SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Prevalence
of
femoroacetabular
impingement
morphology
in
asymptomatic
youth
soccer
players:
magnetic
resonance
imaging
study
with
clinical
correlation
夽
Anthony
Kerbes
Yépez
a,∗,
Marcelo
Abreu
b,
Bruno
Germani
a,
Carlos
Roberto
Galia
caSantaCasadePortoAlegre,DepartamentodeCirurgiaOrtopédica,PortoAlegre,RS,Brazil bHospitalMãedeDeus,DepartamentodeRadiologia,PortoAlegre,RS,Brazil
cUniversidadeFederaldoRioGrandedoSul,HospitaldeClínicasdePortoAlegre(HCPA),DepartamentodeCirurgiaOrtopédica,Porto
Alegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30November2016 Accepted26January2017 Availableonline24June2017
Keywords:
Femoroacetabularimpingement Hipjoint
Soccer
Magneticresonanceimaging
a
b
s
t
r
a
c
t
Objective:To determine the prevalence of femoroacetabular impingement morphology (FAIM),cam-orpincer-type,bymagneticresonanceimaging(MRI)inasymptomatic ado-lescentsoccerplayers,andtoevaluatethepossiblecorrelationbetweenalterationsonMRI andclinicalexaminationfindings.
Methods:Across-sectionalstudywasconductedtodeterminetheprevalenceofFAIMin asymptomaticyouthsoccerplayersaged13–18years.Atotalof112hipsin56players(mean age15.3years)wereevaluatedbyMRI.Imageswereexaminedbytwomusculoskeletal radio-logistsforsignsofFAIM.Cam-type(impingement)deformitywasdiagnosedbyalphaangle ≥55◦
orhead–neckoffset<7mm.Pincer-type(impingement)deformitywasdiagnosedby center-edgeangle(CEA)≥35◦
oracetabularindex≤0◦
.OtherMRIchanges,characteristic ofFAIM,wereobserved.Clinicalexaminationwasperformedtodeterminetherangeof motion(ROM)ofthehips.Inaddition,specifictestsforanterolateralandposteroinferior impingementwereperformed.
Results:TheprevalenceofMRIfindingsconsistentwithFAIMamongthisyoungpopulation was84.8%(95/112).Thealphaanglewas≥55◦
in77.7%(87/112)ofhips,whiletheCEAwas alteredin10.7%(12/112)ofhips.QualitativeMRIfindingsconsistentwithFAIMwerehighly prevalent,andincludedlossofsphericityofthefemoralhead(77%),osseousbump(44%), femoralneckedema(21%),andacetabularosteitis(9%).Theanteriorimpingementtestwas positivein15%ofthehipsevaluated.
夽
StudyconductedattheUniversidadeFederaldoRioGrandedoSul,FaculdadedeMedicina,HospitaldeClínicasdePortoAlegre(HCPA), DepartmentofOrthopedicSurgery,PortoAlegre,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.K.Yépez).
http://dx.doi.org/10.1016/j.rboe.2017.06.005
Conclusion: YouthsoccerplayershaveahighprevalenceofFAIMasdiagnosedbyMRI.There isnocorrelationbetweenphysicalexaminationfindingsandMRIevidenceofFAIMinthis population.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopediae Traumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Prevalência
da
morfologia
de
impacto
femoroacetabular
em
jogadores
de
futebol
juvenil
assintomáticos:
estudo
de
ressonância
magnética
com
correlac¸ão
clínica
Palavras-chave:
Impactofemoroacetabular Articulac¸ãodoquadril Futebol
Ressonânciamagnética
r
e
s
u
m
o
Objetivo:Determinaraprevalênciadamorfologiadeimpactofemoroacetabular(MIFA),tipo camoupincer,porressonânciamagnética(RM)emjogadoresdefuteboladolescentese assintomáticos,bemcomoavaliarapossívelcorrelac¸ãoentreasalterac¸õesobservadasna RMeosachadosdoexameclínico.
