SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
In
situ
repair
of
partial
articular
surface
lesions
of
the
supraspinatus
tendon
夽
Arildo
Eustáquio
Paim
a,baSantaCasadeBeloHorizonte,BeloHorizonte,MG,Brazil bHospitalMaterDeideBeloHorizonte,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received14June2016 Accepted21July2016 Availableonline28April2017
Keywords:
Shoulderjoint/injuries Shoulderjoint/surgery Arthroscopy
a
b
s
t
r
a
c
t
Objective:To demonstrate the in situ repair technique of high-degree partial-thickness articularsurfacelesionsofthesupraspinatustendon(SS).Theprocedureconsistsofthe arthroscopicsurgicalrepairoftheselesions,withouttheneedtocompletethelesion,as occursintraditionalclassicaltechnique.Asmallincisionismadeinthelongitudinal direc-tionoftheintactbursalfibersandwherebonefixationanchorsareintroduced,whichmakes theprocedureeasier.Theseanchorsaretransferredtothetendonandthusenabletherepair ofthelesion.
Methods:48shoulderswereoperatedintheperiod2010–2015.Theminimumfollow-upwas 12 monthsandmaximum60 months.Agesrangedfrom38years to75 years(mean54 years).Theywereindicatedfortherepairofhigh-degreesymptomaticlesionsandatleast 30%intactsuperiorbursalfibersofgoodquality.
Results:PatientswereevaluatedaccordingtotheUCLAcriteria,theresultswere:69% excel-lent,17%good,7%fair,and7%poor.Fairresultsoccurredinthreepatientswithassociated symptomsofpolyarthralgiawhoremainedwithresidualpain.Threepatientsdeveloped postoperativejointstiffness(7%).
Conclusion: Theprocedureunderstudyissafeandeasytoreproduce.Itshowshighratesof positiveresults(86%).TheopeningmadeinthebursalsideoftheSStendonallowedthe arthroscopetoremaininthesubacromialspace,makingiteasiertoperformsurgery.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatSantaCasadeBeloHorizonteandHospitalMaterDeideBeloHorizonte,BeloHorizonte,MG,Brazil. E-mail:[email protected]
http://dx.doi.org/10.1016/j.rboe.2017.04.004
304
r e v b r a s o r t o p . 2017;52(3):303–308Técnica
de
reparo
in
situ
das
lesões
parciais
da
superfície
articular
do
tendão
do
supraespinal
Palavras-chave:
Articulac¸ãodoombro/lesões Articulac¸ãodoombro/cirurgia Artroscopia
r
e
s
u
m
o
Objetivo:Demonstraratécnicadereparoinsitudaslesõesdeespessuraparcialdasuperfície articulardealtograudotendãodosupraespinal(SE).Oprocedimentoconsistenoreparo cirúrgicodessaslesõesporviaartroscópica,semanecessidadedecompletaralesão,como ocorrenatécnicaclássicatradicional.Éfeitaumapequenaincisãolongitudinalnosentido dasfibrasintactasbursais,porondesãointroduzidasasâncorasdefixac¸ãoóssea,oque tornamaisfáciloprocedimento.Essasâncorassãotransferidasparaotendãoeassimse fazoreparodalesão.
Métodos:Foramoperados48ombrosde2010a2015.Oseguimentomínimofoide12mesese omáximode60.Aidadevarioude38anosa75(médiade54).Foramindicadasparaoreparo aslesõessintomáticasdealtograuqueapresentassempelomenos30%dafibrassuperiores bursaisintactasedeboaqualidade.
Resultados: OspacientesforamavaliadossegundooscritériosdaUniversidadeda Califór-nia emLos Angeles(UCLA),obtiveram-seresultados excelentesem69%,bons em17%, razoáveisem7%eruinsem7%.Osresultadosrazoáveisocorreramemtrêspacientesque apresentavamsintomasassociadosdepoliartralgiaepermaneceramcomdorresidual.Três pacientesdesenvolveramrigidezarticularnopós-operatório(7%).
