O
RIGINALA
RTICLE Revista Brasileira de FisioterapiaBrazilian version of the Nottingham Sensory
Assessment: validity, agreement and reliability
Versão brasileira da Avaliação Sensorial de Nottingham: validade, concordância e
confiabilidade
Daniela H. F. Lima1, Ana P. Queiroz1, Geovana De Salvo1, Simone M. Yoneyama2, Telma D. Oberg3, Núbia M. F. V. Lima3
Abstract
Objectives: To investigate the inter-rater and intra-rater reliability, construct validity and internal consistency of the Brazilian version of the Nottingham Sensory Assessment for Stroke Patients (NSA). Methods: The instrument was translated into Portuguese from its original in English by a bilingual translator and was then back-translated into English. Twenty-one hemiparetics were evaluated by two examiners using the NSA and the Fugl-Meyer Assessment (FMA) of physical performance. Results: Significant correlation were found between the FMA and the NSA (r=0.752). The NSA showed excellent internal consistency (0.86), and there were acceptable inter- and intra-rater reliability for all items of the NSA, except temperature. Significant ceiling effects were found for the NSA and the FMA. Conclusions: The Brazilian version of the NSA met the criteria for agreement, internal consistency and concurrent validity. It was quick and easy to apply, and it could be used within clinical practice in neuro-rehabilitation outpatient clinics to assess sensory functions following stroke. The significant ceiling effect for the NSA did not limit its use, given that for the same patients, the FMA also showed ceiling effects.
Key words: stroke; disability evaluation; validity tests; sensation; rehabilitation.
Resumo
Objetivo: Verificar a concordância inter e intraexaminador, validade construtiva e consistência interna da versão brasileira do instrumento Nottingham Sensory Assessment para hemiparéticos após acidente vascular encefálico (AVE). Métodos: O instrumento foi traduzido para língua portuguesa com base na sua versão original em Inglês por um tradutor bilíngue e, posteriormente, revertido para a língua inglesa. Vinte e um hemiparéticos foram avaliados por dois examinadores pela Avaliação Sensorial de Nottingham para pacientes pós-AVE (ASN) e pelo Protocolo de Desempenho Físico de Fugl-Meyer (FM). Resultados: Foi encontrada correlação entre os instrumentos FM e ASN (0,752); excelente consistência interna da ASN (0,86); excelentes coeficientes de concordância interexaminador e intraexaminador para todos os itens da ASN, exceto temperatura e efeito teto significativo para ASN e FM. Conclusão: A versão brasileira da Nottingham Sensory Assessment cumpriu os critérios de concordância, consistência interna e validade concorrente, sendo um instrumento de rápida e fácil aplicação, podendo ser utilizada nos ambulatórios de neuroreabilitação para avaliar a função sensorial pós-AVE. O efeito teto significativo da ASN não limita seu uso, tendo em vista que, para os mesmos pacientes, o Protocolo de Fugl-Meyer também revelou efeito teto.
Palavras-chave: acidente cerebral vascular; avaliação da deficiência; testes de validade; sensação; reabilitação.
Received: 05/05/2009 – Revised: 15/07/2009 – Accepted: 06/08/2009
1 Postgraduate program in Adult Neurological Physical Therapy, Universidade Estadual de Campinas (UNICAMP), Campinas (SP), Brazil.
2 Department of Physical Therapy, Phonoaudiology and Occupational Therapy of the Medical School of the Universidade de São Paulo (USP), São Paulo (SP), Brazil.
3 Service of Physical Therapy and Occupational Therapy of the Clinical Hospital of the UNICAMP and Department of Neurology of the Medical Sciences’ School, UNICAMP, Campinas (SP), Brazil.
Correspondence to: Daniela Helena da Fonseca Lima, Rua Adelaide dos Santos Barreira, 312, Jd Chapadão, Campinas (SP), CEP: 13070-007, email: [email protected]
Introduction
Sensory impairments afect about 60% of patients who have sufered a cerebrovascular disease (CVD) 1. According to Sterzi et al.2, the somatic sensations are afected in 37% of patients with a injury in the right hemisphere and in 25% of patients with a injury in the left hemisphere. he most evident consequences of the somato-sensory impairments are alterations in tactile rec-ognition and in the manipulation of objects, the threat of burns or other injuries in the limb with loss of sensory perception, mo-tor changes of the afected limb, deicits to control the level of strength during hand grip and gait impairments2-7.
he motor cortex is related to sensory processing during the performance of motor tasks1. Two of the main functions of the cutaneous sensations of the hand are to obtain information regarding the environment during exploratory tasks and to provide the feedback for the precision abilities during the tasks of grip and object manipulation1,6,8-10. Sensory impairments in the lower limb can cause losses in gait, since it leads to a reduc-tion of the swing phase, gait velocity and step symmetry11. he sensory functions are recognized as a precursor of the recovery of movement and functional activity3,12.
