3 6 4
Rev Lat ino- am Enfer m agem 2006 m aio- j unho; 14( 3) : 364- 71w w w . eer p. usp. br / r lae
CEREBROVASCULAR ACCI DENT I N THE AGED: CHANGES I N FAMI LY RELATI ONS
Sueli Mar ques1 Rosalin a Apar ecida Par t ezan i Rodr igu es2 Lu cian a Ku su m ot a3
Mar qu es S, Rodr igu es RAP, Ku su m ot a L. Cer ebr ov ascu lar acciden t in t h e aged: ch an ges in f am ily r elat ion s. Rev Lat ino- am Enfer m agem 2 0 0 6 m aio- j unho; 1 4 ( 3 ) : 3 6 4 - 7 1 .
The aim s of t his st udy w er e: t o ident ify aged per sons w ho w er e v ict im s of Cer ebr ov ascular Accident and r eceiv ed car e at t he Em er gency Unit of a Public Hospit al in Ribeir ão Pr et o- SP, Br azil, and t heir r espect iv e fam ilies, as w ell as t o ident ify t he changes in fam ily r elat ions t hat occur r ed aft er t he event . I n or der t o ident ify t hese changes, t he adapt ed Cr it ical I ncident Technique w as used, w hile t he analy sis w as based on t he idea of Cur r ent of Thought . The sam ple consist ed of 11 fam ilies, t ot aling 34 par t icipant s. The analysis of t he consequences display ed t he changes in fam ily r elat ions, w hich m ade up 1 3 subcat egor ies, 5 of w hich w er e posit iv e and 8 negat iv e, t ot aling 58 alt er at ions, 30 of w hich w er e posit iv e and 28 negat iv e. The st udy r ev ealed t he need t o w or k w it h t he fam ily in or der t o ident ify changes and develop an act ion plan t o favor t he fam ily’s r elat ions and adapt at ion t o t he dem ands, w it h a v iew t o im pr ov ing t he liv ing condit ions of it s m em ber s, including t he aged p er so n .
DESCRI PTORS: aged; cer ebr ov ascu lar acciden t ; f am ily ; n u r sin g
EL ANCI ANO TRAS ACCI DENTE CEREBROVASCULAR:
ALTERACI ONES EN EL RELACI ONAMENTO FAMI LI AR
Las f in alid ad es d e est e est u d io f u er on las d e id en t if icar a los an cian os con d iag n óst ico m éd ico d e Accident e Cer ebr ov ascular , at endidos en la Unidad de Em er gencia de un Hospit al Guber nam ent al de Ribeir ão Pr et o- SP, Br asil, y a su s r esp ect iv as f am ilias y t am b ién id en t if icar las alt er acion es en el r elacion am ien t o fam iliar , que ocur r ier on t r as el event o. Fue ut ilizada la Técnica de I ncident es Cr ít icos adapt ada par a ident ificar las alt er aciones en el r elacionam ient o fam iliar ocur r idas t r as la enfer m edad. Par a el análisis, fue adopt ada la r eflexión del Cam ino del Pensam ient o. La m uest r a fue com puest a por 11 fam ilias, t ot alizando 34 par t icipant es. El an álisis de las con secu en cias r ev eló las alt er acion es en el r elacion am ien t o fam iliar , qu e con st it u y er on 1 3 subcat egor ías, 5 posit ivas y 8 negat ivas, con un t ot al de 58 alt er aciones, siendo 30 posit ivas y 28 negat ivas. El est udio r ev eló la necesidad de t r abaj ar con la fam ilia par a ident ificar las alt er aciones y desar r ollar un plan de acción que pueda fav or ecer las r elaciones y la adapt ación de la fam ilia a las dem andas, con v ist as a m ej or ar las condiciones de v ida de sus m iem br os, incluso el anciano.
DESCRI PTORES: an cian o; acciden t e cer ebr ov ascu lar ; f am ilia; en f er m er ía
O I DOSO APÓS ACI DEN TE VASCULAR CEREBRAL:
ALTERAÇÕES NO RELACI ONAMENTO FAMI LI AR
Os obj et iv os dest e est u do for am : iden t ificar os idosos at en didos, n a Un idade de Em er gên cia de u m hospit al gover nam ent al do m unicípio de Ribeir ão Pr et o- SP, com diagnóst ico m édico de acident e vascular cer ebr al, e su as r espect iv as f am ílias, bem com o iden t if icar as alt er ações, n o r elacion am en t o f am iliar , qu e ocor r er am a p ó s o ev en t o . Ut i l i zo u - se a Técn i ca d e I n ci d en t es Cr ít i co s a d a p t a d a p a r a i d en t i f i ca r a s a l t er a çõ es n o r elacionam ent o fam iliar ocor r idas após a doença e, par a a análise, a r eflex ão do Cam inho do Pensam ent o. A am ost r a const ou de 11 fam ílias, t ot alizando 34 par t icipant es. A análise das conseqüências r evelou as alt er ações no r elacionam ent o fam iliar , que const it uír am 13 subcat egor ias, 5 posit ivas e 8 negat ivas, per fazendo o t ot al de 58 alt er ações, sendo 30 posit iv as e 28 negat iv as. O est udo r ev elou a necessidade de t r abalhar com a fam ília par a ident ificar as alt er ações e desenvolver um plano de ações que possa favor ecer as r elações e a adapt ação da fam ília às dem andas, com v ist as a m elhor ar as condições de v ida de seus m em br os, inclusiv e o idoso.
DESCRI TORES: idoso; aciden t e cer ebr ov ascu lar ; f am ília; en f er m agem
1 Junior Pr ofessor, e- m ail: sm ar ques@eer p.usp.br ; 2 Full Pr ofessor, e- m ail: r osalina@eer p.usp.br ; 3 Assist ant Pr ofessor, e- m ail: kusum ot a@eer p.usp.br.
Univer sit y of São Paulo at Ribeir ão Pr et o College of Nur sing - WHO Collabor at ing Cent r e for Nur sing Resear ch Developm ent
D ispon ív e l e m lín gu a por t u gu e sa n a SciELO Br a sil w w w .scie lo.br / r la e
I NTRODUCTI ON
C
er eb r ov ascu lar Acci d en t ( CVA) i s on e of t h e m o st p r e v a i l i n g n e u r o l o g i ca l p r o b l e m s i n t h ecat egor y of car diov ascular sy st em diseases. I t is t he
t h i r d m o st co m m o n ca u se o f d e a t h i n d e v e l o p e d
cou n t r ies. Ap p r ox im at ely 2 0 % of p at ien t s w h o ar e
v ict im s of CVA die w it hin one m ont h; about 50% of
s u r v i v o r s p r e s e n t p e r m a n e n t a n d c o n s i d e r a b l e
d i s a b i l i t i e s , n e e d i n g c a r e a n d s u p e r v i s i o n ; t h e
r em aining 30% pr esent neur ological deficit s, but ar e
capable of leading an independent life( 1).