Conclusão: Oprocedimentoem estudoéseguro edefácil reprodutibilidadeeapresenta altosíndicesderesultadospositivos(86%).AaberturafeitanoladobursaldotendãodoSE permitiuamanutenc¸ãodoartroscópionoespac¸osubacromialetornoumaisfácilacirurgia. ©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
PartialtypeAsupraspinatus(SS)tendonlesionsare incom-pletetearslocatedonthelower surfaceofthetendonwith intactfibersonthesuperiorside.Theyarealsoknownas par-tialarticularsupraspinatustendonavulsion(PASTA)lesions.1
Theselesionsmayproducesymptomsandsurgeryisindicated afterfailureofconservativetreatment.
There are two different techniques for closing PASTA lesions,bothofwhichcanbeperformedvideoarthroscopically. Theclassicaltechnique2isthe“completeandrepair,”thatis,
toclosethedefectitisnecessarytodetachtheSStendonfrom thegreatertubercleofthehumerus.Thistransformsthe par-tiallesionintoacompletelesion,sothatthetraditionalrepair withanchorscanbemade.Theothertechniqueisthe trans-tendonrepair,1 whichconsistsofreconstructingthe lesion
withoutdetachingthebursalfibers.Fixationanchorsare intro-ducedfromabovethroughthesefibersandclosureismadeby thesutureanchors.Forthistechnique,itisnecessaryto con-stantlymovethearthroscopefromtheglenohumeraljointto thesubacromialspaceandviceversa.
Theauthordescribesamethodsimilartotraditional trans-tendonrepair,butsimplerandmorereproducible.Thisstudy aimed to demonstrate this surgical method, developed by the author to facilitate the procedure. Following the same principleoflongitudinalopeningtheSStendontointroduce intramedullarynailsintothehumerus,afterclosure,healingis facilitated.Basedonthisaspect,asmalllongitudinalopening ismadeintheintactfibersinwhichtheanchorsareinserted to be fixated into the bone and then transferred into the
tendonsothatthesuturecanfinallybemade.Inthis tech-nique,thearthroscopecanbekeptinthesubacromialspace duringtheentiresurgicalprocedure.
Material
and
methods
Thisstudy wasapprovedbythe InstitutionalReviewBoard underCAAENo.56917516.1.0000.5138.
48shoulderswereoperatedfrom2010to2015.Minimum postoperativefollow-uptimewas12monthsandmaximum was60months.Ofthe42evaluatedshoulders,34(81%)were fromfemalepatientsandeight(19%)frommalepatients;32 were onthe rightsideand10ontheleft side.Patient’sage rangedfrom38to75years(mean54years).Partialarticular SSlesion(typeA)wasdiagnosedbyradiographyandmagnetic resonanceimaging(MRI)inallcases.Surgerybythistechnique wasindicatedinsymptomaticpatientsrefractorytotreatment byphysicaltherapy,corticosteroidinfiltration,andanalgesic useforatleastthreemonths.LesionswerepartialtypeAof highgrade,andtheyhadatleast30%intact,goodquality supe-riorfibersobservedonMRIandconfirmedbyarthroscopy.The casesofassociationwithother procedures– suchasdistal clavicleresection,bicepstenodesis,andglenohumeraljoint instability–wereexcludedfromthestudy.