It is known that somato-sensory impairments have a signiicant inluence on daily activities. Patients with sen-sory and motor losses have poorer prognostics than patients with exclusive motor impairment, since the somato-sensory impairments have a negative efect on functional perfor-mance of hemiplegic patients and prolongs the rehabilita-tion treatment3,10. Sommerield and Von Arbin13 evaluated the pain and tactile sensitivity of hemiparetic subjects in the acute phase and observed 40% of them had sensory dysfunc-tions, concluding that normal sensory functions were related to high functional performance and to a lower length of per-manence in the hospital.
Sensory assessments are done by 80% of health profes-sionals3, however, much research consider it diicult to be de-veloped and tiring, especially because it is commonly performed after all of the motor tests. Sensory assessments in hemiparetic have been performed through somato-sensory evoked poten-tials14 or functional scales. Considering the last ones, therapists should consider the validity and reliability of the instruments used in their clinical exams, since there are non-standardized forms of assessing sensitivity, but many of them do not provide and adequate information to assess diagnostics or to monitor the gains resulting from sensory rehabilitation 1,10,11,15.
According Lyden and Hantson16, the characteristics of an ideal instrument for the evaluation after CVD consist of easy and quick application; simplicity and a lack of ambiguity; con-current validity; reliability; to demonstrate and appropriate in-ternal consistency and reproducibility inter- and intra-raters;
to be independent of the inluences of age, sex, language, social class, profession or educational levels of the patient and to demonstrate ranges of scores which avoid diiculties to indi-cate minimal clinical changes.
In the literature, the use of clinical instruments for sensory assessment is poorly documented, and there were not found, in the literature, research, nor validated instruments exclusive for the sensory assessment of this population in Brazil. Carey, Oke e Matyas5 created the test of limb position sense. hey con-irmed its reliability and clinical usefulness in the proprioceptive assessment of hemiparetic wrists. Later, Dannenbaum et al.10 created two evaluations of the sensory functions of the hand for this population. In 2002, the instrument Rivermead Assessment of Somato-sensory Performance was created to measure the sen-sory functions of hemiparetic patients and it demonstrated good intra- and inter-rater reliability coeicients, however, it required commercially registered equipment for its administration1.
In 2006, the instrument Hand Active Sensation Test was elaborated. It evaluates the identiication of weights and textures by hemiparetic subjects, however it is limited to the hand evaluation and does not involve thermal sensations and stereognosis17. he subscale of sensitivity of the Fugl-Meyer As-sessment (FMA) of physical performance involves extereocep-tion and proprocepextereocep-tion of the upper and lower limbs and has high inter-rater reliability and internal consistency, neverthe-less it has shown a high ceiling efect and a poor to moderate reliability for the item extereoception18.
he Nottingham Sensory Assessment (NSA) was created
in England, in 1991, by Lincoln et al.19, and aimed to identify the sensory deicits present after CVD and to monitor their recovery. It is related to the evaluation of the protophatic and epicritic sensory modalities, and has shown good intra-rater reliability, but had poor inter-rater reliability after the assess-ment of hemiparetic subjects. Considering this, in 1998, the instrument were items reduced and went through a new eval-uation of its reliability, in its country of origin, and there was found acceptable levels of inter-rater reliability20. he NSA dif-fers from the other types of sensory assessments since it tests all body segments and does not require high cost equipment for its administration.
his present study has the purpose of translating the
Nottingham Sensory Assessment (NSA) scale, and to verify its
reliability, concordance, internal consistency and concurrent validity in hemiparetic patients after CVD occurrence.
Methods
Hospital of the Universidade Estadual de Campinas (UNI-CAMP). his research was approved by the Ethics Committee of Research of the Medical Sciences Scholl of the UNICAMP (number 996/2007). he study of validation of the NSA had been permitted by the authors of the instrument20, through its concession and of its manual, while maintaining the authors rights.
Participants
Patients were invited with hemiparesis secondary to CVD from a list of patients treated at the Outpatients Clinic of Physi-cal herapy and Occupational herapy. he inclusion criteria a-dopted were ages up to 18 years-old; of both sexes; and unilateral CVD ischemic or hemorrhagic CVD with an onset of up to six months. here were included literate patients. Patients excluded from this study included subjects with sensitive impairments secondary to other diseases; those with speech impairments and/or unable to understand simple instructions; with severe cognitive disturbances; with cerebellar CVD and those with Diabetes Mellitus and/or peripheral neuropathies. he patients or their relatives signed a free informed consent form.