Métodos: EsteestudotransversaltevecomoobjetivodeterminaraprevalênciadeMIFAem jogadoresdefuteboljuvenilassintomáticos,comidadeentre13e18anos.Umtotalde112 quadrisde56jogadores(idademédia15,3anos).Asimagensforamexaminadaspordois radiologistasmusculoesqueléticos,comoobjetivodeidentificarsinaisdeMIFA.A deformi-dade(impacto)dotipocamfoidiagnosticadaquandooânguloalfa≥55◦
oudesvioentre acabec¸aeocolofemoral<7mm.Adeformidade(impacto)dotipopincerfoi diagnosti-cadaquandooângulocentro-borda(ACB)≥35◦ouíndiceacetabular≤0◦.Outrasalterac¸ões
característicasdeMIFAforamobservadasnaRM.Aamplitudedemovimento(ADM)dos quadrisfoideterminadaapartirdeumexameclínico.Alémdisso,foramrealizadostestes específicosparaimpactosanterolateraiseposteroinferiores.
Resultados: AprevalênciadeachadosdeRMconsistentescomMIFAnessapopulac¸ãofoi de84,8%(95/112).Oânguloalfafoi≥55◦
em77,7%(87/112)dosquadris,enquantooACB apresentoualterac¸õesem10,7%(12/112)dequadris.Observou-seumaaltaprevalênciade achadosqualitativosde RMconsistentescomMIFA,incluindoperdade esfericidadeda cabec¸afemoral(77%),elevac¸ãoóssea(44%),edemafemoral(21%),eosteiteacetabular(9%). Otestedeimpactoanteriorfoipositivoem15%dosquadrisavaliados.
Conclusão: OsexamesdeRMindicaramumaaltaprevalênciadeMIFAentrejogadoresde futeboljuvenil.Nestapopulac¸ão,nãohouvecorrelac¸ãoentreosachadosdoexamefísicoe aevidênciadeMIFAobservadanaRM.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Femoroacetabularimpingement (FAI) is a condition result-ing from abnormalcontactbetween the femoralhead and theacetabularrim,usuallycausedbyachangein morphol-ogyoftheproximalfemurand/oracetabulum.1–4Ganzetal.2 described two basic mechanisms of FAI: cam and pincer. Thecammechanismoccursinpatientswithanon-spherical femoralheadorwithadecreasedoffsetbetweentheheadand neckoffemur.Theimpingementareaistypicallylocatedon theanterolateralportionofthefemoralhead–neckjunction. Pincerimpingement,inturn,ischaracterizedbyacetabular overcoveragecausedbyanexcessoftheanteriorwall.1,2,4,5
FAImay decreasethe rangeofmotion(ROM)ofthehip, especially in internal rotation (IR) of the flexed hip.2,6 FAI isdescribed asacause ofhippainexacerbatedbyphysical activity,andoccursmainlyinyoungadultpatients.4,5Clinical
symptomsusuallydonotappearuntiladulthood;however, detection ofFAIMisbecomingincreasinglycommon inthe pediatricpopulation.7Patientsoftendevelopcartilagelesions andinjurytotheacetabularlabrum,whichcanprogresstohip osteoarthritis(OA)iftheanatomicchangesarenottreatedor thephysicalactivitymodified.2,8–10
Adolescent patients who practice sports often perform high-impactactivitiesthatrequireextrememovementsofthe hip,whichmaypredisposetomorefrequentandmoreintense conflictsbetweentheproximalfemurandtheacetabulum.11
Physicalactivityduringbonegrowthseemstobeassociated withanincreasedriskofcam-typedeformity.Siebenrocketal. suggestedthatcamimpingementinyoungathletesmaybe relatedtoanabnormalityinthephysealplate.Studiesin high-performanceadolescentbasketballandhockeyplayersfound ahighincidenceofcamtypeFAI.3,12
soccerplayersasdiagnosedbymagneticresonanceimaging (MRI)findings.Patientsalsounderwentaclinicalevaluation ofthehip jointstoascertainpossiblecorrelations between changesonMRIandclinicalsignsofFAI.