Surgicaltechnique
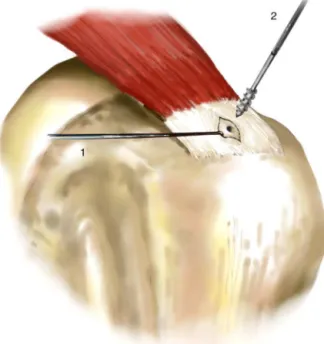
Fig.1–Portals:(1)posterior;(2)posterosuperior;(3)lateral; (4)anterior;(5)anterosuperior.
anteriorportalsaremade(Fig.1),aswellasan anterosupe-riorminiportal. Initially, ajoint inspection isperformed to diagnoseandcorrectotherexistingassociatedlesions.Then, theclassical fibrillation ofthe lower portionofthe SS ten-donisvisualized.Atthistime,theassistantsurgeonforces theshoulderintoapproximately80◦ ofabduction,and
infe-riorlysubluxatesthe humeralheadtoimprove theview of thearticularsurfaceoftheSStendon.Throughtheanterior portal,asofttissueshaverisusedtodebrideallfibrillation andprepareabonebed.Thelesionismarkedwithasuture marker,whichisintroducedfromabovethroughaJelcoNo.14 (Fig.2)cathetertobepositionedonthebursalside.Thiswire shouldbelocatedinthemostmedialportionofthelesion andinthenormaltendontransition.Duringbursoscopy,the suturemarkerislocatedandtheposterolateralportalismade, towhichthearthroscopeistransferred.Afterthebursectomy, ashouldercannulaisplacedinthelateralportalandaprobe isusedtoassess thequalityoftheremainingintactfibers; ifthequality ispoor, i.e., thefibersare friableand translu-cent,then thepreferredapproachistocompletetheinjury andperformtherepair.Ifthequalityisgood,thentheinsitu repairtechniqueisused. Atthis point,a longitudinal inci-sionofapproximately10mmlongismadeinthedirectionof thetendonfibers,fromthesuturemarkertowardthegreater tuberosity,without damaging the tendon insertion (Fig. 2). Thisopeningmeetsthebonebed,whichhasalreadybeen pre-paredduringthejointinspection.Thisincisionisopenedwith aretractortoimprovedepthvision(Fig.3).Then,an acces-soryanterosuperiorminiportalismade,fromtheoutsidein,
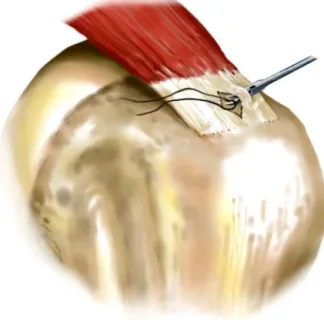
Fig.2–(1)Suturemarkerdelimitingthelocationofthe partialarticularlesionoftheSSnotvisibleinthe
bursoscopy.(2)Longitudinalincisioninthedirectionofthe SStendonfibers,untilreachingthebonebedinferiorlyfor theintroductionoftheanchors.
controlledwithaJelcoNo.14catheter,seekingthebest posi-tion for the entry of the anchors, which should make an angleofapproximately 15◦ withthehumeralshaft. Two
5-mmanchors,preferablyabsorbable,areintroduced,oneata time,throughthisportal(Fig.3).Throughtheopening,they
306
r e v b r a s o r t o p . 2017;52(3):303–308Fig.4–Eachtipoftheanchorwireistransportedtothe tendonviawirepasseratdifferentpoints.
arefixatedtothebonebed,oneattheanteriorendandthe otherattheposteriorend.TheNo.2anchorwiresmustbe non-absorbableandresistant.Thesewiresaretransferredto thetendonviawirepassersatapproximately6mmfromthe edgeofthe openingon each side(Fig. 4).Closure ismade withasuturebridge;thelooseendsoftheposteriorwiresare joinedwiththetipsoftheanteriorwires,sothatthetendon iscompressedinferiorlyoverthebonebedandthe longitu-dinalopeningisclosed(Figs.5and 6).Thearthroscopecan bemovedtotheposterolateralandlateralportalswhen nec-essaryforbettervision;itremainsinthesubacromialspace throughoutthesurgery.Inthefinalrevision,theinsertionof thesupraspinaltendonintothelargertuberremainsintact,
Fig.5–Thewiresoftheanteriorandposterioranchors, alreadytransportedtotheSStendon.