Measurement Instruments
he NSA has four subscales and 20 items (in annex). he subscales were tactile sensation, proprioception, stereognosis and two-point discrimination. he NSA identiied the sensory impairments in the face, trunk, shoulder, elbow, wrist, hand, knee, ankle and foot. Each item of the subscale tactile sensation (light touch, pressure, pinprick, temperature, tactile location on both sides of the body and bilateral simultaneous touch) may be scored from 0 to 2, which represented tactile anesthesia and normal tactile sensation, respectively. he total scoring for the non-afected side of the body ranged from 0 to 90 and for the afected one ranged from 0 to 108.
he subscale for proprioception of the NSA evaluated the movement performance, its direction and the joint position of segments only on the afected side of the body. Each item was scored from 0 (absence of proprioception) and 3 (normal pro-prioception), with a total score that ranged from 0 to 21. he segments of the face, trunk and foot were not assessed through this subscale according to the original version.
he subscale stereognosis of the NSA observes the recogni-tion of 11 objects by the afected side of the body, being scored from 0 (astereognosis) to 2 (normal stereognosis) and with a total score ranging from 0 to 22. he objects required by this subscale are used in the activities of daily living.
he subscale two-point discrimination was tested in the index inger and thenar region, and each part received a score
from 0 (absence of discriminative touch) to 2 (normal func-tion), with a total score ranging from 0 to 4.
In the cases in which were impossible to test any segment, it was given a punctuation from 4 to 10 for the subscales: (4) unable to detect pressure, (5) physical reasons, for example, motor disability which impairs tactile location, (6) unable to assess due to the vestment, (7) communication impairments, (8) cognitive problems, (9) pain or increased tone, (10) drowsi-ness or impaired concentration 7.
he Fulg-Meyer21 measures the sensory motor recovery in hemiparesis through the subscales: motor function on upper extremity, lower extremity, passive mobility, pain, sensitivity and balance. Each item is pointed from 0 to 2, and, the lower the punctuation, the higher the sensory motor impairment of the patient. his is an instrument validated internationally, translated for the Portuguese language and it has shown high reliability coeicients in Brazilian hemiparetic21. he subscale sensitivity of the FMA protocol involves extereoception (light touch in forearm, hand palm, thigh and foot sole) and prop-rioception (joints from the upper and lower limbs) and its score ranges from 0 to 8 for extereoception and from 0 to 16 for proprioception. he patients were evaluated through the mo-tor and sensitivity subscales of the FMA in order to categorize their sensory motor impairment.
Instrument translation
he NSA and its manual were translated for the Portuguese language based in its original version in English by a bilingual translator and posteriorly reversed for the English by a second translator. his last translator compared the original version to the English version resultant from the back translation, corrected the conlicting interpretations and performed the cultural adaptation with the assistance of a physical therapist experienced in neurological rehabilitation22.
Material
According to the exigencies from the NSA, there shall be used for the assessment of the tactile sensation: cotton ball, monoilament (green color), two test tubes containing hot or cold water and talcum. To measure stereognosis it shall be used: coins of R$ 0,01, 0,10 and 1,00, ballpoint pen, pencil, comb, scissors, sponge, cloth, a tea-cup and a cup, and, for the test of two-point discrimination, a compass is used.
Procedure
he examiners were professionals of physical therapy whom have done, separately, the theoretic-practical training with the
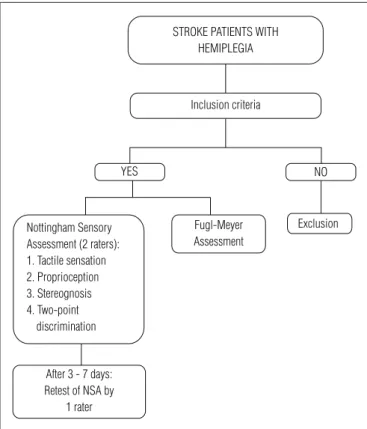
purpose of standardization of the criteria from NSA using the proper manual and listening to seminars developed by an experi-enced physical therapist whom kept contact with the researcher creator of the instrument. Posteriorly, the NSA was administered to three hemiparetic who did not take place of this research’s sample. he patients from the sample were assessed by two ex-aminers, simultaneously, and one did not have asses to the other’s evaluation. A re-test was performed by the examiner 2 after a pe-riod of 3 to 7 days. Figure 1 exhibits the procedure of the study.
he order of application of the NSA was: tactile sensation, stereognosis, proprioception and two-point discrimination. During the evaluation, the patients were asked to use a blind-fold and they could take it out between the tests in case of discomfort. he tactile sensation was examined in both sides of the body, in a variable order. Patients were evaluated with the minimum vestment, preferably wearing a short, when al-lowed by them. Orthosis and elastic stokings were removed during the evaluation. A third examiner administered the FMA protocol in the irst day of evaluation. Patients were evaluated in the Outpatient Clinic of Physical herapy and Occupational herapy in the evening.
