Detour technique, Dipping technique, or IIeal bladder
flap technique for surgical correction of uretero-ileal
anastomotic stricture in orthotopic ileal neobladder
_______________________________________________
Mohamed Wishahi
1, Hossam Elganzoury
1, Amr Elkhouly
11Department of Urology, Theodor Bilharz research Institute, Cairo, Egypt
ABSTRACT
ARTICLE
INFO
______________________________________________________________ ______________________
Background: Uretero-ileal anastomotic stricture (UIAS) is a urological complication after ileal neobladder, the initial management being endourological intervention. If this fails or stricture recurs, surgical intervention will be indicated.
Design and Participants: From 1994 to 2013, 129 patients were treated for UIAS after un-successful endourological intervention. Unilateral UIAS was present in 101 patients, and bilateral in 28 patients; total procedures were 157. The previous ileal neobladder techniques were Hautmann neobladder, detubularized U shape, or spherical shape neobladder.
Surgical procedures: Dipping technique was performed in 74 UIAS. Detour technique was done in 60 renal units. Ileal Bladder flap was indicated in 23 renal units. Each procedure ended with insertion of double J, abdominal drain, and indwelling catheter.
Results: Follow-up was done for 12 to 36 months. Patency of the anastomosis was found in 91.7 % of cases. Thirteen patients (8.3%) underwent antegrade dilatation and insertion of double J.
Conclusion: After endourological treatment for uretero-ileal anastomotic failure, ba-sically three techniques may be indicated: dipping technique, detour technique, and ileal bladder flap. The indications are dependent on the length of the stenotic/dilated ureteral segment. Better results for long length of stenotic ureter are obtained with detour technique; for short length stenotic ureter dipping technique; when the stenotic segment is 5 cm or more with a short ureter, the ileal tube flap is indicated. The use of double J stent is mandatory in the majority of cases. Early intervention is the rule for protecting renal units from progressive loss of function.
Key words:
Urethral Stricture; Urinary Bladder; Surgical Flaps
Int Braz J Urol. 2015; 41: 796-803
_____________________
Submitted for publication: July 26, 2013
_____________________
Accepted after revision: June 08, 2014
INTRODUCTION
Uretero-ileal anastomotic stricture (UIAS) in orthotopic ileal neobladder may develop in 4-10 % of cases in the follow-up period of 6-36 months (1-6). Various techniques were described to treat this complication which were mainly en-dourological, but not always successful (1, 4-9). The incidence of stricture would result in any of the described techniques of uretero-ileal
recurrent urinary tract infection (UTI), and ulti-mately loss of kidney function. The primary treat-ment is placetreat-ment of a percutaneous nephrostomy tube followed by antegrade dilatation of the stric-ture and insertions of double J ureteral stent (4-8). The endourological procedure would fail due to impassable stricture, or the stenosis would recur soon after removal of the double J stent. The sur-gical approaches and standardization of the tech-niques for surgical correction of UIAS were not described before. Our goal is to describe our expe-rience in the surgical management of uretero-ileal strictures.
MATERIALS AND METHODS
From 1994 to 2013, we performed surgical correction of uretero-ileal stricture in 129 patients after radical cystectomy for invasive carcinoma of the bladder with orthotopic ileal neobladder by different techniques that included detubularized U-shaped neobladder, Hautman neobladder, or spherical shape neobladder. Most of these patients were referrals from different hospitals where the cystectomy procedure and the ileal neobladder were done by other urologists. Part of the ma-terials and the surgical procedures were done in private hospitals to which the authors are affilia-ted to. Patients data were retrieved from hospital and private archives and extracted from doctoral theses that were completed before the year 2004. Patients included 112 men and 17 women. Total number of renal units affected by UIAS was 157. The incidence of bilateral stenosis was 28 out of 129 patients. Left side stricture was 68%, while the right side was 32%. The median interval to diag-nosis of stricture was 8 months.
Investigations at presentation included la-boratory work for renal function, liver function, prothrombin concentration, CBC, hepatitis ma-rkers, blood sugar, urine analysis and bacteriolo-gy. Imaging studies included abdominal ultraso-nography and non-contrast CT-urography.
Initial intervention was ultrasound-guided placement of a percutaneous nephrostomy tube for drainage of the obstructed kidney, antibio-tics being administered when urine was infected. Some cases referred to us had undergone insertion
of nephrostomy tube and unsuccessful endourolo-gical procedure to insert ureteric stent.
