BrazJOtorhinolaryngol.2014;80(5):455---456
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
CASE
REPORT
Opsoclonus-ataxia
syndrome
in
an
adolescent:
an
acute
otitis
media
complication
夽
Síndrome
de
opsoclonus-ataxia
em
adolescente:
uma
complicac
¸ão
de
otite
média
aguda
Rafael
Bispo
de
Souza,
Pedro
Henrique
Alves
do
Amaral,
Daniel
de
Sousa
Michels,
Lisiane
Seguti
Ferreira
∗FaculdadedeMedicinadaUniversidadedeBrasília(UNB),Brasília,DF,Brazil
Received22January2013;accepted27March2013 Availableonline3July2014
Introduction
Opsoclonusisdefinedasnon-rhythmic,involuntary, sponta-neous,multidirectional,andhyperkineticeye movements, withalargeamplitudeandhighfrequency(10---15Hz).These movements arepresent during visual fixation and conver-gence,andremainactiveduringsleepandwhentheeyelids areclosed.Theyshouldnotbeconfusedwithanacquired nystagmus, which is usually unidirectional, withfast and slowcomponents.Inaddition,opsoclonusisdifferentfrom eyeflutter,asthismovementisrestrictedtothehorizontal plane.
The opsoclonus-myoclonus-ataxiasyndrome(OMAS)is a rareconditioncharacterizedbyopsoclonusassociatedwith compensatoryheadmovements,myoclonus,andcerebellar
夽 Please cite this article as: de Souza RB, do Amaral PH,
MichaelsDS,FerreiraLS.Opsoclonus-ataxiasyndromeinan adoles-cent:anacuteotitismediacomplication.BrazJOtorhinolaryngol. 2014;80:455---6.
∗Correspondingauthor.
E-mail:[email protected](L.S.Ferreira).
ataxiamostlikelysecondarytoanautoimmunemechanism. Theetiologiesincludeparainfectious,paraneoplastic,toxic, and metabolic causes. Among the paraneoplastic causes, neuroblastomaisprominentinchildhoodandsmall-celllung carcinomastandsoutinadults.1,2
The objective of this article was to present a case of OMAS secondary to a CNS infection resulting from an unusualcourseofanacuteotitismedia(AOM)complicated byotomastoiditisinapreviouslyhealthyadolescent.
Case
report
NCO, an eleven-year-old girl, experienced an episode of bacterialpharyngitisthatwastreatedwithbenzylpenicillin. Feverpersisted,andshedevelopedrecurringvomiting,after whichAOMwasfound;amoxicillinwasinitiatedand cefurox-imewasadded. Approximately15 daysafterthe onsetof symptoms,shecomplainedof dizzinessand unstablegait, and her mother noticed non-rhythmic eye movements in botheyes.
She was admitted to the University Hospital. On the generalphysical examination,thepatientwasinanormal
http://dx.doi.org/10.1016/j.bjorl.2014.05.027
456 deSouzaRBetal.
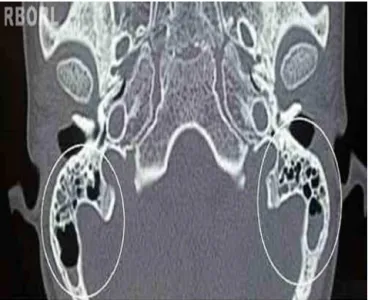
Figure 1 Mastoid computed tomography, cross-sectional view.Withinthe clearcircles,a bilateral partialclouding of mastoidcellsisobserved.
state, exhibiting irritation; her skin was pale, the tym-panic membraneswerebulging and hyperemicbilaterally, and no discharge was observed from the ear canal. No other changes, such as enlarged lymph nodes, enlarged liverandspleen,orachangeinheartorlungsoundswere observed.Duringotoneurologicalexamination,thepatient wasconsciousandhadrapid,frequent,involuntary, multidi-rectional(bothhorizontalandvertical),unpredictable,and disorderedeyemovements,inadditiontoaxialcerebellar ataxia(stableRomberg,Fukudawithbroadbase,andno dys-metriaor dysdiadochokinesia).Rhinoscopywasnormal.No myoclonus,meningealsigns, orcranial nerveimpairments wereobserved.