Aft er a per iod in hospit al, aged vict im s of CVA
c a n g o b a c k h o m e w i t h p h y s i c a l a n d e m o t i o n a l
se q u e l a e , w h i ch a f f e ct t h e i r f u n ct i o n a l ca p a ci t y,
independence and aut onom y, and can also exert social
and econom ic effect s t hat inv ade all aspect s of life.
I n general, w hen a funct ional decline occurs as a result
of som e pat hological process, it is t he fam ily t hat get s
involved in care aspect s, supervision of responsibilit ies
an d dir ect car e deliv er y.
H o s p i t a l s a r e r e d u c i n g t h e i r c l i e n t s ’
hospit alizat ion period due t o different fact ors, including
healt h care cost s. How ever, aft er hospit alizat ion, aged
per sons’ r et ur n hom e r equir es car e and at t ent ion. The
e f f e ct s o f t h i s r e t u r n o n a g e d p e r so n s a n d t h e i r
f am ilies can of t en b e d est r u ct u r in g , as it d em an d s
t h e a v a i l a b i l i t y o f sp a ce , a ca r e g i v e r a n d , a l so ,
econom ic resources. Nevert heless, m ost elderly prefer
t o r eceiv e car e at hom e.
S i g n i f i c a n t e v e n t s i n l i f e , s u c h a s t h e
a p p e a r a n c e o f a c h r o n i c d i s e a s e , d i v o r c e ,
unem ploym ent or deat h of a r elat ive can br ing about
r elev an t t r an sf or m at ion s in t h e f am ily sy st em as a
w h o l e . Th e s e c h a n g e s c a n a f f e c t t h e c o g n i t i v e ,
a f f e c t i v e o r b e h a v i o r a l d o m a i n s . H o w e v e r, a n
alt er at ion in on e of t h em cau ses an im p act in t h e
ot hers. I t is im port ant for nurses w ho w ork w it h fam ilies
t o ca r ef u l l y o b ser v e a n d a ssess t h ese a sp ect s t o
enable t hem t o ident ify changes and develop a nur sing
int ervent ion plan t hat is capable of cont ribut ing t o t he
achiev em ent of a new balance in t he fam ily sy st em .
The change in fam ily st r uct ur e is exper ienced
as a dist ur bance in it s syst em . Fam ily syst em s aim t o
p r eser v e t h eir st ab ilit y. An alt er at ion is seen as a
b eh av ior al ch an g e, w h ich m ay b e accom p an ied b y
j udgm ent or not and, t hus, suggest s an invest igat ion
of differences in fam ily int eract ion pat t erns. Alt erat ion
and st abilit y m ust be consider ed j oint ly( 2).
Ch a n g e s a r e c o n s t a n t i n o u r s o c i a l
in t er act ion s an d en v ir on m en t , b u t w e of t en d o n ot
not ice and get used t o t hem . I n fam ilies t oo, alt erat ions
const ant ly develop and nur ses w or king in t his cont ext
m ay be aw ar e of t his fact or not . This is t he t ype of
cont inuous or spont aneous alt er at ion t hat happens in
d a i l y l i f e a n d i n v o l v e s t h e st a g e s o f f a m i l y a n d
in div idu al dev elopm en t( 3 ).
Nur ses should obt ain fam ilies’ act ive and
responsible part icipat ion in care for dependent elderly.
How ever, t o achieve t his, t here is a need t o invest in
r esear ch an d in cr easin gly in clu de f am ilies in h ealt h
ca r e.
Considering t he relevance of t his t hem e, t his
st u dy aim ed t o iden t if y aged per son s w h o r eceiv ed
car e at t h e Em er g en cy Un it of a Pu b lic Hosp it al in
Ri b e i r ã o Pr e t o - S P, B r a z i l , a n d w e r e v i c t i m s o f
( hem or r hagic or ischem ic) Cer ebr ov ascular Accident ,
w h o se f i r st e p i so d e o ccu r r e d i n 2 0 0 2 , a n d t h e i r
respect ive fam ilies, as w ell as t o ident ify t he changes
in fam ily r elat ions t hat occur r ed aft er t he CVA, using
an adapt ed ver sion of t he Cr it ical I ncident Technique.
METHODOLOGY
We car r ied out a qualit at ive st udy. Dat a w er e
collect ed by m eans of t he Crit ical I ncident Technique,
w it h a view t o ident ifying t he changes in fam ily relat ions
t h at o ccu r r ed af t er o n e f am i l y m em b er b ecam e a
v ict im of CVA.
The Cr it ical I ncident Technique cov er s a set
of pr ocedur es t o obt ain dir ect obser vat ions of hum an
behav ior, st im ulat ing it s applicat ion t o solve pract ical
problem s. The crit ical incident refers t o an observable
an d com p let e h u m an act iv it y t h at p er m it s m ak in g
i n d u ct i o n s a n d f o r eca st s a b o u t w h o p er f o r m s t h e
act iv it y. I t sh ou ld h appen in sit u at ion s in w h ich t h e
in t en t ion or obj ect iv e of t h e per son per f or m in g t h e
act iv it y is clear t o t h e obser v er, an d it s r esu lt s ar e
sy st em at ically def in ed( 4 ).
I n su m m ar y, t h e t ech n iq u e inv olv es ask in g
an act iv it y ’s agent s for r epor t s about sit uat ions t hey
ex per ien ced. Th e r esear ch er obser v es an d an aly zes
t h ese r ep o r t s i n v i ew o f a p r ev i o u sl y est a b l i sh ed
ob j ect iv e.
St udy par t icipant s w er e fam ilies w ho lived in
Ribeir ão Pr et o- SP and included an aged per son of 60
3 6 6
Cer ebr ovascular accident in t he aged...Mar ques S, Rodr igues RAP, Kusum ot a L.
Rev Lat ino- am Enfer m agem 2006 m aio- j unho; 14( 3) : 364- 71 w w w . eer p. usp. br / r lae
U n i t o f t h e H CFM RP- U S P, a n d w a s a v i c t i m o f
( hem or r hagic or ischem ic) Cer ebr ov ascular Accident ,
w hose fir st episode occur r ed in 2002.