Antegrade urography was done to evalu-ate the site and length of the stricture segment, urine cytology from the obstructed renal unit and the neobladder, cystoscopy was done to exclude cancer recurrence in the ileal neobladder pouch. Endourological management to treat the obstruc-tion was tried first by passing a guide wire. After successfully passing the guide wire, the obstructed ureter was dilated by balloon catheter, followed by insertion of double J ureteral stent being left for 30 days. Development of restenosis, manifested by dilatation of the upper tract and/or recurrent UTI was an indication for surgical intervention.
Inclusion criteria in this series of 157 renal units were: 1) Complete obstruction of the ureter with no passage of the contrast media to the neo-bladder shown in antegrade urogram (Figure-1A); CT-urography confirming the complete ureteral obstruction and the length of the stenotic segment (Figure-1B); 2) Recurrent uretero-ileal anastomo-tic stricture following endourological dilatation and insertion of double J, with recurrent attacks of acute pyelonephritis.
Surgical Technique
Incision and Identification of the Ureter and Ne-obladder
from adhesion till it reaches the stenotic segment (Figure-2). The length of the stenotic segment is measured and according to the distance between the distal end of the dilated ureter and the neobla-dder the procedure is selected.
Detour Technique
Detour means side way, not the straight main street. The technique is illustrated in Figu-re-3. It was done in 60 uretero-ileal anastomotic strictures. The dilated ureter is followed down to the stenotic site. If the ureter has an insufficient length to reach the neobladder when it is empty and if cutting the ureter will not allow tension--free anastomosis, then the detour technique is performed. The site of the anastomosis is selec-ted in the neobladder which is facing the lowest point in the dilated ureter. The ureter is not dis-connected from the stenotic segment which will act as a fixation point. The width of the opening in the neobladder will be 1-2cm length. The mesen-teric vessels of the mesentery of the ileal neobladder which is crossing the hiatus will be controlled by coagulation or multiple 4/0 interrupted sutures. A 1-2cm opening is made in the ureter facing the ne-obladder hiatus. Double J ureteric stent is passed
Figure 1 - Uretero-ileal anastomotic stricture. (A) Antegrade urogram showing complete obstruction of the ureteroileal anastomotic stricture. (B) CT urography showing obstructed uretero-ileal anastomosis with dilatation of the renal unit.
Figure 2 - Intraoperative view showing the distended obstructed ureter and the distended neobladder as the ureter and the bladder were filled with saline solution via the nephrostomy tube and the bladder catheter.
to the kidney and the neobladder. The edges of the two hiatus are connected with interrupted 3 zero polyglycolic acid sutures. An abdominal drain is placed at the site of operation, and an indwelling urethral catheter is passed to the ileal neobladder.
Dipping Technique
The technique is performed as illustrated in Figures 4 and 5. The dilated ureter is followed down to the stenotic site. When the ureter has sufficient length to reach the neobladder when it is empty, then the dipping technique is performed. A hiatus site in the neobladder is chosen being equal to the diameter of the dilated ureter; interrupted sutures are made around the hiatus to control the possi-ble mesenteric vessels crossing this area. Doupossi-ble J ureteric stent is passed to the kidney and the ne-obladder; the ureter is dipped into the neobladder and fixed to it with 4-6 interrupted sutures with 3/0 polyglycolic acid sutures that are passed from the seromuscular layers of the ureter to the wall of the neobladder. An indwelling catheter is left in the ne-obladder, abdominal drain is placed in the operation site. The abdominal incision is closed in layers.
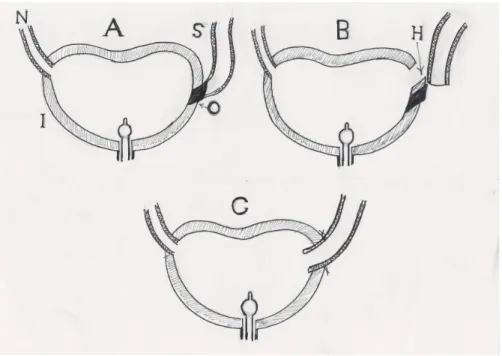
Figure 3 - Detour technique. (A) The stenosed short ureter and the obliterated segment. (B) Two hiatus are created in the ureter and in the neobladder facing each other. (C) Two hiatus are connected with interrupted sutures in a side to side fashion.