Statistical analysis
he descriptive analysis of the numerical and categorical vari-ables of the sample was done. here were calculated the ceiling and loor efects of the subscales of the NSA and of the subscale sensitivity of the FMA protocol – the percentage of the scores which are grouped around the higher and lower punctuations, respectively. Values higher than 20% are considered signiicant. he existence of high ceiling efect indicates a limited capacity of an instrument to discriminate between individuals23.
he level of reliability of an instrument can be obtained measuring the concordance between the results originated from diferent examiners in their applications to the same patients24. he concordance inter and intra-raters (retest) was veriied for the domains of the NSA and in its score in the af-fected side of the body by the Intraclass Correlation Coeicient (ICC): ICC<0,40 – weak concordance, ICC or 0,4-0,75- moderate concordance and ICC>0,75 – strong concordance25. he Bland-Altman analysis was performed through graphics of the sum of the four subscales of the NSA, whose objective is to evaluate the level of concordance inter and intra-rater, considering the diferences from the scores and their means26.
he internal consistency was assessed through the Cron-bach’s Alpha, and values above 0,70 indicate high internal con-sistency27. he correlation item-total of the NSA was executed, being the score above 0,4 considered satisfactory28. he correla-tion between the measuring instruments was performed by the Pearson’s Correlation Coeicient (r). he level of signiicance
adopted for the analysis was of 5%. It was used the statistical program SPSS 15.0 for Windows.
Results
Demographic data and the categorization of the sensory and motor impairments are summarized on Table 1. Partici-pated in this study 21 hemiparetic patients whose mean age
sensory-motor (n=21).
Variables Mean±SD [min; max]
Age (years) 49.47±13.64 [21;78] Gender (F/M) 8 (38.1%) / 13 (61.9%) Type of stroke (H/I) 4 (19%) / 17 (81%) Time since lesion (months) 40.23±32.35 [6;116] FMA – motor scale 54.09±19.21 [24;88] FMA – sensory scale 16.23±5.43 [8;24] Exteroception 5.14±1.68 [3;8] Proprioception 11.28±3.82 [4;16] Nottingham Sensory Assessment
Tactile sensation (non-affected side) 90 Tactile sensation (affected side) 98.61±12.5 [59;108] Proprioception 14.95±3.89 [8;21] Stereognosis 10.85±10.27 [0;22] Two-point discrimination 1.28±1.45 [0;4]
Table 1. Demographic data and impairment levels (n=21).
F=female; M=male; H=hemorrhagic; I=ischemic; FMA=Fulg-Meyer Assessment.
Figure 1. Flow chart of the study.
Exclusion Fugl-Meyer
Assessment Nottingham Sensory
Assessment (2 raters): 1. Tactile sensation 2. Proprioception 3. Stereognosis 4. Two-point
discrimination
After 3 - 7 days: Retest of NSA by
1 rater
STROKE PATIENTS WITH HEMIPLEGIA
YES NO
was of 49.47 (±13.64), being one of them older than 60 years. he level of motor and sensory recovery corresponds to 54% and 67% of the maximal function, respectively, by the FMA pro-tocol. Considering the scores from the nine body points form the NSA, the patients reached 91.3% of the score for tactile sen-sation, 71% of proprioception, 49.3% of stereognosis and 32% of two-point discrimination. here were not found tactile sensory disturbances in the body side contralateral to the hemiparesis. None patient obtained maximal score in all the subscales from the NSA.
A ceiling efect of 66% was found for the subscale tactile sensation of the NSA, of 38% for the stereognosis of the NSA and of 28% for the subscale sensitivity of the FMA protocol; a loor efect of 42% for the subscale two-point discrimination of the NSA and absence of ceiling/loor efects for the subscale proprioception of the NSA.
here was found a correlation between the subscale sensitiv-ity of the FMA and the total score of the NSA (r=0.708, p<0.001). here was not found a correlation between the subscales from the NSA and the motor subscale of the FMA protocol, as well as there was not found a correlation between the motor and sensory sections of the FMA protocol in this sample (r=-0.035, p=0.882). here was found a high internal consistency for the NSA (0.86). he correlation item-total was satisfactory in 16 items from the NSA (Table 2).
It was observed an excellent inter-rater coeicient of con-cordance for all the items of the NSA (Tables 2 and 3). here
Item ICC Confidence interval (CI)
95% p-values Item-total correlations
Light touch 0.998 0.995;0.999 <0.01 0.79
Pressure 1.000 1.000;1.000 <0.01 0.82
Pinprick 1.000 1.000;1.000 <0.01 0.88
Temperature 0.804 0.578;0.916 <0.01 0.199
Tactile localization 0.890 0.750;0.954 <0.01 0.362
Bilateral touch 1.000 1.000;1.000 <0.01 0.341
Proprioception 0.997 0.994;0.999 <0.01 0.334
One cent coin 1.000 1.000;1.000 <0.01 0.64
Ten cent coin 1.000 1.000;1.000 <0.01 0.64
One real coin 1.000 1.000;1.000 <0.01 0.64
Ballpoint pen 1.000 1.000;1.000 <0.01 0.509
Pencil 1.000 1.000;1.000 <0.01 0.575
Comb 1.000 1.000;1.000 <0.01 0.515
Scissors 0.976 0.941;0.990 <0.01 0.582
Sponge 1.000 1.000;1.000 <0.01 0.64
Face cloth 1.000 1.000;1.000 <0.01 0.599
Cup 1.000 1.000;1.000 <0.01 0.692
Glass 0.974 0.937;0.989 <0.01 0.638
Two-point disc. palm 0.953 0.889;0.981 <0.01 0.431
Two-point disc. fingertips 1.000 1.000;1.000 <0.01 0.616
Table 2. Inter-rater reliability and intra-class correlation coefficients.
n=21; ICC= intraclass correlation coefficient; disc=discrimination.
Item ICC
Confidence interval (CI)
95%
p-values
Light touch 0.901 0.776;0.959 <0.01
Pressure 0.988 0.971;0.995 <0.01
Pinprick 0.907 0.786;0.961 <0.01
Temperature -0.070 -0.479;0.363 <0.622
Tactile localization 0.863 0.693;0.942 <0.01
Bilateral touch Proprioception
0.976 0.933
0.943;0.990 0.843;0.972
<0.01 <0.01
One cent coin 1.000 1.000;1.000 <0.01
Ten cent coin 0.977 0.943;0.990 <0.01
One real coin 1.000 1.000;1.000 <0.01
Ballpoint pen 0.909 0.790;0.962 <0.01
Pencil 0.974 0.937;0.989 <0.01
Comb 0.977 0.944;0.990 <0.01
Scissors 1.000 1.000;1.000 <0.01
Sponge 0.888 0.745;0.953 <0.01
Face cloth 1.000 1.000;1.000 <0.01
Cup 0.975 0.941;0.990 <0.01
Glass 0.949 0.874;0.979 <0.01
Two-point disc. palm 0.855 0.677;0.939 <0.01
Two-point disc. fingertips 1.000 1.000;1.000 <0.01
Table 3. Intra-rater reliability and intra-class correlation coefficients.
n=21; ICC= intraclass correlation coefficient; disc=discrimination.
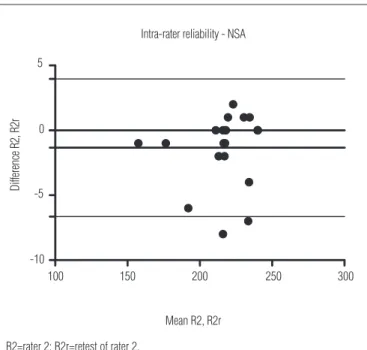
was found a high intra-rater concordance (re-test) in the items of the NSA, except for the item temperature. Figure 2 shows the analysis Bland-Altman for inter-rater concordance and reveals a deviation of -0.33 and a conidence interval of [-1.89; 1.22]. Figure 3 shows the same analysis for concordance between the scores of the examiner 2 (intra-rater or re-test) and there was a deviation of -1.33 and a conidence interval of [-6.64; 3.97]. here was found a good inter and intra-rater concordance, since the majority of the measures pairs was inside the expected limit of concordance.
Discussion
In the present study, the Brazilian version of the NSA has shown a high internal consistence, concurrent validity and high inter and intra-raters concordance levels in all the scale’s items, except for temperature in the intra-rater concordance. Lincoln, Jackson e Adams20 developed the study of concor-dance of this instrument in 27 hemiparetic and found that the items light touch, pressure and the subscale proprioception have shown the best coeicients of concordance, whereas pin-prick and temperature were the less reliable.
he assessment of the thermal sensation through the NSA was reported as unreliable by Lincoln, Jackson e Adams20. hermal sensitivity is poorly explored by the instruments used to assess sensitivity in outpatient settings, possibly due to its lack of standardized resources to provoke hypothermia or hy-perthermia. he temperature of the water was not deined by the authors of the NSA, which may afect the results from the examination. Besides this, the changes on environmental tem-perature may interfere on the thermal sensation of the patient; nevertheless, our patients were assessed in the same period of the day and in the same environment.
In 2006, Stolk-Hornsveld et al.29 performed the second revi-sion of the SNA – eliminating the item temperature, modify-ing the test of pain sensitivity and standardizmodify-ing the tests of proprioception and discriminative touch – and submitted the new version to the test for reliability in 18 patients. he authors found high inter and intra-raters reliability coeicients and took away the subscale discriminative touch of the instru-ment due to its diicult reproduction. his diiculty was not observed in the present study.
he only measuring instrument available and validated to Brazil which measures the sensitivity of hemiparetic is the FMA protocol21. his instrument contains two subscales – extereo-ceptive and proprioextereo-ceptive sensitivity. On the other hand, the NSA involves tactile sensations, proprioception, stereognosis. two-point discrimination, identiication of the sensory deicits in the face, trunk, shoulders, elbows, hand, knees, ankles and
the feet on both sides of the body which is a more complete instrument for the investigation of sensory deicits. he sub-scale of proprioception of the NSA evaluates movement per-formance, its direction and the joint positions (kinesthetic and joint aesthesis), and the FMA protocol, but on the other hand, evaluates only the number of locations of the inal joint posi-tions, in other words, the joint aesthesis.
Knowing that stereognosis is a key component in the recov-ery of the upper limb functions, Gaubert and Mockett30 veriied
Figure 2. Bland-Altman analysis for inter-rater reliability (total score NSA).
Inter-rater reliability - NSA
100 150 200 250 300 -4
-2 0 2
Mean R1, R2
D
iff
er
en
ce
R
1,
R
2
R1=rater 1; R2=rater 2.
Figure 3. Bland-Altman analysis for intra-rater reliability (total score NSA).
Intra-rater reliability - NSA
100 150 200 250 300 -10
-5 0 5
Mean R2, R2r
D
iff
er
en
ce
R
2,
R
2r
the inter-rater reliability of the subscale of stereognosis of the NSA in 20 patients after CVD in the acute phase, and veriied that the subscale had a moderate to high reliability and could be used as a measure for monitoring the evolution of the pa-tients who sufered CVD,, thus reinforcing the present indings. However, there was found a diiculty to assess stereognosis in patients with distal spasticity and impaired hand grip, and it was necessary to position and to move the object in the paretic hand. Some patients confounded the coins’ sizes, especially between the R$ 0,01 e 0,10, as well as named the cloth of the towel.
Although the stereognosis subscale allowed the reference of items similar to those tested, for example, a cloth may be identi-ied as a silk or a face towel, Gaubert and Mockett30 reported that this confusion should be assessed by the inclusion of an interme-diate score on this subscale with a level of score two,. his should be chosen when the patient indicated the names of objects with the characteristics similar to the object being evaluated and the score of three would be designated to its normal function.
he light touch and proprioception are the sensory modali-ties most commonly tested by therapists31. Connell, Lincoln and Radford32 reported that stereognosis and the propriocep-tion are mostly impaired than the tactile sensapropriocep-tions in the hemiparetic patients evaluated through the SNA. heir data was conirmed by the present indings, however, the most im-portant deicits occurred in the two-point discrimination. he authors found that 17% of patients with sensory disturbances were on the side of the body corresponding to the side of the brain injury, however, there were not found sensitive altera-tions on this side of the body in the present study.
For the assessment of tactile locations, it is necessary to use the contralateral limb to indicate the points of stimuli of the sensory test. In case of patients with signiicant spasticity or paresis of upper limb, they were evaluated with the score of ive and, when the patient had aphasia or disarticulate speech, the score of seven was given. he NSA does not ofer alterna-tive strategies, such as verbal indications of the examined segments, in the case of motor impairments, which afect the tactile locations.
he ceiling efects found on the subscales of tactile sensitiv-ity and stereognosis and the loor efect of the subscale of the two-point discriminations, seem to be limiting factors for the use of the instrument. However, there was also found a ceiling efect for the subscale sensitivity of the FMA protocol, as already documented in a previous study18. he signiicant ceiling efect of the NSA subscales may have happened due to the fact that the sample was composed by chronic hemiparetics with mainly motor deicits, which did not allow the conirmation of the NSA limitations in discriminating deicits of these patients.
Among the limitations of this study, it was also observed the absence of assessment of vibratory sensitivity, the small amount of patients and the diiculty to measure the sensory deicits in patients with severe disturbances of speech, lan-guage or cognitions. his sample, with only one patient over 60 years old, reduced the possibility of the interference of the signs aging, such as the deterioration of the vibratory, tactile and pain sensitivity and the reduction of the velocity of con-duction from the peripheral nerves33, which could interfere in the results from the instrument.
he NSA were afected by adaptations concerning the ma-terial used, since only Real coins were used and a single test tube with cold water to assess their thermal sensitivity. he NSA was administered by the examiners in approximately 20 mins., which showed its eiciency for the assessment of sen-sory disturbances of hemiparetic subjects. he length of appli-cation of the FMA protocol was of 20 mins. In addition to the provision of a determined pattern to identify their deicits, the SNA was an inexpensive and easy application procedure. he low cost of the material requested by the SNA favored its use in outpatient clinics for neurological rehabilitation. It is suggested to perform the reliability examination with a greater sample of hemiparetic subjects in the acute and sub-acute phases after the CVD, to establish the validity and temporal stability of its subscales.
he use of validated and reliable measurement instruments is extremely relevant for clinical practice, since it allows the deinition of the sensory proiles and the creation of protocols of sensory rehabilitation during diferent stages of recovery after the CVD.
Conclusions
he Brazilian version of the Nottingham Sensory Assessment has shown excellent intra- and inter-rater coeicients of con-cordance for all the items, except for the item of temperature. here was also found a high level of internal consistency and conirmed the concurrent validity of the instrument. he NSA is an instrument that is rapid and easy to administer, and it can be used in clinical practice for services of neurological rehabilitation, to assess the tactile sensations, proprioception, stereognosis and two-point discrimination in hemiparetic subjects after CVD. he signiicant ceiling efects of the NSA does not limit its use, considering that, for the same patients, the FMA protocol has also revealed ceiling efects. he SNA and its application manual are available by e-mail: nubia@fcm. unicamp.br.
1. Winward CE, Halligan PW, Wade DT. The rivermead assessment of somatosensory performance (RASP): standardization and reliability data. Clin Rehabil. 2002;16(5):523-33.
2. Sterzi R, Bottini G, Celani MG, Righetti E, Lamassa M, Ricci S, et al. Hemianopia, hemianesthesia and hemiplegia after right and left hemisphere damage. A hemispheric difference. J Neurol Neurosurg Psychiatry. 1993;56(3):308-10.
3. Winward CE, Halligan PW, Wade DT. Current practice and clinical relevance of somatosensory assessment after stroke. Clin Rehabil. 1999;13(1):48-55.
4. Carey LM. Somatosensory loss after stroke. Critical Reviews in Physical & Rehabilitation Medicine. 1995;7:51-91.
5. Carey LM, Oke LE, Matyas TA. Impaired limb position sense after stroke: a quantitative test for clinical use. Arch Phys Med Rehabil. 1996;77(12):1271-8.
6. Smania N, Montagnana B, Faccioli S, Fiaschi A, Aglioti SM. Rehabilitation of somatic sensation and related deficit of motor control in patients with pure sensory stroke. Arch Phys Med Rehabil. 2003;84(11):1692-702.
7. Connell LA. Sensory impairment and recovery after stroke [tese na internet]. Nottingham: Universidade de Nottingham; 2007 [acesso em 17/08-/2007]. Disponível em http://etheses.nottingham.ac.uk/247/1/PHD_final.pdf.
8. Wagner JM, Lang CE, Sahrmann SA, Hu Q, Bastian AJ, Edwards DF, et al. Relationships between sensorimotor impairments and reaching deficits in acute hemiparesis. Neurorehabil Neural Repair. 2006;20(3):406-16.
9. Nudo RJ, Friel KM, Delia SW. Role of sensory deficits in motor impairments after injury to primary motor cortex. Neuropharmacology. 2000;39(5): 733-42.
10. Dannenbaum RM, Michaelsen SM, Desrosiers J, Levin MF. Development and validation of two new sensory tests of the hand for patients with stroke. Clin Rehabil. 2002;16(6):630-9.
11. Lynch EA, Hillier SL, Stiller K, Campanella RR, Fisher PH. Sensory retraining of the lower limb after acute stroke: a randomized controlled pilot trial. Arch Phys Med Rehabil. 2007;88(9):1101-7.
12. Tyson SF, Hanley M, Chillala J, Selley AB, Tallis RC. Sensory loss in hospital-admitted people with stroke: characteristics, associated factors, and relationship with function. Neurorehabil Neural Repair. 2008;22(2):166-72.
13. Sommerfeld DK, von Arbin MH. The impact of somatosensory function on activity performance and length of hospital stay in geriatric patients with stroke. Clin Rehabil. 2004;18(2):149-55.
14. Julkunen L, Tenovuo O, Jääskeläinen SK, Hämäläinen H. Recovery of somatosensory deficits in acute stroke. Acta Neurol Scand. 2005;111(6): 366-72.
15. Sullivan JE, Hedman LD. Sensory dysfunction following stroke: incidence, significance, examination and intervention. Top Stroke Rehabil. 2008;15(3):200-17.
16. Lyden PD, Hantson L. Assessment scales for the evaluation of stroke patients. J Stroke Cerebrovasc Dis. 1998;7(2):113-27.
17. Williams PS, Basso DM, Case-Smith J, Nichols-Larsen DS. Development of the hand active sensation test: reliability and validity. Arch Phys Med Rehabil. 2006;87(11):1471-7.
18. Lin JH, Hsueh IP, Sheu CF, Hsieh CL. Psychometric properties of the sensory scale of the Fugl-Meyer ssessment in stroke patients. Clin Rehabil. 2004;18(4):391-7.
19. Lincoln NB, Crow JL, Jackson JM, Waters GR, Adams SA, Hodgson P. The unreliability of sensory assessments. Clin Rehabil. 1991;5(4):273-82.
20. Lincoln NB, Jackson JM, Adams SA. Reliability and revision of the Nottingham sensory assessment for stroke patients. Physiotherapy. 1998;84(8):358-65.
21. Maki T, Quagliato EMAB, Cacho EWA, Paz LPS, Nascimento NH, Inoue MMEA, et al. Estudo de confiabilidade da aplicação da escala de Fugl-Meyer no Brasil. Rev Bras Fisioter. 2006;10(2):177-83.
22. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46(12):1417-32.
23. Mao HF, Hsueh IP, Tang PF, Sheu CF, Hsieh CL. Analysis and comparison of the psychometric properties of three balance measures for stroke patients. Stroke. 2002;33(4):1022-7.
24. Côté R, Batista RN, Wolfson CM, Hachinski V. Stroke assessment scales: guidelines for development, validation and reliability assessment. Can J Neurol Sci. 1988;15(3):261-5.
25. Fleiss JL, Levin B, Paik MC. Statistical methods for rates and proportions. 2º ed. New York: John Wiley & Sons; 1999.
26. Bland JM, Altman DG. Statistical method for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307-10.
27. Nunnally JC. Psychometric theory. 2ª ed. New York: McGraw-Hill; 1978.
28. Ware JE, Brook RH, Davies AR, Williams KN, Stewart A, Rogers WH, et al. Model of health and methodology. In: Ware JE, Brook RH, Davies AR, Williams KN, Stewart A, Rogers WH, et al. (editors). Conceptualization and measurement of health for adults in the health insurance study. Santa Monica: RAND Corporation; 1980. p. 1-47.
29. Stolk-Hornsveld F, Crow JL, Hendriks EP, van der Baan R, Harmeling-van der Wel BC. The Erasmus MC modifications to the (revised) Nottingham sensory assessment: a reliable somatosensory assessment measure for patients with intracranial disorders. Clin Rehabil. 2006;20(2):160-72.
30. Gaubert CS, Mockett SP. Inter-rater reliability of the Nottingham method of stereognosis assessment. Clin Rehabil. 2000;14(2):153-9.
31. Winward CE, Halligan PW, Wade DT. Somatosensory recovery: a longitudinal study of the first 6 months after unilateral stroke. Disabil Rehabil. 2007;29(4):293-9.
32. Connell LA, Lincoln NB, Radford KA. Somatosensory impairment after stroke: frequency of different deficits and their recovery. Clin Rehabil. 2008;22(8):758-67.
33. Clark GS, Siebens HC. Reabilitação geriátrica. In: De-Lisa já, Gans BM (editores). Tratado de medicina de reabilitação: princípios e prática. São Paulo: Manole; 2002. p. 1013-47.
Nome: ____________________________________________________ Data do AVE: _____/_____/_____
Idade:______________________ Tel(s): (____) ____________________ Tipo do AVE (H/I): _____________
Examinador: ________________________________________________ Data da avaliação: ____/____/____
Lado do corpo afetado: ( ) Direito ( ) Esquerdo
( ) Nenhum
( ) Ambos Se AMBOS, lado avaliado: _______ Presença de edema: ( ) Sim ( ) Não Se sim, onde? ________________
Sensação Tátil Regiões do
corpo
Toque leve Pressão Picada Temperatura Localização tátil Toque bilateral
simultâneo Propriocepção
D E D E D E D E D E
Face Tronco Ombro Cotovelo Punho Mão Quadril Joelho Tornozelo Pé
Avaliação sensorial de Nottingham (Lincoln et al.19)
Moeda de R$ 0,01 Caneta esferográfica Pente Esponja Xícara
Moeda de R$ 0,10 Lápis Tesoura Flanela Copo
Moeda de R$ 1
Estereognosia
Sensação Tátil e Estereognosia Propriocepção Discriminação entre 2 pontos
0: Ausente 0: Ausente 0: Ausente
1: Alterado 1: Execução do movimento (direção errada) 1: >3mm dedos e >8 mm mão 2: Normal 2: Direção do movimento (>10°) 2: <3mm dedos e <8 mm mão 4 a 9: Não testável 3: Normal ou posição articular <10° 4 a 9: Não testável
4 a 9: Não testável
Pontuação
Discriminação entre dois pontos
Palma da mão
mm Pontuação
Pontas dos dedos
mm Pontuação
Comentários: (por exemplo: edema ou palidez presente, meias de compressão, presença de reflexos).
Appendix 1