Materials
and
methods
Demographics
FromJuly2012toJuly2013,56athletesfromafirst-division Brazilianyouthsoccer teamwere selectedtoparticipatein thestudy.Theypracticesoccerincompetitionlevel,training amean offivehours perday.All athleteswere aged13–18 yearsanddidnothaveanysymptomsofhippathology.The dominantsideofeachathletewasidentified.Theexclusion criteriaforthisstudywereanyhistoryoftreatmentforpain relatedtothehipjointandcontraindicationsorintoleranceto MRI.
Writteninformedconsentwasobtainedfromallathletes andfromtheparentsorguardiansofathletesunder18years old.Theinformed consentformwasapprovedbythe local institutionalreviewboard.
Magneticresonanceimagingevaluation
MRIwas performedin a1.5-T scannerusing the following parameters:panoramicT1coronalsequencesincludingboth hips(echotimesof10–14msandrepeattimesbetween400 and600ms)andT2(echotimesof35–70msandrepeattimes between2000and 3500ms),withaslicethicknessof5mm and512×256linematrixwithafieldofviewof33–36cm;T2 sequencesfocusedonthehipjoints,withandwithoutfat sat-urationinthecoronal,sagittal,andobliqueaxialslices,with athicknessof4mmanda384×224linematrixwithafieldof viewof22–25cm.
Based on the radiographic appearance of the capital femoralphysisonMRI,participantswerestratifiedintothose withopenphysealplatesandthosewithclosedphysealplates. Cammorphologywasevaluatedbymeasuringthealpha angleandfemoralhead–neckoffset.Thealphaanglewas mea-suredonanobliqueaxialsequence asdescribedelsewhere intheliterature.Participantswithanalphaangle≥55◦were diagnosedwithcammorphology13,14(Fig.1).
Thefemoralhead–neckoffsetwasmeasuredbydrawinga lineinthecenterofthefemoralheadandneckandtwoparallel lines,onealongtheanteriorcortexofthefemoralneckandthe otheralongtheanteriorouterpartofthefemoralhead.The distancebetweenthesecondandthirdlinescorrespondsto thehead–neckoffset,and,whenlessthan7mm,isindicative ofcamdeformity15(Fig.2).
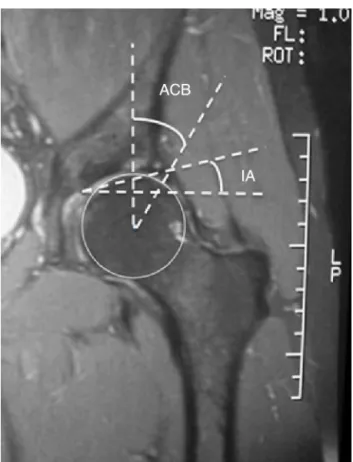
Thediagnosis ofpincer morphology was establishedby measuringthecenter-edgeangle(CEA),orWibergangle,and theacetabularindex(AI),orTönnisangle.ACEA≥39◦ orAI ≤0◦indicatespincerdeformity.TheCEAwasmeasuredonthe coronalplane,betweenaverticallinepassingthroughthe cen-terofthefemoralheadandanotherlinedrawnfromthecenter ofthefemoralheadtothe lateralacetabularrim.TheAIis definedastheanglebetweenahorizontallineandanother lineconnectingthemedialpointofthescleroticzoneofthe
Fig.1–MRIoftherighthip(axialobliqueview)for measurementofthealphaangle.Imagerepresentativeof alteredalphaangle.
Fig.2–Femoralhead–neckoffset<7mmindicatescam deformity.
acetabularroofand the lateral edgeoftheacetabulum16,17 (Fig.3).