A = Normal ureter; S = Stenosed Ureter; O = Obliterated segment; I = Ileal neobladder; H = New hiatus
Ileal Bladder Flap Technique
Figure 4 - Dipping technique. (A) The stenosed long ureter and short obliterated segment. (B) The ureter is disconnected from the obliterated segment, and a hiatus is made in the ileal neobladder. (C) The ureter is implanted in the new bladder by dipping it in the hiatus; interrupted sutures are made.
A = Normal ureter; S = Stenosed Ureter; O = Obliterated segment; I = Ileal neobladder; H = New hiatus
Figure 5 - Intra-operative steps of dipping technique. (A) The obstructed ureter is identified and the site of obliterated segment is viewed. (B) The obstructed ureter is disconnected from the obliterated segment. (C) A hiatus is made in the neobladder to receive the dilated ureter. (D) The ureter is dipped into the neobladder, interrupted seromuscular sutures are made to fix the ureter to the ileal neobladder.
A B C D
ureter with interrupted sutures. An indwelling ca-theter is left in the neobladder, and an abdominal drain is placed in the site of operation.
Post-operative Care and Follow-up
In the three techniques, the indwelling urethral catheter was removed after one week post-operatively, if the abdominal drain was dry.
RESULTS
Surgical intervention for uretero-ileal stric-ture was done in 157 ureters. Three techniques were applied, the choice of either technique depending upon the length of the stenotic segment, and the length of the dilated ureter whether it would allow a tension free-anastomosis of the ureter to the ne-obladder. If so, the dipping technique was applied. In case the obstructed ureter was short and the stenotic segment was 2-3cm, the detour technique was applied. In presence of long stenotic segment of 5cm with short ureter, a tube flap technique was indicated. In patients with bilateral stricture, each side was dealt with independently.
Dipping technique was done in 74 renal units (47.1%), detour technique in 60 renal units (38.2%), and ileal tube flap ureteroplasty in 23 re-nal units (14.7%). The indwelling catheter and ab-dominal drain were removed after 7 days if there
was no leakage. The double J ureteric stent was re-moved after 30 days of removal of the indwelling catheter. 10 patients were reported to have urine leakage following removal of the indwelling ca-theter. Re-insertion of the catheter was done for another 5 days where the leakage stopped. Posto-perative follow-up for 12-36 months showed re-solution of the pelvic-calyceal dilatation and no re-stricture in 91.7 % of cases. Thirteen patients (8.3%) showed unresolved dilatation of the upper tract and recurrent UTI with febrile episodes; they underwent antegrade ballon dilatation of the ure-tero-ileal region and insertion of double J for 3 months. In 8.3% of cases, no restenosis was recor-ded in the follow-up period.
DISCUSSION
Uretero-ileal anastomotic stricture is a chal-lenging urological complication after orthotopic
Figure 6 - Ileal bladder flap technique. (A) Short ureter and long obliterated segment. (B) The ureter is disconnected from the stenosed segment. An ileal flap is created from the lateral side of the neobladder to avoid mesenteric vessels, its base is equal to the circumference of the dilated ureter. (C) The flap is fashioned to form a tube. (D) The newly created tube is anastomosed to the cut end of the dilated ureter.
ileal neobladder following radical cystectomy. Such complication will ultimately lead to loss of kidney function. In our series, we treated 157 re-nal units in 129 patients with failed endourologi-cal procedures. Schöndorf et al. (1), in their study on 74 patients with 85 obstructed renal units due to uretero-ileal anastomotic stricture, concluded that open surgical revision produces better re-sults than primary invasive endourological inter-vention for uretero-ileal stricture. In our study the enrolling criteria was the failed endourolo-gical intervention or complete occlusion of the stricture segment. Stenzel et al. (2) reported that occurrence of uretero-ileal stricture depends on the technique used for construction of ileal neo-bladder; in their series they reported the inciden-ce to be between 2.7 to 3.8%. In our series, most of the cases were referred from other hospitals - university hospital as well as private sector. Our retrospective study covers the period between 1994 till 2013. Echo et al. (5) reported the inci-dence of uretero-ileal anastomotic stricture to be 5.2% and 18.3% in two groups of patients who underwent ileal neobladder and stenting of the uretero-ileal anastomosis with double J or open--end ureteric stent. They emphasised the fre-quency of occurrence of stricture. Maksiomovic et al. (6) had a 73.5 % success for endourological treatment of uretero-ileal anastomotic stricture and stated that the success of the endourologi-cal procedure was based upon morphology of the stricture. In our series, the completely obstructed stricture had failed endourological intervention. Echo et al. (5) in their series reported a failure rate of 26.5% which necessitated open surgical intervention. Liatsikos et al. (8) described the use of a self-expandable metal stent for uretero-ileal anastomotic stricture in 18 patients; pre-condi-tion of feasibility of their technique being the primary patency of the stricture.
