. Chodzko-Zajko WJ, Proctor DN, Singh MAF, Minson CT, Nigg CR, Salem GJ, et al. Exercise and Physical Activity for Older Adults. Med Sci Sports Exerc. 2009;41(7):1510-30. doi: 10.1249/ MSS.0b013e3181a0c95c.
11. Santariano WA, Haight TJ, Tager IB. Reasons given by older people for limitation or avoidance of leisure time physical activ-ity. J Am Geriatr Soc. 2000; 48(5):505-12. doi: 10.1111/j.1532-5415.2000.tb04996.x
12. Nascimento CMC, Gobbi S, Hirayama MS, Brazão MC. Nível de atividade física e as principais barreiras percebidas por idosos de Rio Claro. Rev Educ Fis. 2008;19(3):109-118. doi: 10.4025/ reveducis.v19i1.4321
13. Franco MR, Tong A, Howard K, Sherrington C, Ferreira PH, Pinto RZ, et al. Older people’s perspectives on participation in physical activity: a systematic review and thematic synthesis of qualitative literature. Br J Sports Med. 2015;49(19):1221-1222. doi: 10.1136/bjsports-2014-094015.
14. American College of Sports Medicine. Exercise and Physical Activity for Older Adults. Med Sci Sports Exerc. 2009;0195-9131(09):4107-1510. doi: 10.1249/MSS.0b013e3181a0c95c 15. Memória CM, Yassuda MS, Nakano EY, Forlenza OV. Brief
Brazilian version of the Montreal cognitive assessment. Int J Geriatr Psychiatry. 2013; 28 (1): 34-40. doi: 10.1002/gps.3787. 16. Dergance JM, Calmbach WL, Dhanda R, Miles TP, Hazuda HP,
Mouton CP. Barriers to and Beneits of Leisure Time Physical Activity in the Elderly: Differences Across Cultures. J Am Geriatr Soc. 2003;51:863-868. doi: 10.1046/j.1365-2389.2003.51271.x 17. Phillips EM, Schneider JC, Mercer GR. Motivating Elders
to Initiate and Maintain Exercise. Arch Phys Med Rehabil. 2004;85(3):58-9. doi: 10.1016/ j.apmr.2004.03.012
18. Newson RS, Kemps EB. Factors That Promote and Prevent Exercise Engagement in Older Adults. J Phys Act Health. 2007;19(3):470-481. doi: 10.1177/0898264307300169
19. Jancey J, Howat P, Lee A, Clarke A, Shilton T, Fisher J, et al.. Effective Recruitment and Retention of Older Adults in Physical Activity Research: PALS Study. Am J Health Behav. 2006;30(6):626-635. doi: 10.5993/AJHB.30.6.9
20. Cardoso AS, Borges LJ, Mazo GZ, Kuhnen AP. Fatores inluentes na desistência de idosos em um programa de exercício físico. Revista Movimento. 2008;14(1):225-239.
21. Nascimento MC, da Silva OMP, Saggioratto CML, Vargas KCC, Schopf K, Klunk J. O desaio da adesão aos exercícios físicos em grupos de idosos em Palmitos/ SC: Motivos para a prática e para a desistência. Rev Bras Ativ Fis Saúde. 2010;15(3):140-144, 2010. doi: 10.12820/ RBAFS.V.15N3P140-144
22. Manzano AB, Molina SF. Motivos de inscripción, permanencia y satisfacción em un programa de actividad física de manteniniento para mujeres mayores. Cuad Desporte. 2012;12(1):79-92. 23. Bandura A. Self-eficacy: toward a unifying theory of behav
-ioral change. Psychological Review. 1977;84(2):191-215. doi: 10.1037/0022-3514.35
24. Santarém JM. Promoção da saúde do idoso: a importância da ativi-dade física. Avaiable from: http://www.saudetotal.com/santarem. htm. Acesso em 30 de abril de 2011. [Accessed 03th April 2015]. 25. Wilcox S, King AC. The effects of life events and interpersonal
loss on exercise adherence in older adults. J Aging Phys Act. 2004;11:117-130. doi: 10.1123/japa.12.2.117.
26. Picorelli AMA, Pereira LS, Pereira DS, Felício D, Sherrington C. Adherence to exercise programs for older people is inluenced by program characteristics and personal factors: a system-atic review. J. Physiother. 2014; 60(3):151-156. doi: 10.1016/j. jphys.2014.06.012.
27. Booth ML, Bauman A, Owen N. Perceived barriers to physical activity among older Australians. J Aging Phys Act. 2002; 10:271-280. doi: 10.1123/japa.10.3.271.
28. Phelan EA, Mahoney JE, Voit JC, Stevens JA. Assessment and management of fall risk in primary care settings. Med.Clin. North. Am. 2015; 99(2): 281–293. doi:10.1016/j.mcna.2014.11.004. 29. Huang S, Duong T, Ieong L, Quach T. Understanding Falls Risk
and Impacts in Chinese American Older Patients at a Community Health Center. J Community Health. 2017. doi: 10.1007/ s10900-017-0315-x.
30. Franco MR, Tong A, Howard K, Sherrington C, Ferreira PH, Pinto RZ, et al. Older people’s perspectives on participation in physical activity: a systematic review and thematic synthesis of qualitative literature. Br J Sports Med 2015: 1-9. doi:10.1136/ bjsports-2014-094015.
31. Kulavic K, Hultquist CN, McLester JR. A comparison of motiva-tional factors and barriers to physical activity among tradimotiva-tional versus nontraditional college students. J Am Coll Health. 2013; 61(2):60-6. doi: 10.1080/07448481.2012.753890.
32. Franco MR, Howard K, Sherrington C, Ferreira PH, Rose J, Gomes JL, et al. Eliciting older people’s preferences for exercise programs: a best-worst scaling choice experiment. J Physiother. 2015 Jan; 61(1):34-41. doi: 10.1016/j.jphys.2014. 11.001.
Acknowledgement
We thank the FESC (Fundação Educacional São Carlos) for ceding the place for this research.
Corresponding author
Anielle Cristhine de Medeiros Takahashi
UFSCar, Federal University of São Carlos, Department of Physical Therapy, São Carlos, SP, Brazil. Rodovia Washington Luiz, km 235.
Email: [email protected]
Manuscripted received on December 12, 2016 Manuscripted accepted on March 16, 2017