Other MRIalterations consistentwithFAIconsideredby the examiningradiologists were osseous bump,18 synovial pit,6,7,14,19–22 bone edema in the femoral neck, acetabular osteitisandlesionsofthelabrumand/oracetabularcartilage.
Physicalexamination
Fig.3–CEAandtheAIindicativeofpincerdeformity.
anterolateralandposteroinferiorimpingementwerealso per-formed.
Theanteriorimpingementtest wasperformed withthe patientinthesupineposition,flexingthehip90◦,with adduc-tionandinternalrotation.Thetestwasconsideredpositiveif itelicitedpain.2,6
Theposteroinferiorimpingementtestwasperformedwith thepatientinthesupineposition,hangingthelegoverthe end of the bed while in extension and external rotation. Again,thetestwasconsideredpositiveifthepatientreported pain.20,23
Statisticalanalysis
Two independent musculoskeletal radiologists, blinded to physicalexaminationfindings,analyzedtheMRIscans. Con-cordancebetweentheirresultswasassessedusingthekappa index,whichisconsideredsatisfactorywhen>0.7.Incaseof discrepancybetweenexaminers,athird,experienced radiolo-gistconductedanotherevaluation.
Theresultswere entered into aMicrosoft Excel spread-sheet and exported to PASW Statistics, version 18.0, for analysis. Quantitative variables were described as means andstandarddeviations,andcategoricalvariables,as abso-lute and relative frequencies. Prevalence was reported with95% confidence intervals. Comparisonsofcontinuous variables were performed using the independent samples
t-test.
Table1–Distributionofpatientsbyage.
Age n %
13 7 12.5
14 15 26.8
15 10 17.9
16 11 19.6
17 7 12.5
18 6 10.7
Total 56 100.0
Table2–PrevalenceofMRIfindingsindicativeof femoroacetabularimpingementmorphologyinthe sample(n=56,112hips).
MRIfinding Prevalence(%) 95%CI
Lossofsphericity 73 65–82
Decreasedhead–neckoffset 57 48–66
Alphaangle≥55◦ 77.7 69.8–85.5
Acetabularindex≤0◦ 0 0
Wibergangle≥39◦ 10.7 4.9–16.5
Osseousbump 44 34–53
Sinovialpit 4 0–7
BMEathead/neckjunction 21 14–29
Labrallesion 8 3–13
Degenerativelabrallesion 2 −1to4
Acetabularosteitis 9 4–14
Chondrallesion 3 0–6
BME,bonemarrowedema;CI,confidenceinterval;MRI,magnetic resonanceimaging.
Results
Baselinedemographics
Atotal of56male athletes(112hips)were included inthe study. Noathletes were excluded. Themean age was 15.3 years,withadistributionasshowninTable1.Therightside wasdominantin80.3%(45/56)oftheathletes.Therewasno significantdifferenceintheprevalenceofFAIMoncomparison ofthedominantandcontralateralhips.
MRIfindings
Concordance between the findings of the two examining radiologists was satisfactory; therefore, analysis bya third radiologistwasnotnecessary.Thebestinter-rater concord-ancewasinthealphaangle,withakappacoefficientof0.91.
TheprevalenceofabnormalitiescharacteristicofFAIMwas 84.8%(95/112)(95%CI78–91.5%).TheMRIchangesobserved, andtheirrespectiveprevalence,aredescribedinTable2.
Abnormalalphaangle(≥55◦)wasobservedin77.7%(87/112) ofhips,whileabnormalfemoralhead–neckoffset(<7mm)was seenin57%(64/112).Thealphaanglewasalteredinall indi-viduals withreduced offset.Thephysealplatewasopenin 23.2%(13/56)ofathletes.Therewasnosignificantdifference intheprevalenceofalteredalphaanglebetweenathleteswith anopenphysealplateandthosewithaclosedphysealplate.
Table3–NumberofMRIchangesfoundinthesample (n=56,112hips).