In our series, we applied three techniques for the open surgical treatment of uretero-ileal stricture; application of either technique was de-cided on the length of the stenotic segment and the length of the dilated ureter.
The present study is, to our knowledge, the largest series for the challenging complica-tion of ureteroileal anastomotic stricture after
orthotopic ileal neobladder. We described three different surgical techniques that covered the di-fferent possibilities of operative findings. Contra-ry to other authors (4), in our series we did not meet a condition that indicated to use an intes-tinal ileal segment or to perform complete ileal replacement of the ureter in order to bridge the obstructed segment. The three techniques fulfil-led the criteria of direct access to the targeted site of stricture, avoided unnecessary dissection, and secured a tension-free anastomotic suture line.
CONCLUSIONS
The three techniques described for treat-ment of uretero-ileal anastomotic stricture after radical cystectomy for bladder cancer and ile-al neobladder replacement appear to be feasible surgical procedures. Dipping technique, detour technique and ileal bladder flap were applied to three potential morphological types of ureteric stenosis. Short and long term follow-up of the three procedures showed success and no recur-rence of stenosis in 91.7% of cases. 8.3% renal units needed a second procedure of endourologi-cal dilatation and insertion of double J, in these cases there was no obliteration of the anastomo-tic site and not needed secondary operation. Ho-wever, surgical treatment of uretero-ileal stric-ture should be the second step after unsuccessful endourological intervention, or recurrent stric-ture. An absolute indication to resort to surgical intervention is the radiological finding of com-plete obstruction of the stricture. Early interven-tion to treat uretero-ileal stricture will save renal units from progressive loss of function.
ABBREVIATIONS
UIAS = Ureter- ileal anastomotic stricture UTI = Urinary tract infection.
CONFLICT OF INTEREST
REFERENCES
1. Schöndorf D, Meierhans-Ruf S, Kiss B, Giannarini G, Thalmann GN, Studer UE, et al. Ureteroileal strictures after urinary diversion with an ileal segment-is there a place for endourological treatment at all? J Urol. 2013;190:585-90. 2. Stenzl A, Sherif H, Kuczyk M. Radical cystectomy with
orthotopic neobladder for invasive bladder cancer: a critical analysis of long term oncological, functional and quality of life results. Int Braz J Urol. 2010;36:537-47.
3. Ballouhey Q, Thoulouzan M, Lunardi P, Bellec L, Huyghe E, Plante P, et al. Prospective study of the results of ureterointestinal anastomosis in 100 patients after the Hautmann ileal neobladder with double chimney. Prog Urol. 2012;22:255-60.
4. Nassar OA, Alsafa ME. Experience with ureteroenteric strictures after radical cystectomy and diversion: open surgical revision. Urology. 2011;78:459-65.
5. Echo H, Zerbib M, Saighi D, Amsellem-Ouazana D, Flam T, Debré B, Peyromaure M. Use of double J ureteral stent as an alternative to prevent ureteroileal anastomosis stricture in orthotopic bladder substitution. Prog Urol. 2009;19:127-31.
6. Maksimovic HM, Markovic BB, Pejcic T, Hadzi Djokic J, Markovic Z, Yachia D. Interventional radiology methods of treating ureteral strictures developed on anastomoses after the radical cystectomy in Mainz pouch II and ileal conduit derivation. Acta Chir Iugosl. 2007;54:83-7.
7. Varkarakis IM, Delis A, Papatsoris A, Deliveliotis C. Use of external ureteral catheters and internal double J stents in a modified ileal neobladder for continent diversion: a comparative analysis. Urol Int. 2005;75:139-43.
8. Liatsikos EN, Kagadis GC, Karnabatidis D, Katsanos K, Papathanassiou Z, Constantinides C, et al. Application of self-expandable metal stents for ureteroileal anastomotic strictures: long-term results. J Urol. 2007;178:169-73.
_______________________ Correspondence address: