www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Trans-oral
endoscopic
partial
adenoidectomy
does
not
worsen
the
speech
after
cleft
palate
repair
夽
Mosaad
Abdel-Aziz
a,∗,
Badawy
Khalifa
a,
Ahmed
Shawky
a,
Mohammed
Rashed
b,
Nader
Naguib
b,
Asmaa
Abdel-Hameed
caDepartmentofOtolaryngology,CairoUniversity,Cairo,Egypt bDepartmentofOtolaryngology,BeniSuefUniversity,BeniSuef,Egypt
cDepartmentofOtolaryngology(PhoniatricUnit),CairoUniversity,Cairo,Egypt
Received16June2015;accepted12August2015 Availableonline18December2015
KEYWORDS
Endoscopic adenoidectomy; Cleftpalate;
Adenoidhypertrophy; Velopharyngeal insufficiency
Abstract
Introduction:Adenoid hypertrophy may play arole in velopharyngeal closure especially in patientswithpalatalabnormality;adenoidectomymayleadtovelopharyngealinsufficiencyand hypernasalspeech.Patientswithcleftpalateevenafterrepairshouldnotundergo adenoidec-tomyunlessabsolutelyneeded,andinsuchsituations,conservativeorpartialadenoidectomy isperformedto avoidthe occurrenceofvelopharyngeal insufficiency.Trans-oralendoscopic adenoidectomyenablesthesurgeontoinspectthevelopharyngealvalveduringtheprocedure. Objective:Theaimofthisstudywastoassesstheeffectoftransoralendoscopicpartial ade-noidectomyonthespeechofchildrenwithrepairedcleftpalate.
Methods:Twentychildren withrepairedcleftpalateunderwenttransoralendoscopicpartial adenoidectomytorelievetheirairwayobstruction.Theprocedurewascompletelyvisualized with the useof a70◦ 4mm nasal endoscope; theupper part ofthe adenoidwas removed
usingadenoidcuretteandSt.ClaireThompsonforceps,whilethelowerpartwasretainedto maintainthevelopharyngealcompetence.Preoperativeandpostoperativeevaluationofspeech wasperformed,subjectivelybyauditoryperceptualassessment,andobjectivelybynasometric assessment.
Results:Speechwasnotadverselyaffectedaftersurgery.Thedifferencebetween preopera-tiveandpostoperativeauditoryperceptualassessmentandnasalancescoresfornasalandoral sentenceswasinsignificant(p=0.231,0.442,0.118respectively).
夽 Pleasecitethisarticleas:Abdel-AzizM,KhalifaB, ShawkyA,RashedM,Naguib N,Abdel-HameedA. Trans-oralendoscopicpartial adenoidectomydoesnotworsenthespeechaftercleftpalaterepair.BrazJOtorhinolaryngol.2016;82:422---6.
∗Correspondingauthor.
E-mail:[email protected](M.Abdel-Aziz). http://dx.doi.org/10.1016/j.bjorl.2015.08.025
Conclusions: Transoralendoscopicpartialadenoidectomyisasafemethod;itdoesnotworsen the speech ofrepaired cleftpalate patients. Itenables the surgeon tostrictly inspectthe velopharyngeal valveduringtheprocedurewith betterdeterminationoftheadenoidalpart thatmaycontributeinvelopharyngealclosure.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Adenoidectomia endoscópica; Fendapalatina; Hipertrofiada adenoide; Insuficiência velofaríngea
Adenoidectomiaparcialendoscópicatransoralnãopioraafaladepacientescom correc¸ãocirúrgicadefendapalatina
Resumo
Introduc¸ão: Ahipertrofiadaadenoidepodedesempenharumpapelnofechamento velofarín-geo,especialmenteem pacientescomanormalidadepalatal;aadenoidectomiapodelevarà insuficiência velofaríngeae falahipernasal. Os pacientescom fenda palatina, mesmo após a correc¸ão, não devem ser submetidos a adenoidectomia, exceto quando absolutamente necessário e, em tais situac¸ões, aformaconservadora ou parcialé realizada para evitar a ocorrênciadeinsuficiênciavelofaríngea.Aadenoidectomiaendoscópicatransoralpermiteao cirurgiãoinspecionaraválvulavelofaríngeaduranteoprocedimento.