Numberof changes
Frequency Percentage Cumulative percentage
0 17 15.2 15.2
1 9 8.0 23.2
2 8 7.1 30.4
3 20 17.9 48.2
4 24 21.4 69.6
5 19 17.0 86.6
6 11 9.8 96.4
7 2 1.8 98.2
8 2 1.8 100.0
Total 112 100.0
Table4–Resultsofrangeofmotion(ROM)testsin patientswithandwithoutMRIevidenceof femoroacetabularimpingementmorphology.
Variable MRIevidence ofFAIM
NoMRI evidenceof
FAIM
p
Flexion 127.9±5.6 126.5±7.8 0.48
Extension 9.9±1.5 10.6±1.7 0.12
Adduction 32±4.5 31.5±3.4 0.64
Abduction 47.4±4.4 48.5±3.8 0.31
IR 43±11.2 46.8±10.7 0.2
ER 49.3±8.2 48.2±4.6 0.43
ER,externalrotation;FAI,femoroacetabularimpingement;IR, inter-nalrotation;MRI,magneticresonanceimaging.
Resultsexpressedasmean±standarddeviation.p-valuesfrom Stu-dent’st-testforindependentsamples.
100%(6/6)in18-year-olds. Therewere nosignificant differ-encesinprevalenceacrossdifferentages.
Areasofbonemarrowedema(BME)wereobservedinthe femoral head–neckjunction of24 hips (21%), all ofwhich exhibitedanelevatedalphaangle.Acetabularlabrallesions wereidentifiedin10hipsandchondrallesionswerefoundin three.
All hips had an AI ≥2◦. A CEA >39◦ was seen in10.7% (12/112)ofthehips,indicatingadiagnosisofpincerdeformity. PooledanalysisofMRIfindings(Table3)showedthatmost ofthehips(76.8%)hadmorethanonealterationsuggestiveof FAI,and>50%hadfourormoresuchchanges.
CorrelationbetweenMRIandphysicalexamination
findings
TheresultsofROMmeasurementarepresentedinTable4. TherewasnosignificantassociationbetweenROMandMRI findingsconsistentwithFAI.Concerningtheposteroinferior andanterolateralimpingementtests,theformer was nega-tiveinallathletes, whilethelatterwaspositivein17hips, ofwhich15showedfindingssuggestiveofFAIonMRIscans. Therewasnosignificantdifferenceintheprevalenceof posi-tiveimpingementtestresultsbetweenhipswithandwithout signsofFAI.Evenwhenanalphaangle≥65◦wasconsidered diagnosticofcam-typeimpingement,therewasnocorrelation betweenalphaangleandpositiveanterolateralimpingement
test.TherewasnocorrelationbetweenMRIchangesand phys-icalexaminationfindings.
Discussion
Physicalactivityduringbonegrowthmaybeassociatedwith anincreasedriskofFAIdeformity,whichcanprogresstohip OAduringadulthood.Thisisthefirststudytoassessthe preva-lenceofMRIchangesconsistentwithFAIMinasymptomatic youth soccer players and analyze the potential correlation betweenthesechangesandphysicalexaminationfindings.
The prevalence of MRI changes indicative of FAIM in the present samplewas84.8%.This isahigherprevalence thanthatreportedinpreviousstudiesofsoccerplayers.24–26 Whencomparingtheprevalenceofpathologicalalphaangle only(≥55◦,cam-typedeformity),the77.7%ratefoundinthe present study was higher than those reported byGerhardt et al.25 (68%) and Johnsonet al.26 (60%), both studies that evaluatedadultsoccerplayersusingplainradiography.Itwas also higher than the 26% prevalence reported by Agricola et al. who evaluated adolescent soccer players using plain radiography,butconsideringthealphaangleabnormalonly if>60◦.24–26 Thiscanbeexplainedbythegreatersensitivity ofMRIcomparedtoplainradiographyinidentifyingchanges thatcharacterizeFAI.27–29Theexcellentconcordancebetween theexaminingradiologistsinmeasuringthealphaangle,with akappacoefficientof0.91,demonstratesthereproducibilityof MRIfordiagnosisofcam-typeimpingement.
MRIfindingsofcamdeformityinthepresentsamplewere verysimilartothosereportedinpreviousstudiesofadolescent athletesinothersports.Siebenrocketal.30reportedan89% prevalenceofcamdeformityinbasketballplayersaged9–25 years,includingafterphysealclosure.Philipponetal.found analphaangle≥55◦in75%ofhockeyplayersbetweentheages of10and18.21
Comparingtheprevalenceofcamdeformityinthepresent studywiththeresultsofFranketal.31inasystematicreview aboutprevalenceofFAIMinasymptomaticvolunteers,itwas higherthanthe37–54.8%foundinathletesandmuchhigher thanthe23.1%inthegeneralpopulation.
A high prevalence of cam-type impingement morphol-ogyinyounghigh-levelathletescorroboratesthehypothesis proposedbySiebenrocketal.,12whichsuggestsadirect rela-tionshipbetweenphysicalactivityandahigherincidenceof cam-typeFAIM,probablyduetoenlargementofthephyseal plate. The finding ofMRI evidence ofBME in the femoral head/neckjunction in21.4%ofhips(24/112)inthissample ishighlysuggestiveofstress-relatedchanges,whichsuggest activeFAIandprobablyprecedethedevelopmentoffemoral head–neckbumpdeformity.
Theprevalenceofcamdeformitywassimilarbetween ath-leteswithopenandclosedphysealplates,whichsuggestthat thecamisformedevenbeforephysealplategrowthis com-pleted.Ifthislesioniscausedbystressfromboneimpaction, theearlieritstarts,thegreaterthepotentialfordamage;the immature skeletonis more complacent, and can easilybe remodeledbyabnormalforces.
activ-ityormovementthatcausesFAI.Simplestressoverthephysis duringphysicalactivitiescouldexplainthehighprevalenceof cam-typeimpingementmorphology.
TheidentificationoftwoormoreMRIchangesindicative ofFAIin 76.8% ofhips, inan entirely asymptomatic sam-ple,underlinesthe importanceofcarefulassessmentwhen recommendingsurgicalprocedurestopatientsinwhom diag-nosisisbasedsolelyonMRIfindings.Monitoringofathletes couldhelpdefinehowmanyofthesepatientswoulddevelop symptomsandrequiresurgery.Follow-upofthepresent sam-plewouldallowidentificationtheincidenceofchondraland labrallesionsinyouthsoccerplayers,aswellasidentification ofwhichlevelofsportspracticeintensitycouldbeconsidered ariskfactorforhipOA.
When athleteswithsigns ofimpingementon MRIwere comparedtothosewithnormalhips,nosignificantdifferences inROMoranterolateralandposteroinferiorimpingementtest resultswerefound.Thissuggeststhat,inasymptomaticyouth soccerplayers,physicalexaminationfindingsareinconclusive regardingthediagnosisofFAI.Furthermore,itsuggeststhat MRIcanrevealabnormalitiesconsistentwithFAIMbeforethey becomeapparentonclinicalexamination.
The inverse relationship between increased prevalence ofFAI and reduced IR described in the literaturewas not confirmed inthis study, probably because the samplewas asymptomaticandveryyoung(i.e.,asubclinicalpopulation).32 Any decrease in IR or ER could be important, because of thepossibilityofincreasedriskofanteriorcruciateligament rupture.33
Limitations
Thelimitationsofthisstudyincludethelackofacontrolgroup ofadolescents who didnotpracticephysicalactivitiesata highlevel.Weplantoconductamatchedcase–controlstudy toevaluatetheprevalenceofthesefindingsinanormal pop-ulation.Inaddition,theagerangeoftheathletescouldhave beenextendeddownto10years,whichwouldhaveallowed betterassessmentofthetimingofFAIMonset,especiallyof cam-typeFAI.
Conclusion
Theyouthsoccerplayerswhoparticipatedinourstudyhad ahighprevalenceofabnormalitiescharacteristicofFAIMon MRI.Physical examinationfindingsdid notcorrelated with MRIevidenceofFAIM.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. ClohisyJC,KnausER,HuntDM,LesherJM,Harris-HayesM, PratherH.Clinicalpresentationofpatientswithsymptomatic
anteriorhipimpingement.ClinOrthopRelatRes. 2009;467(3):638–44.
2.GanzR,ParviziJ,BeckM,LeunigM,NötzliH,SiebenrockKA. Femoroacetabularimpingement:acauseforosteoarthritisof thehip.ClinOrthopRelatRes.2003;(417):112–20.
3.ItoK,MinkaMA2nd,LeunigM,WerlenS,GanzR. Femoroacetabularimpingementandthecam-effect.A MRI-basedquantitativeanatomicalstudyofthefemoral head–neckoffset.JBoneJointSurgBr.2001;83(2):171–6.
4.SinkEL,GrallaJ,RybaA,DaytonM.Clinicalpresentationof femoroacetabularimpingementinadolescents.JPediatr Orthop.2008;28(8):806–11.
5.FabricantPD,HeyworthBE,KellyBT.Hiparthroscopy improvessymptomsassociatedwithFAIinselected adolescentathletes.ClinOrthopRelatRes.2012;470(1):261–9.
6.PhilipponMJ,MaxwellRB,JohnstonTL,SchenkerM,Briggs KK.Clinicalpresentationoffemoroacetabularimpingement. KneeSurgSportsTraumatolArthrosc.2007;15(8):1041–7.
7.PhilipponMJ,YenYM,BriggsKK,KuppersmithDA,Maxwell RB.Earlyoutcomesafterhiparthroscopyfor
femoroacetabularimpingementintheathleticadolescent patient:apreliminaryreport.JPediatrOrthop.
2008;28(7):705–10.
8.BeauléPE,KimYJ,RakhraKS,StelzenederD,BrownTD.New frontiersincartilageimagingofthehip.InstrCourseLect. 2012;61:253–62.
9.BeckM,KalhorM,LeunigM,GanzR.Hipmorphology influencesthepatternofdamagetotheacetabularcartilage: femoroacetabularimpingementasacauseofearly
osteoarthritisofthehip.JBoneJointSurgBr. 2005;87(7):1012–8.
10.SchmitzMR,CampbellSE,FajardoRS,KadrmasWR. Identificationofacetabularlabralpathologicalchangesin asymptomaticvolunteersusingoptimized,noncontrast1.5-T magneticresonanceimaging.AmJSportsMed.
2012;40(6):1337–41.
11.KeoghMJ,BattME.Areviewoffemoroacetabular impingementinathletes.SportsMed.2008;38(10):863–78.
12.SiebenrockKA,BehningA,MamischTC,SchwabJM.Growth platealterationprecedescam-typedeformityinelite basketballplayers.ClinOrthopRelatRes.2013;471(4):1084–91.
13.JohnstonTL,SchenkerML,BriggsKK,PhilipponMJ. Relationshipbetweenoffsetanglealphaandhipchondral injuryinfemoroacetabularimpingement.Arthroscopy. 2008;24(6):669–75.
14.NötzliHP,WyssTF,StoecklinCH,SchmidMR,TreiberK, HodlerJ.Thecontourofthefemoralhead–neckjunctionasa predictorfortheriskofanteriorimpingement.JBoneJoint SurgBr.2002;84(4):556–60.
15.ClohisyJC,NunleyRM,OttoRJ,SchoeneckerPL.Thefrog-leg lateralradiographaccuratelyvisualizedhipcam
impingementabnormalities.ClinOrthopRelatRes. 2007;462:115–21.
16.KuttyS,SchneiderP,FarisP,KieferG,FrizzellB,ParkR,etal. Reliabilityandpredictabilityofthecentre-edgeangleinthe assessmentofpincerfemoroacetabularimpingement.Int Orthop.2012;36(3):505–10.
17.StelzenederD,HingsammerA,BixbySD,KimYJ.Can radiographicmorphometricparametersforthehipbe assessedonMRI?ClinOrthopRelatRes.2013;471(3):989–99.
18.FritzAT,ReddyD,MeehanJP,JamaliAA.Femoralneck exostosis,amanifestationofcam/pincercombined femoroacetabularimpingement.Arthroscopy. 2010;26(1):121–7.
20.ParviziJ,LeunigM,GanzR.Femoroacetabularimpingement.J AmAcadOrthopSurg.2007;15(9):561–70.
21.PhilipponMJ,HoCP,BriggsKK,StullJ,LaPradeRF.Prevalence ofincreasedalphaanglesasameasureofcam-type femoroacetabularimpingementinyouthicehockeyplayers. AmJSportsMed.2013;41(6):1357–62.
22.PittMJ,GrahamAR,ShipmanJH,BirkbyW.Herniationpitof thefemoralneck.AJRAmJRoentgenol.1982;138(6):1115–21.
23.CrawfordJR,VillarRN.Currentconceptsinthemanagement offemoroacetabularimpingement.JBoneJointSurgBr. 2005;87(11):1459–62.
24.AgricolaR,BessemsJH,GinaiAZ,HeijboerMP,vander HeijdenRA,VerhaarJA,etal.ThedevelopmentofCam-type deformityinadolescentandyoungmalesoccerplayers.AmJ SportsMed.2012;40(5):1099–106.
25.GerhardtMB,RomeroAA,SilversHJ,HarrisDJ,WatanabeD, MandelbaumBR.Theprevalenceofradiographichip abnormalitiesinelitesoccerplayers.AmJSportsMed. 2012;40(3):584–8.
26.JohnsonAC,ShamanMA,RyanTG.Femoroacetabular impingementinformerhigh-levelyouthsoccerplayers.AmJ SportsMed.2012;40(6):1342–6.
27.BartonC,SalinerosMJ,RakhraKS,BeauléPE.Validityofthe alphaanglemeasurementonplainradiographsinthe evaluationofcam-typefemoroacetabularimpingement.Clin OrthopRelatRes.2011;469(2):464–9.
28.MasjediM,MarquardtCS,DrummondIM,HarrisSJ,CobbJP. Camtypefemoro-acetabularimpingement:quantifyingthe diagnosisusingthreedimensionalhead–neckratios.Skeletal Radiol.2013;42(3):329–33.
29.DuddaM,AlbersC,MamischTC,WerlenS,BeckM.Do normalradiographsexcludeasphericityofthefemoral head–neckjunction?ClinOrthopRelatRes.2009;467(3):651–9.
30.SiebenrockKA,FernerF,NoblePC,SantoreRF,WerlenS, MamischTC.Thecam-typedeformityoftheproximalfemur arisesinchildhoodinresponsetovigoroussportingactivity. ClinOrthopRelatRes.2011;469(11):3229–40.
31.FrankJM,HarrisJD,EricksonBJ,SlikkerW3rd,Bush-Joseph CA,SalataMJ,etal.Prevalenceoffemoroacetabular impingementimagingfindingsinasymptomaticvolunteers: asystematicreview.Arthroscopy.2015;31(6):1199–204.
32.ReichenbachS,JüniP,WerlenS,NüeschE,PfirrmannCW, TrelleS,etal.Prevalenceofcam-typedeformityonhip magneticresonanceimaginginyoungmales:a cross-sectionalstudy.ArthritisCareRes(Hoboken). 2010;62(9):1319–27.