Thecompletebloodcountshowedincreasedwhiteblood cells (40,700 leucocytes), with neutrophils predominat-ing (89%) and no left shift. Cranial tomography revealed a bilateral partial clouding of mastoid cells (Fig. 1). Lumbar puncture showed pleocytosis (18 cells, predom-inance of lymphocytes and monocytes) with no other findings. Audiometry showed mixed (sensorineural and conductive) hearing loss. Cranial MRI was normal, and the entire metabolic investigation and infectious agents screening,includingHIV, hepatitis,rubella, toxoplasmosis, cytomegalovirus,herpes,andEpstein---Barrvirus,were neg-ative.Following a 28-day course of parenteral antibiotics (ceftriaxoneandoxacillin), therewascompleteregression ofallsignsandsymptoms.
Discussion
The present patienthadan AOM complicatedby bilateral mastoiditis,progressingtoencephalitisover athree-week period.Thiscoursewasunusualnotonlyfortheearly diag-nosisinthispatient,butalsoduetotheantimicrobialagents currentlyavailable.3,4
Inaddition,whenthepatientwasadmittedtothe Uni-versityHospital,shehadnoearacheorretroauricularpain, buthergaitwasunstableandshehadassociatedeye move-ments,thus meetingthecriteriafor theopsoclonus-ataxia syndrome.1,2ThesesymptomscouldonlybelinkedtoanAOM
afterotomastoiditiscomplicatedbyencephalitiswasfound, whichexplainedthefindings.Anumberofpatientsmayhave neurologicalsymptomsasancomplicationofotomastoiditis, butitisunusualtofindanOMAS.4Therichnessof
semiologi-caldatafordifferentialdiagnosisoftheeyemovementsand the rareness of this condition, usually present in younger children,makethiscaseunique.2
Since there was clinical and laboratorial evidence of bacterial infection associated with a good response to antibiotics, the use of anti-inflammatory agents and immunosuppressingdrugsusuallyusedinOMASmanagement was not required. The findings demonstrate that there is nodefinitiveruleintreatingthesecasesand,by consider-ingtheseveraletiologies,managementshouldbechosenin accordancewiththeuniquenessofeachpatient.5,6
Thepromptdiagnosisinthiscaseparticularlyfavoredthe goodclinicalcourseandavoidedadditionalunnecessaryand costlymethodsusuallyemployedtoestablishadiagnosisin patientswithOMAS.Atthe30-dayandthe90-dayfollow-up, thepatientwasasymptomaticandherneurological exami-nationwascompletelynormal.
Final
remarks
The rare characterof this OMAS case, occurring after an acuteotitismedia,andthe favorablecoursehighlight the importance of a thorough history and a careful clinical examination to guide the investigation and therapeutic strategies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.SahuJK,PrasadK.Theopsoclonus-myoclonussyndrome.Pract Neurol.2011;11:160---6.
2.Desai J, Mitchell WG. Acute cerebelar ataxia, acute cere-bellitis and opsoclonus-myoclonus syndrome. J Child Neurol. 2012;27:1482---8.
3.Johnson NC, Holger JS. Pediatric acute otitis media: the casefor delayedantibiotic treatment.JEmergMed.2007;32: 279---84.
4.Osborn AJ, Blaser S, Papsin BC. Decisions regarding intracra-nialcomplicationsfromacutemastoiditisinchildren.CurrOpin OtolaryngolHeadNeckSurg.2011;19:478---85.
5.GlatzK,MeinckH-M,Wildemann B.Parainfectious opsoclonus-myoclonussyndrome:highdoseintravenousimmunoglobulinsare effective.JNeurolNeurosurgPsychiatry.2003;74:277---82. 6.BrunklausA, PohlK, ZuberiSM. Outcomeand prognostic