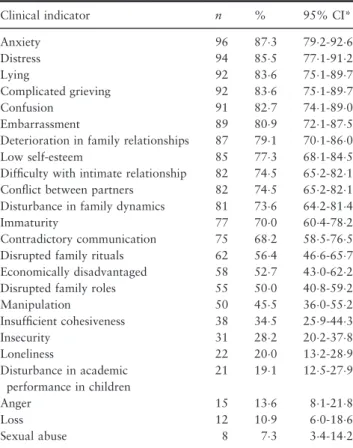
Clinical validation of the nursing diagnosis of dysfunctional family processes related to alcoholism
Texto
Imagem
Documentos relacionados
With respect to the type of support and the nature of the family exchanges, the following were related to high levels of satisfaction with family relations: neither provide
Group 1, constituted of individuals with clinical diagnosis of neurocryptococcosis, with positive results for culture and India Ink test, PCR demonstrated high sensitivity (100%)
pylori EIA presented high sensitivity and specificity when employed for a population in Brazil, permitting the use of the test both to confirm the clinical diagnosis and to
High sensitivity and specificity, rapid identification of the parasite, the possibility of direct application on clinical specimens producing reliable results in a
This study is a clinical validation study based on measures of diagnostic accuracy for clinical indicators of the nursing diagnosis imbalanced nutrition: less than body requirements
The purpose of this study was to analyze the accuracy of NANDA-I clinical indicators of the nursing diagnosis ineffective airway clearance (IAC) in children with acute
The current study aimed to describe the prevalence of high blood pressure – HBP (measured at one sitting, and suggestive of a clinical diagnosis of arterial hypertension), as
After confirming the diagnosis of high blood pressure, the differences in sex, age, and BMI, obesity, tobacco use and alcoholism were analyzed as well as were the values of