Fig.6–Thelooseendsoftheanterioranchorwireare connectedwiththetipsoftheposterioranchorwire throughabridgesuture.
withoutanydetachment.Inthepostoperative(PO)period,a slingisusedforfourweeksandthepatientisorientedto per-formactiveelbowandhandexercisesandpassiveshoulder exercises. Rehabilitationfollows thetraditionalprotocolfor POrehabilitationofrotator cuffrepair.Theassisted physio-therapystartssixweeksaftersurgery.
Results
PatientswereevaluatedaccordingtoUCLAcriteria;theresults obtainedwere69%excellent,17%good,7%fair,and7%poor. POMRIwasperformedineightcasesandultrasonographyin four.Allimagesshowedhealingofthelesion(Figs.7and8). Thefairresultswereobservedinthreepatientswhohad pol-yarthralgiasymptomsandremainedwithresidualpain.Three patientsdevelopedPOjointstiffness(7%)andprogressedwell with conservative treatment through physical therapy and analgesicuse.
Discussion
Fig.7–PreoperativeT2-weightedMRIcoronalcutofright shouldershowspartial-thicknessSSlesionofhighgrade.
Fig.8–SamecaseasinFig.7.MRIoneyear postoperatively,showingthehealedSS.
Partialjointrupturesaremorefrequent,intheratioof3:1in relationtotypeBruptures.2Theiretiologyandpathogenesis
aremultifactorial,andbothintrinsicandextrinsicfactorsare involved.Traumaticlesionsaremorefrequentlyobservedin youngpatients.1
Studies showthat theincidenceoftheselesions ranges from13%to37%.2Theyarefrequentcausesofshoulderpain
inyoungerpatients.Itisacceptedthathigh-gradelesionsare indicatedforsurgicalrepairafterfailureofconservative treat-ment.Theauthorindicatedneedforsurgeryinsymptomatic casesthatdidnotimproveafteratleastthreetosixmonths ofconservativetreatment,whichconsistedofanalgesicuse, corticoid infiltration, and physiotherapy forstretching and musclestrengthening.
Surgeriesarealwaysdonebythearthroscopicroute.For lowandmoderatedegreelesions,onlydebridementis indi-cated.Tendonrepairisindicatedforhighgradesymptomatic lesions. Two techniques are used for reconstruction. The classic methodistoconvert the partialinjuryinto a com-pleteinjury andthenperformtheconventionalrepairwith anchors.2 Transtendon repair, initiallydescribed bySnyder
etal.,1consistsofreconstructingthetorninferiorfiberswhile
preservingtheintactsuperiorfibers.Theanchorsare intro-ducedthroughthesebursalfibers.Theliteratureshowsthat bothtechniquesleadtogoodresults.3
Nonetheless, there are still conflicting opinions regard-ing them. Supporters of completing the injury claim that thetranstendonrepairistechnicallymoredifficultandthat thetissueofintactfibersisalwaysofpoorquality.4,5
Tradi-tionalrepairissimplerandclinicalresultsarefavorable.2The
present author completes theselesions only inhigh-grade ruptureswherelessthan30%ofthetendonisintactandthe poorqualityofthetissueinitiallyseeninMRIisconfirmedby arthroscopy.
Proponents6–8ofthetranstendonrepairtechniquesuggest
that theintactfibers ofthe bursalside aresubstantial and protecttherepairedmedialpart,presentingahighpotential forhealingafterrepair,inadditiontoavoidingthepromotion oftendonshorteningandleadingtoamoreanatomic heal-ing.Mazzoccaetal.,9inacadavericstudy,demonstratedthat
insitutranstendonrepairrestoresthestrengthoftheintact rotatorcuff.Clinicalstudiesdemonstratethatthisrepairhas betterfunctionalresultswhencomparedwiththetraditional “completeandrepair”technique.10
Accordingtotheauthor,toperformtheclassic transten-donrepairdescribedbySnyderet al.,1 thefixationanchors
areintroducedthroughtheintacttendonbursalside,which requiresthearthroscopetobetransferredfromthejointto thesubacromialspace,andviceversa.Thismakestheprocess moredifficultandtime-consuming.Theauthordevelopedthis new in situ repairtechnique by followingthe principles of transtendonrepair.Asmalllongitudinalopeningismadeon the upperfibers ofthe tendon and throughit the anchors are introduced, tobe fixated into the bone bed. Through-outthesurgery,thearthroscoperemainsinthesubacromial space,whichfacilitatesthetechniqueandshortensthetime ofsurgery.
Someauthors2havewarnedthattranstendonrepairsare
308
r e v b r a s o r t o p . 2017;52(3):303–308Conclusions
ThisstudyshowedthattheinsiturepairoftypeApartialSS lesionissafeandreproducible.Itpresentedhighratesof pos-itiveresults(86%),andthecomplicationrateswerelow.The longitudinalopeningonthebursalsideoftheSStendon facil-itatedtheintroduction ofthefixationanchorsand allowed themaintenanceofthearthroscopeinthesubacromialspace throughouttheentiretendonsuture.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SnyderSJ,PachelliAF,PizzoWD,FriedmanMJ,FerkelRDF, PatteeG.Partialthicknessrotatorcufftears:resultsof arthroscopictreatment.Arthroscopy.1991;7(1):1–7.
2. GartsmanGM.Shoulderarthroscopy.Philadelphia:Saunders; 2003.
3. StraussEJ,SalataMJ,KercherJ,BarkerJU,McGillK,BachBRJr, etal.Thearthroscopicmanagementofpartial-thickness rotatorcufftears:asystematicreviewoftheliterature. Arthroscopy.2011;27(4):568–80.
4. YamakadoK,HayashiS,KatsuoS.Histopathologyofthe residualtendoninhigh-gradearticular-sided
partial-thicknessrotatorcufftears(PASTAlesions)(SS-12). Arthroscopy.2011;27(5):34–5.
5.KarthikeyanS,DamianRG,ParsonsN,LawrenceTM,Chetan LS,StephenMJ,etal.Microvascularbloodflowinnormaland pathologicrotatorcuffs.JShoulderElbowSurg.
2015;29(12):1954–60.
6.JinS,SangS,ShinJ.Acomparisonof2repairtechniquesfor partial-thicknessarticular-sidedrotatorcufftears.
Arthroscopy.2012;28(1):25–33.
7.LomasGG,KippeMA,BrownGD,GardnerTR,DingA,Levine WN,etal.Insitutranstendonrepairoutperformstear completionandrepairforpartialarticular-sided supraspinatustendontears.JShoulderElbowSurg. 2008;17(5):722–8.
8.KamathG,GalatzLM,KeenerJD,TeefeyS,MiddletonW, YamaguchiK.Tendonintegrityandfunctionaloutcomeafter arthroscopicrepairofhigh-gradepartial-thickness
supraspinatustears.JBoneJointSurgAm.2009;91(5):1055–62.
9.MazzoccaDA,RinconLM,O’ConnorRW,ObopilweE, AndersenM,GeaneyL,etal.Intra-articularpartial-thickness rotatorcufftearsanalysisofinjuredandrepairedstrain behavior.AmJSportsMed.2008;36(1):110–6.
10.CastagnaA,BorroniM,GarofaloR,RoseGD,CesariE,PaduaR, etal.,ContiAffiliatedwithIRCCSIstitutoClinico
HumanitasM.Deeppartialrotatorcufftear:transtendon repairortearcompletionandrepair?Arandomizedclinical trial.KneeSurgSportsTraumatolArthrosc.2015;23(2):460–3.
11.KyleDS,KarzelRP,GanjianpourM,SnyderSJ.Long-term outcomeforarthroscopicrepairofpartialarticular-sided supraspinatustendonavulsion.Arthroscopy.