ISSN 0100-879X CLINICAL INVESTIGATION
Texto
Imagem
Documentos relacionados
The goal of PECD is to decompress the cervical nerve root through a direct endoscopic visualization, removing the herniated mass and shrinking the nucleous
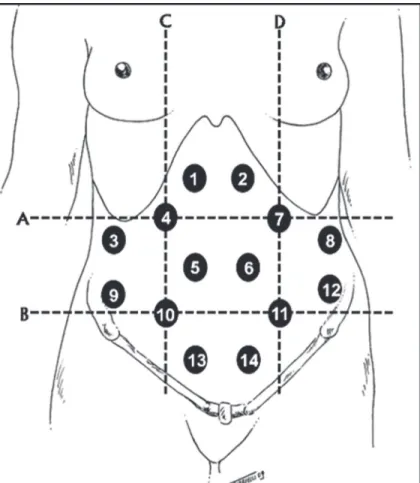
he objective of this study was to verify the reliability of the intra- and inter-examiner evaluation of anteriorization and inclination angles of the head in the anterior and
Universidade Estadual da Paraíba, Campina Grande, 2016. Nas últimas décadas temos vivido uma grande mudança no mercado de trabalho numa visão geral. As micro e pequenas empresas
Material e Método Foram entrevistadas 413 pessoas do Município de Santa Maria, Estado do Rio Grande do Sul, Brasil, sobre o consumo de medicamentos no último mês.. Resultados
The greater feed conversion observed in animals receiving RAC may explain their better performance compared with the higher final weight and better average daily
The probability of attending school four our group of interest in this region increased by 6.5 percentage points after the expansion of the Bolsa Família program in 2007 and
A estratégia algébrica adotada para o acoplamento permite que a matriz de rigidez condensada do meio contínuo seja aplicada ao sistema algébrico do MEF a cada iteração
didático e resolva as listas de exercícios (disponíveis no Classroom) referentes às obras de Carlos Drummond de Andrade, João Guimarães Rosa, Machado de Assis,