Fam ilies w er e select ed in August 2003, aft er
t he st udy had been appr oved by t he Resear ch Et hics
Com m it t ee at t he Univer sit y of São Paulo at Ribeir ão
Pr et o Medical School Hospit al das Clínicas.
We asked t he Hospit al’s Medical and St at ist ical
Filing Ser v ice for a list of pat ient s aged 60 or older,
w ho w er e v ict im s of CVA and had been at t ended at
t h e Em er g en cy Un it in 2 0 0 2 , t h eir r ecor d n u m b er,
addr ess and phone num ber, t ot aling 109 aged per sons.
Af t er t h is su r v ey, w e f ir st con t act ed t h ese per son s’
fam ilies t o set a t im e for t he int erview s. The follow ing
exclusion cr it er ia w er e adopt ed: pat ient s w ho had died
an d pat ien t s w h o did n ot liv e in Ribeir ão Pr et o. We
int er v iew ed 11 fam ilies, t ot aling 34 par t icipant s. The
n u m b er of in t er v iew ed f am ilies w as d et er m in ed b y
t he sat ur at ion point of answ er s.
Dat a w er e collect ed fr om August t o Novem ber
2003. For t he int er view s, w e used t w o dat a collect ion
inst rum ent s w it h open and closed quest ions. The first
w as an ident ificat ion quest ionnair e w it h social pr ofile
inform at ion: dat e and t im e of birt h, gender, color, civil
s t a t u s , n u m b e r o f c h i l d r e n , e d u c a t i o n l e v e l ,
pr ofession / occu pat ion , in com e ( in m in im u m w ages) ,
addr ess an d t eleph on e.
Th e secon d in st r u m en t w as a qu est ion n air e
t o: a) ident ify t he elder ly v ict im ’s fam ily, cont aining:
f am ily com posit ion , m on t h ly in com e an d r eligion of
each m em ber ; b) ident ify changes in fam ily r elat ions
aft er t his ev ent s, using t w o quest ions elabor at ed t o
obt ain t he crit ical incident s: 1) Think of sit uat ions t hat
happened aft er t he elder ly r et ur ned hom e, aft er t he
h o sp i t al i zat i o n p er i o d , b ecau se ( s) h e su f f er ed t h e
st r oke. 2) Tr y t o r em em ber sit uat ions r elat ed t o t he
e l d e r l y a n d t h e s t r o k e , i n v o l v i n g t h e f a m i l y
en v i r o n m en t an d i t s m em b er s, w h i ch y o u b el i ev e
cau sed p osit iv e/ n eg at iv e alt er at ion s. Tell m e ab ou t
t he sit uat ions, w hich persons w er e involved, w hat t hey
d i d an d w h at t h e r esu l t w as. We f i r st r ef er r ed t o
p o si t i v e a l t e r a t i o n s a n d t h e n r e p e a t e d t h e sa m e
quest ion for negat iv e alt er at ions.
One of t he r esear cher s collect ed dat a at t he
fam ilies’ hom es, aft er a first cont act by t elephone and
each p ar t icip an t ’s con sen t . Bet w een t w o an d t h r ee
v isit s and an av er age of t hr ee phone cont act s w er e
r ealized for each fam ily.
Th e r e p o r t s o f t h e s e s i t u a t i o n s w e r e
r egist er ed in t he field diar y and, at t he end of each
r epor t , t he t ext w as r ead aloud t o be validat ed by t he
int erview ees. The researcher’s observat ions w ere also
r eg ist er ed .
Th e an aly sis w as b ased on t h e id ea of t h e
Cu r r en t of Th ou gh t , pr esen t ed as “ t h e possibilit y of
t echnical r ealizat ion r elat ed t o com m unicat ions in t he
h ealt h ar ea”( 5 ). All collect ed m at er ial, in clu d in g t h e
m eaning of social relat ions, w as j oined in t he analysis
t o ident ify changes in fam ily r elat ions. I n t his st udy,
w e a n a l y ze d t h e co n se q u e n ce s o f t h e si t u a t i o n s
ex per ien ced by t h e f am ily m em ber s.
I n accor d an ce w it h r esolu t ion s 1 9 6 / 9 6 an d
2 5 1 / 9 7 by t h e Nat ion al Healt h Cou n cil, t h is pr oj ect
w as ev aluat ed by t he Resear ch Et hics Com m it t ee at
t he Univ er sit y of São Paulo at Ribeir ão Pr et o Medical
Sch ool Hosp it al d as Clín icas. I t w as ap p r ov ed in a
m eet in g on 0 8 / 1 8 / 2 0 0 3 as HCRP Pr ocess No 4 7 0 0 /
2 0 0 3 .
RESULTS
Th e r esu lt s w ill be pr esen t ed in t w o st eps,
d escr ib ed b elow : a) I d en t if icat ion of Ag ed Per son s
Diagnosed as CVA and t heir Respect ive Fam ilies and
b) Descr ipt ion of changes in fam ily r elat ions.
I dent ificat ion of Aged Per sons Diagnosed as CVA and
t h eir Respect iv e Fam ilies
All aged per sons w er e vict im s of CVA in 2002
and w er e at t ended at t he at t he Em er gency Unit of
t he Univ er sit y of São Paulo at Ribeir ão Pr et o Medical
School Hospit al das Clínicas.
Their ages r anged fr om 62 t o 84 year s, w it h
a m ean age of 7 3 . 4 y ear s. Sev en pat ien t s ( 6 3 . 6 % )
w er e m en. Most ( 7 2 . 7 % ) CVA v ict im s w er e m ar r ied
an d t h r ee ( 2 7 . 3 % ) w idow ed. Fiv e ( 4 5 . 4 % ) pat ien t s
k n ew h ow t o r ead an d w r it e, fou r ( 3 6 . 4 % ) h ad n ot
f i n i sh e d p r i m a r y e d u ca t i o n , o n e ( 9 . 1 % ) f i n i sh e d
secondar y educat ion and one ( 9. 1% ) w as illit er at e.
As t o pr ofession/ occupat ion, m ost par t icipant s
w er e r et ir ed. Five ( 45.4% ) ear ned one m inim um w age
p er m on t h , t w o ( 1 8 . 2 % ) on e an d a h alf m in im u m
w ages, one ( 9.1% ) ear ned four m inim um w ages, one
( 9 . 1 % ) si x m i n i m u m w a g e s p e r m o n t h a n d t w o
( 1 8 . 2 % ) d id n ot h av e t h eir ow n in com e. Wh at t h e
m edical diagnosis is concer ned, 10 pat ient s ( 90. 9% )
w er e v ict im s of ischem ic CVA, and only one ( 9 . 1 % )
O n e f a m i l y ( 9 . 1 % ) c o n s i s t e d o f s e v e n
m e m b e r s , f o l l o w e d b y t h r e e ( 2 7 . 3 % ) w i t h s i x
m e m b e r s , o n e ( 9 . 1 % ) w i t h f i v e m e m b e r s , t w o
( 1 8 . 2 % ) w it h four m em ber s, one ( 9 . 1 % ) w it h t hr ee
m em ber s and t hr ee ( 27. 3% ) w it h t w o m em ber s. On
t he aver age, t he 11 fam ilies consist ed of 4.3 m em ber s.
I n t e r m s o f f a m i l y i n co m e , f i v e ( 4 5 . 4 % )
f am ilies r eceiv ed b et w een on e an d a h alf an d t w o
m inim um w ages, four ( 36.4% ) bet w een t w o and four
m inim um w ages, t w o ( 18. 2% ) bet w een four and six
and only one ( 9 . 1 % ) r eceiv ed nine m inim um w ages
per m ont h. At t he t im e of r esear ch, t he m inim um w age
in Br azil w as R$240.
What r eligion is concer ned, in eight ( 72.7% )
f a m i l i es, a l l m em b er s o f t h e f a m i l y n u cl eu s w er e
Ca t h o l i c; i n o n e ( 9 . 1 % ) , t h e a g e d p e r so n w a s a
N O I T A R E T L
A SUBCATEGORIES
E V I T I S O
P Nº NEGATIVE Nº
n o i t a l e R y l i m a F 8 5 = N . n o s r e p d e g a e h t f o e r a c e k a t o t s e v i t a l e r m o r f n o i t a r o b a ll o
C 7 Worsenedtheagedperson'srelationwithfamilymembers. 11 . s r e b m e m y l i m a f g n o m a n o i t a l e r d e v o r p m
I 12 Increasedtheagedperson'saggressivenesstowardshis . e f i w 5 . t n e m t a e r t t u o b a e d i c e d o t s e v i t a l e r m o r f t r o p p u
S 4 Lackofcollaborationfromrelativestotakecareoftheaged . n o s r e p 4 . s d n e i r f d n a s r o b h g i e n m o r f n o i t a r o b a ll o
C 6 Changedthecompositionofthefamilynucleus. 2 . r e w o p n o i s i c e d s ' e f i w e h t d e s a e r c n
I 1 Chargesduetodecisionmakingabouttreatment. 1 o t n o i t n e t t a e r o m e t a c i d e d o t r e h t a f r i e h t g n i k s a n e r d l i h C . A V C h t i w r e h t o m r i e h t 1 . A V C e h t r e t f a e g a i r r a M 1 . s d n e i r f d n a s r o b h g i e n m o r f g n i c n a t s i D 3 L A T O
T 30 28
Sp ir it ist , t h e w if e Ad v en t ist an d t h e d au g h t er an d
g r an d ch ild r en Cat h olic; in on e f am ily, ( 9 . 1 % ) , t h e
e l d e r l y a n d h i s w i f e w e r e Ca t h o l i c a n d t h e i r
gr andchildr en Ev angelic and, in anot her one ( 9, 1% ) ,
t h e a g e d w o m a n , h e r s o n - i n - l a w a n d t w o
g r a n d d a u g h t e r s w e r e Ca t h o l i c, h e r d a u g h t e r w a s
Spir it ist and one gr anddaught er w as Buddhist .
Descr ipt ion of Changes in Fam ily Relat ions
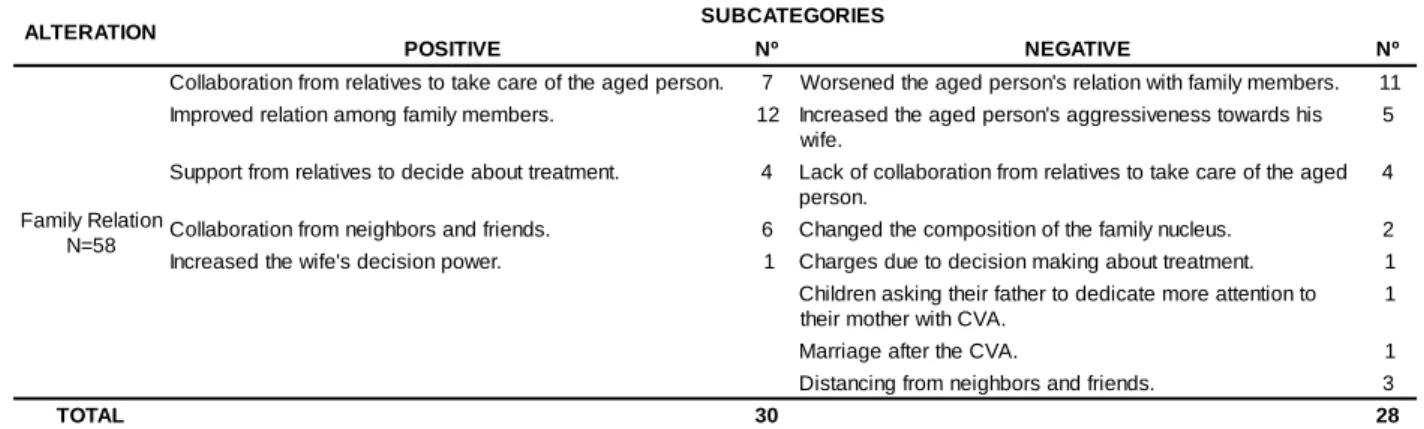
The analy sis of t he consequences r ev ealed a
n u m b e r o f c h a n g e s i n f a m i l y r e l a t i o n s . Th e s e
const it ut ed 13 subcat egor ies, fiv e posit iv e and eight
n eg at iv e, t ot alin g 5 8 ch an g es, 3 0 p osit iv e an d 2 8
n eg at iv e, in accor d an ce w it h t h e f am ily m em b er s’
r epor t s ( Table 1 ) .
Table 1 – Cat egor y of ch an ge in f am ily r elat ion s an d r espect iv e su bcat egor ies, w it h a posit iv e or n egat iv e
r efer ence, ex t r act ed fr om t he r epor t s of r elat iv es of aged per sons diagnosed as CVA - Ribeir ão Pr et o, 2003
DI SCUSSI ON
The 11 elder ly per sons’ aver age age w as 73.4
y ear s and 6 3 . 6 % w er e m en. These dat a ar e sim ilar
t o a st udy( 6) on healt h condit ions am ong per sons aged
60 or older in t he cit y of São Paulo, car r ied out t hr ough
sel f - r ef er r ed a ssessm en t . Th i s r esea r ch o b ser v ed
h ig h er in cid en ce lev els of CVA am on g eld er ly m en
over 75, accom panied by a lar ger am ount of sequelae.
Most m ale v ict im s w er e m ar r ied, an d m ost
fem ale vict im s w idow ed. Am ong t he m en, t he condit ion
of being m arried favors car e deliver y by t heir fam ilies.
I n t e r m s o f e d u c a t i o n , a m a j o r i t y o f
par t icipant s knew how t o r ead and w r it e, follow ed by
t h ose w h o h ad n ot fin ish ed pr im ar y edu cat ion , w it h
f ou r y ear s of st u d y at m ost . Th is is in accor d an ce
w it h t h e Br azilian r ealit y, w h er e m ost eld er ly aliv e
did not have t he oppor t unit y t o lear n how t o r ead and
w r it e( 7 ). Low edu cat ion lev els can con t r ibu t e t o t h e
ap p ear an ce of t h e d isease, as t h is f act , associat ed
w it h socioeconom ic and cult ur al fact or s, can difficult
aw ar eness about healt h car e needs acr oss a per son’s
life, adher ence t o t r eat m ent and t o t he m aint enance
of a h ealt h y lif est y le t h at lim it s t h e ef f ect s of r isk
fact or s( 8 ).
W h a t p r o f essi o n / o ccu p a t i o n i s co n cer n ed ,
81. 8% w er e r et ir ed, w hile t he ot her par t icipant s did
n o t h av e an y o w n i n co m e an d d ep en d ed o n t h ei r
p ar t n er. As a r esu lt of t h is con d it ion , m ost eld er ly
needed help fr om t heir r elat iv es t o com plem ent t heir
low in com e. Th is w as ag g r av at ed ev en m or e w h en
t h e a p p e a r a n c e o f t h e d i s e a s e l e d t o i n c r e a s e d
ex p en ses.
Most p ar t icip an t s ( 9 0 . 9 % ) w er e v ict im s of
ischem ic CVA, and only 9.1% of t he hem or r hagic t ype.
Th i s i s p r o b a b l y d u e t o t h e h i g h l e t h a l i t y o f
h em or r h ag ic CVA( 6 ).
On t he aver age, t he fam ilies consist ed of 4.3
m em ber s. I n m ost of t hem , t w o or m or e gener at ions
3 6 8
households. This fact can creat e t he need for a fam ily
ar r an gem en t t o cope w it h t h e sit u at ion of h av in g a
sick and dependent elder ly at hom e.
We f ou n d t h at m ost f am ilies su r v iv ed on a
m ont hly fam ily incom e of about one and a half t o t w o
m i n i m u m w a g e s , t h a t s o m e m e m b e r s w e r e
u n e m p l o y e d a n d t h a t t h e p a r e n t a f f e ct e d b y t h e
d i s e a s e c o u l d n o t w o r k . H e n c e , s o m e r e l a t i v e s
m en t ion ed t h e lack of r esou r ces t o bu y food, dr u gs
a n d d i sp o sa b l e d i a p e r s, a s w e l l a s t o r e n t ca r e
equ ipm en t , am on g ot h er s.
When all m em ber s of t he fam ily nucleus had
t he sam e r eligion, t his w as m ost ly Cat holic. I n som e
c a s e s , m e m b e r s i n o n e a n d t h e s a m e f a m i l y
m en t i o n ed d i f f er en t r el i g i o n s, i n cl u d i n g Ev an g el i c,
Spir it ist , Buddhist and Advent ist . This m ixt ur e did not
af f ect t h eir m u t u al r elat ion s. Wh en q u est ion ed , all
r elat iv es in dicat ed r espect f or each ot h er ’s r eligion .
Ev an g el i cal s r eg u l ar l y w en t t o ch u r ch , w h i l e m ost
Ca t h o l i c f a m i l y m e m b e r s a t t e n d e d se r v i ce s m o r e
sp or ad ically. We f ou n d t h at t h e d isease r ecov er ed
per son s’ lin k w it h r eligion , in dicat ed as a possibilit y
of hope t o r ecover fr om t he healt h pr oblem s r esult ing
f r om ch r on ic disease.
The analysis of t he consequences of CVA and
t he sit uat ions it pr oduced r ev ealed changes in fam ily
relat ions. The concept of fam ily relat ion is linked w it h
connect ions and/ or co- liv ing am ong fam ily m em ber s
or per sons t hey find significant . I n t his st udy, w e look
at changes in t he dom est ic env ir onm ent of t he aged
per son v ict im of CVA.
Fo r e l d e r l y p e r s o n s , t h e f a m i l y i s
fundam ent ally im por t ant for solidar it y and pr ot ect ion,
as w ell as af f ect iv e r elat ion s per m eat in g t h e f am ily
d y n a m i c s . W h e n t h e d i s e a s e a p p e a r s , b e s i d e s
br eak in g t h e f am ily ’s or gan ic balan ce, in t er f er en ces
occur in ot her lev els of life, m ainly in co- liv ing w it h
close r elat iv es( 9 ). Hen ce, a d isease lik e CVA, w h ich
can pr oduce sequelae in one of t he fam ily m em ber s,
fav or s disor ganizat ion and changes balance and pr
e-est ablished int er act ion pat t er ns. Pr om ot ing har m ony
and under st anding am ong it s m em ber s is par am ount
for t he r eor ganizat ion of t he fam ily sy st em .
For people t o liv e t oget h er, t h er e is a n eed
for an int er per sonal r elat ion am ong fam ily m em ber s,
w it h one under st anding t he ot her. This is not an easy
t a sk , a s i n t er p r et i n g o t h er p er so n s’ b eh a v i o r a n d
a c k n o w l e d g i n g d i f f e r e n c e s s o m e t i m e s l e a d s t o
p r e o ccu p a t i o n s, d i sa g r e e m e n t s a n d d i f f i cu l t i e s i n
r e l a t i o n s( 1 0 ). Th e s a m e a u t h o r a d d s t h a t
c o m m u n i c a t i o n i s a n i m p o r t a n t s t r a t e g y t o
appr oxim at e people, and t hat dialogue is fundam ent al
in fam ily r elat ions.
Th e m ost r elev an t ch an ges f or t h e posit iv e
subcat egor ies r efer t o collabor at ion for car e, im pr oved
r elat ion s am on g f am ily m em ber s, r elat iv es’ su ppor t
in decision processes and collaborat ion from neighbors
an d fr ien ds.
Mo st f a m i l i e s m e n t i o n e d t h a t t h e f a m i l y
car egiv er r eceiv ed bot h infor m al and for m al suppor t
t o h e l p i n ca r e a ct i v i t i e s. W i v e s, d a u g h t e r s a n d
g r an d ch ild r en assu m ed t h e r esp on sib ilit y f or d ir ect
ca r e.
Tw o fam ilies r eceived suppor t at t heir hom es
fr om a hospit al’s hom e visit t eam , w hich guided care
a ct i v i t i e s. Re l a t i v e s d e scr i b e d t h i s e x p e r i e n ce a s
posit iv e, due t o t he fact t hat it m ade car egiv er s feel
m or e secur e t o handle car e sit uat ions.
Th e du t ies im posed by car e f or t h e elder ly
ch an ged f am ily r elat ion s. Th is gav e bot h car egiv er s
and t he aged per sons t he oppor t unit y t o obt ain new
per cept ions of t hem selves and t he ot her s, as t he car e
process im plies a set of act ions t hat involve at t it udes,
feelin gs an d com m it m en t s.
Th e g r ea t er p r o x i m i t y a s a r esu l t o f ca r e
a c t i v i t i e s s t i m u l a t e d i m p r o v e d r e l a t i o n s a m o n g
r e l a t i v e s, i n cl u d i n g t h e a g e d . Fa m i l y 4 ’s m o t h e r
indicat ed t hat m ost childr en m et m or e fr equent ly and,
b esid es t ak in g car e f or t h eir f at h er, t h ey also t ook
car e of each ot h er. Th ey w er e con cer n ed abou t n ot
leaving t he car e r esponsibilit y w it h one single per son
and t he pr esence of affect ion and under st anding w as
clear.
I n 5 4 . 5 % o f f a m i l i es, r el a t i v es st a r t ed t o
dedicat e m or e at t ent ion t o t he elder ly, t hat is, w ives,
i n - l a w s , c h i l d r e n , g r a n d c h i l d r e n a n d g r e a t
g r an d ch ild r en sp en t m or e t im e w it h t h em , t alk in g ,
w a t ch i n g TV a n d a cco m p a n y i n g l ei su r e a ct i v i t i es,
am on g ot h er s. Man if est at ion s of h ar m on iou s f am ily
r elat ions cont r ibut ion t o t he aged per sons’ em ot ional
com for t( 1 1 ).
Th e cogn it iv e an d m ot or deficit s t h at affect
vict im s of CVA br ing about a lar ge- scale redist r ibut ion
o f f a m i l y r o l e s . Th e v i c t i m s ’ d e c i s i o n p o w e r i s
consider ably im pair ed and, oft en, w hat r em ains is t he
illusion t hat t hey ar e st ill m aking decisions. I n fam ily
7, befor e t he disease, t he aged m an w as aut onom ous,
i n sp i t e of al coh ol i sm an d ev en w i t h ou t assu m i n g
f a m i l y r e v e n u e s. Af t e r t h e CVA, d e ci si o n p o w e r
p assed t o t h e w if e, w h o assessed t h e sit u at ion as
p osit iv e, as f am ily or g an izat ion ch an g ed in sev er al
w a y s. Cer ebr ovascular accident in t he aged...
Mar ques S, Rodr igues RAP, Kusum ot a L.
Fam ilies 1 , 5 an d 8 ex p er ien ced sit u at ion s
r elat ed t o t h e r esp on sib ilit y of d ecid in g ab ou t t h e
r ealizat ion of su r g ical p r oced u r es in t h e eld er ly, as
w ell as ab ou t w it h d r aw in g t h e n asog ast r ic cat h et er
a n d t h e st a r t o f o r a l d i e t . W i t h r e sp e ct t o t h e se
p r o c e d u r e s , w e p e r c e i v e d t h e i m p o r t a n c e o f a l l
r el at i v es’ p ar t i ci p at i o n i n t h e d eci si o n p r o cess, as
coh esion m ad e t h em f eel m or e secu r e ab ou t t h eir
final at t it ude t ow ar ds int er v ent ion.
Som e par t icipant s m ent ioned collabor at ion by
neighbor s and fr iends, r elat ed t o t r anspor t , secur it y,
com pany for t he elder ly w hen car egiver s w er e absent
and suppor t in em er gency sit uat ions.
I n f a m i l y 3 , t h e d a u g h t e r i n d i c a t e d t h e
fam ily ’s t ight r elat ion w it h t he closes neighbor s, w ho
offered help for som e needs. The elderly w ife in fam ily
5 spent par t of t he day alone at hom e w it h her aged
husband and could also count on neighbor s in case of
em er g en cy.
I t i s n at u r al f o r r el at i v es t o cu l t i v at e an d
in v est in f r ien d sh ip sy st em s, in clu d in g ou t sid e t h e
f am ily. Som e in div idu als con sider f r ien ds as people
w it h w hom t hey develop significant and m or e pr ofound
r elat ions. Co- living w it h t hese per sons can happen in
t h e n ei g h b o r h o o d , w o r k en v i r o n m en t a n d sch o o l ,
a m o n g o t h er so ci a l i n st i t u t i o n s. Th e r el ev a n ce o f
r elat ion s w it h n eigh bor s an d f r ien ds w as ev iden ced
in t er m s of t h eir collabor at ion w it h daily pr oblem s,
m ak in g t h e r elat iv es r esp on sib le f or t h e ag ed f eel
su ppor t ed an d secu r e.
As t o n eg a t i v e su b ca t eg o r i es o f ch a n g es,
t h ese i n cl u d ed w o r se r el a t i o n s b et w een t h e a g ed
p e r s o n a n d r e l a t i v e s , i n c r e a s e d a g g r e s s i v e n e s s
bet w een t he aged and his w ife, lack of collabor at ion
f or car e an d d ist an cin g f r om n eig h b or s d u e t o t h e
elder ly per son s’ bad m ood.
El d er l y p er son s i n f am i l i es 2 an d 7 h ad a
dr inking habit , w hich ser iously im pair ed t heir r elat ion
w it h r elat iv es befor e t he CVA. Alcoholism can dist or t
or dest r oy fam ilies’ self- confidence and self- est eem .
Fam ily m em ber s can isolat e an alcoholic r elat iv e and
k eep only lim it ed cont act s w it h him / her( 12).
I n f a m i l y 2 , t h e w i f e t o l d t h a t h e r a g e d
h u sban d h ad a con f lict in g r elat ion w it h h er an d h is
childr en, ev en befor e t he CVA. She also added t hat ,
at t he t im e of t he int er view , he had been even m or e
ag g r essiv e an d t h at , d u r in g car e, h e in su lt ed h er,
spit t ed on her face and had alr eady t r ied t o physically
at t ack h er. Sh e at t r ibu t ed t h is beh av ior t o t h e f act
t hat “ he is nat urally bad- t em per ed”, did not accept t o
depen d on h er f or body car e an d f in an cial m at t er s,
am ong ot her for m s of dependence. The sam e per son
a l so h a d a co n f l i ct i n g r e l a t i o n w i t h h i s ch i l d r e n ,
gr an dch ildr en , in - law s an d br ot h er s.
The w ife in fam ily 7 m ent ioned t hat her aged
h u sb an d o f f en d ed b o t h h er sel f an d h er d au g h t er s
p s y c h o l o g i c a l l y a n d p h y s i c a l l y. Th i s v i o l e n c e o r
m i st r eat m en t i s a com p l ex p u b l i c h eal t h p r ob l em ,
or iginat ed in t he int er act ion am ong biological, social,
cult ur al, econom ic and polit ical fact or s( 13). The oldest
daught er felt r evolt ed by her fat her ’s violent at t it udes
t ow ar ds t he fam ily in t he past , and t his fact int er fer ed
in daily car e. This r esponsibilit y w as assum ed by t he
m ot her, w ho also w ent out t o w or k t o sust ain t he fam ily.
Th e co n f l i ct i n g r e l a t i o n s d e scr i b e d a b o v e
dat ed back t o sit uat ions befor e t he occur r ence of t he
CVA, how ever, w it h a considerable incr ease aft er t he
disease. The w ife in fam ily 2 indicat ed t hat neighbors
and fr iends no longer v isit ed t heir house due t o t he
aged per son ’s bad m ood an d aggr essive beh av ior.
The lack of collabor at ion for car e can pr oduce
conflict s am ong relat ives, as t he desire t o help cannot
solely depend on one single per son.
I n fam ily 3, t he daught er t old about conflict s
b e t w e e n b r o t h e r s d u e t o t h e d i v i s i o n o f c a r e
r espon sibilit ies. I n an at t em pt t o t r an sf er t h e aged
w om en t o h er sist er ’s h om e, h er br ot h er - in - law did
not accept . As a r esult , t he aged w om an r et ur ned t o
h er or ig in al h om e an d car eg iv er. I n t h is case, on e
sist er could not decr ease t he ot her ’s over load due t o
h er h u sb an d ’s op p osit ion t o t ak e t h e ag ed w om an
int o his hom e.
Fa m i l y r e p o r t s r e v e a l e d v a r i o u s o t h e r
im pedim ent s t o collabor at ion. The m ost com m on ones
w er e ext er nal w or k, obligat ions t ow ar ds husband and
childr en and angr iness and gr udges against t he aged
p er so n .
Fam ily relat ions are relevant in t erm s of love,
af f ect ion , r espect an d v alu es, as t h ey con t r ibu t e t o
healt hy aging( 14). These aut hors also highlight t hat , in
case of healt h pr oblem s, t he r elat ion w it h significant
p er son s an d t h eir co- liv in g can h elp t h e eld er ly t o
cope w it h and adapt t o t he inst abilit ies of t he disease.
Dev elop in g an d look in g f or f r ien d sh ip s an d
cl ose r el at i on s i s essen t i al w h en p eop l e n eed on e
anot her. I nt er dependent and com plem ent ar y r elat ions,
char act er ized by m ut ual help w hen needed, gener at e
t h e su p p o r t o f secu r i t y a n d co m f o r t , r el ev a n t f o r
3 7 0
Disorganizat ion, due t o t he lack of cont r ol on
t h e s i t u a t i o n p r o d u c e d b y c h r o n i c d i s e a s e a n d
ag g r av at ed by t h e f am ily ’s ow n lif e h ist or y, m ak es
relat ives look for reorganizat ion t o achieve a balance,
using st rat egies t hat can guarant ee coping w it h t hese
si t u a t i o n s, w i t h a v i ew t o co n t i n u i n g t h e f a m i l y ’ s
t r aj ect or y.
Nu r sin g p r of ession als n eed t o ack n ow led g e
an d v alu e each f am ily ’s ef f or t s an d pot en t ial, u sin g
w hat is posit ive t o give t he required support . Fam ilies
m ust be encour aged and suppor t ed t o r eor ganize and
balance t he fam ily syst em by looking int o it s ow n daily
dem ands and challenges. This at t it ude can st r engt hen
and enable t he fam ily t o at t end t o t he aged per son’s
car e needs, as w ell as t o adm inist er t he sit uat ion all
r elat iv es ar e g oin g t h r ou g h w it h less su f f er in g an d
d isag r eem en t s.
FI NAL CONSI DERATI ONS
Cer ebr ov ascular accident can cause a r ange
o f n e u r o l o g i c a l d e f i c i t s t h a t p r o d u c e s e q u e l a e ,
af f ect in g t h e v ict im s’ self - car e per f or m an ce an d lif e
m a i n t e n a n c e . B e s i d e s p h y s i c a l c o n s e q u e n c e s ,
p s y c h o l o g i c a l a n d s o c i a l f u n c t i o n s a l s o c h a n g e ,
e x p o s i n g f a m i l y s t r u c t u r e , d e v e l o p m e n t a n d
f u n ct ion in g.
I n t h e f a m i l y s p h e r e , f a m i l y r e p o r t s
d em o n st r at ed ch an g es r esu l t i n g f r o m t h e d i sease
p r o c e s s , a s s o c i a t e d w i t h l o s s e s d u e t o a g i n g ,
at t r i b u t i n g p o si t i v e o r n eg at i v e r ef er en ces. Th ese
alt er at ions influenced and w er e influenced by fam ily
r elat ions and t he fam ilies’ cont ex t it self.
A g e d p e r s o n s ’ l i v i n g a n d c o - l i v i n g i n
con t in u ou s car e pr ocesses is per m eat ed by f eelin gs
of t ir edness, st r ess, ex haust ion, but som et im es also
b y w elcom in g , af f ect ion an d t en d er n ess. Car e an d
t ir edness as a r esult of t he car e pr ocess ar e hum an
condit ions t hat r equir e r eflect ion and suppor t t o t he
car e- g iv in g f am ily.
Ch a n g e s e m e r g e d f r o m t h e s i t u a t i o n s
pr oduced by t he chr onic disease and aggr av at ed by
t h e f am ily ’s ow n lif e h ist or y. Th ey r eceiv ed posit iv e
or n eg at iv e con n ot at ion s f r om t h e p er sp ect iv es of
r elat ives w ho w ere going t hr ough t he disease pr ocess
of aged per sons w ho w er e vict im s of CVA, pr esent ing
sequelae and decr eased funct ional capacit y and t hus
n e e d e d h e l p t o p e r f o r m b a s i c a n d i n s t r u m e n t a l
act iv it ies of daily liv ing.
Fam ily dy n am ics can in flu en ce on e or m or e
of it s m em bers posit ive or negat ively. Mult idisciplinary
t eam s can fav or fam ilies’ r elat ions and adapt at ion t o
t h e d em an d s. Nu r ses w h o d o n ot k n ow t h e f am ily
st r uct ur e should not v alue it s difficult ies w it h a v iew
t o solv ing pr oblem s.
REFERENCES
1 . Kl i n g C, Waszy n sk i CM. To p i cs i n n eu r o l o g i c car e. I n : M o l o n y S L, W a s z y n s k i CM , Ly d e r CH , o r g a n i z e r s . Ge r o n t o l o g i ca l n u r si n g : a n a d v a n ce d p r a ct i ce a p p r o a ch . St am for d ( CT) : Applet on & Lange; 1999. p. 311- 87. 2 . Mat ur ana HR. Biology of Language: The Epist em ology of Realit y. I n : Miller G, Len n eber g E, edit or s. Psy ch ology an d Biology of Language and Thought . New Yor k ( NY) : Academ ic Pr e ss; 1 9 7 8 .
3 . Wr igh t LM, Leah ey JM. En f er m eir as e f am ílias: u m gu ia p ar a av aliação e in t er v en ção n a f am ília. 3 ª ed . São Pau lo ( SP) : Roca; 2 0 0 2 .
4. Flanagan JC. A t écnica do incident e cr ít ico. Ar q Br as Psicol Ap l 1 9 7 3 ab r il- j u n h o; 2 5 ( 2 ) : 9 9 - 1 4 1 .
5 . Mi n a y o MCS . O d e s a f i o d o c o n h e c i m e n t o : p e s q u i s a q u a l i t a t i v a em sa ú d e. 7 ª ed . Sã o Pa u l o ( SP) : HUCI TEC-A B RTEC-A S CO; 2 0 0 0 .
6. Lebr ão ML, Laur ent i R. Condições de saúde. I n: Lebr ão ML, D u a r t e YAO, o r g a n i za d o r es. SABE - Sa ú d e, Bem - est a r e Envelhecim ent o - O pr oj et o Sabe no m unicípio de São Paulo: u m a a b o r d a g e m i n i ci a l . Br a síl i a ( D F) : Or g a n i za çã o Pa n -Am er ican a da Saú de; 2 0 0 3 . p. 7 5 - 8 9 .
7 . Ro d r i g u e s RAP. At i v i d a d e Ed u ca t i v a d a En f e r m a g e m Ger i át r i ca: co n sci en t i zação p ar a o au t o cu i d ad o d e i d o sas que t iver am queda. [ disser t ação] . Ribeir ão Pr et o ( SP) : Escola de Enfer m agem de Ribeir ão Pr et o/ USP; 1 9 9 3 .
8. Per lini NMOG. Cuidar de pessoa incapacit ada por acident e v ascular cer ebr al no dom icílio: o fazer do cuidador fam iliar. [ t ese] São Paulo ( SP) : Escola de Enfer m agem / USP; 2 0 0 0 . 9 . Pa u l a A A D , Fu r e g a t o A R, S c a t e n a M CM . I n t e r a ç ã o e n f e r m e i r o - f a m i l i a r d e p a c i e n t e c o m c o m u n i c a ç ã o p r e j u d i ca d a . Re v La t i n o - a m En f e r m a g e m 2 0 0 0 a g o st o ; 8 ( 4 ) : 4 5 - 5 1 .
1 0 . Alt hoff CR. Delineando um a abor dagem t eór ica sobr e o p r ocesso d e con v iv er em f am ília. I n : Elsen I , Mar con SS, Silva MRS, or ganizador es. O viver em fam ília e sua int er face com a saúde e a doença. Mar ingá ( PR) : Eduem ; 2002. p.25-4 3 .
1 1 . Gon zales TBD, An d r ad e AME, Vea HB. Car act er ización d e las r elacion es f am iliar es d el an cian o. Rev Cu b an a Med Gen I n t eg r 2 0 0 1 ; 1 7 ( 5 ) : 4 1 8 - 2 2 .
12. Kr est an JA, Bepk o C. Pr oblem as de alcoolism o e o ciclo de vida fam iliar I n: Car t er B, Mcgoldr ick M, Aylm er RC, Bepko C, I m ber - Black E, Car t er B, et al. As m udanças no ciclo de v ida fam iliar : u m a est r u t u r a par a a t er apia fam iliar. 2 ª ed. Por t o Aleg r e ( RS) : Ar t es Méd icas; 1 9 9 5 . p . 4 1 5 - 3 4 .
Cer ebr ovascular accident in t he aged... Mar ques S, Rodr igues RAP, Kusum ot a L.
1 3 . Or g a n i za cío n Mu n d i a l d e La Sa l u d . La v i o l e n ci a , u n pr oblem a ubicuo. I nfor m e m undial sobr e la v iolencia y la salud: r esu m en . Wash in gt on ( DC) : OPS; 2 0 0 2 .
1 4 . Oliv eir a TC, Ar au j o TL. Mecan ism os d esen v olv id os p or i d o s o s p a r a e n f r e n t a r a H i p e r t e n s ã o A r t e r i a l . Re v Es c En f er m ag em USP 2 0 0 2 set em b r o; 3 6 ( 3 ) : 2 7 6 - 8 1 .
15. Cr ose R. Por que as m ulher es vivem m ais que os hom ens: e o que eles podem apr ender com elas. Rio de Janeir o ( RJ) : Edit or a Rosa dos Tem pos; 1 9 9 9 .