Objetivo: Oobjetivodesteestudofoiavaliaroefeitodaadenoidectomiaparcialendoscópica transoralnafaladecrianc¸assubmetidasàcorrec¸ãodefendapalatina.
Método: Umtotalde20crianc¸ascomfendapalatinapreviamentecorrigida,foisubmetidaa adenoidectomiaparcialendoscópicatransoral,paradesobstruc¸ãodasviasaéreas,.O procedi-mentofoicompletamentevisualizadocomousodeumendoscópiode4mmeângulode70◦;
apartesuperiordaadenoidefoiremovidacomumacuretaparaadenoideefórcepsSt.Claire Thompson,enquantoaparteinferiorfoiconservadaparamanteracompetênciavelofaríngea. Avaliac¸õesdafalaforamrealizadasnosperíodospréepós-operatório,deformasubjetivapela avaliac¸ãoperceptivo-auditiva,eobjetivapelaavaliac¸ãonasométrica.
Resultados: Afalanãofoiprejudicadaapósacirurgia.Adiferenc¸aentreosescoresdaavaliac¸ão perceptivo-auditiva e nasalância para as sentenc¸as nasais e orais nos períodos pré e pós-operatóriofoiinsignificante(p=0,231,0,442,0,118,respectivamente).
Conclusões: Aadenoidectomiaparcialendoscópicatransoraléummétodoseguro,enãopiora a fala dos pacientes com fenda palatina operada. Ela permite que o cirurgião inspecione rigorosamenteaválvulavelofaríngeaduranteoprocedimento,commelhordeterminac¸ãoda parteadenoidequepodecontribuirparaofechamentovelofaríngeo.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Adenoidhypertrophyisacommoncauseofairway
obstruc-tion in children; it may lead to mouth breathing, nasal
discharge, snoring,sleepapnea, andhyponasalspeech. It
also contributesto the pathogenesis of rhinosinusitis and
recurrent otitis media.1 However, the adenoid liesin the
posterior pharyngeal wall and may act as a pad against
thepalatefacilitatingvelopharyngealclosure,especiallyin
patientswithpalatalabnormality.Itspresencecan
compen-sateforashortorapoorlymobilepalate,aconditionthat
may follow cleft palate repair. Following adenoidectomy,
compensation is eliminated and velopharyngeal
insuffi-ciency (VPI) may result.2 Therefore, patients with cleft
palate---evenafterrepair---shouldnotundergo
adenoidec-tomy unless absolutely necessary, and in such situations
conservativeorpartialadenoidectomyisperformed.3,4
Patientswithadenoidhypertrophymayneedpartial
ade-noidectomy if they are prone to develop VPI after the
operation.Theprocedureentailsremovaloftheupperpart
thatobstructs the choanaeand preservation of thelower
partthatassistsinvelopharyngealclosure.2,5,6Several
meth-odsforadenoidremovalhavebeen previouslydescribedin
theliterature.Adenoidcuretteguidedbyanindirect
trans-oralmirrorandaheadlightisasimpleandquickprocedure
thathasalreadybeeninuseforalongtime,buttheindirect
visualizationoftheadenoidaltissuemaymakethesurgeon
unabletocompletelyclearthechoanae,especiallyifpartial
removalistheintendedprocedure.7Transnasalendoscopic
partial adenoidectomy has been used with the ability to
clearthechoanae precisely,6,8 butthismethod maymake
thesurgeonunabletocompletelyinspect the
velopharyn-gealvalvethatisusuallyhiddenbytheresidualadenoidal
of this study was to assess the effect of transoral
endo-scopicpartialadenoidectomyonthespeechofchildrenwith
repairedcleftpalate.
Methods
Twenty patients with adenoid hypertrophy were included
in this case series study. All patients have repaired cleft
palate.Theywere13malesandsevenfemales;theirages
ranged between 4 and 9 years with a mean age of 6
years.Eight patients hadbilateral complete cleft lip and
palate, seven patients had unilateral complete cleft lip
and palate, and five patients had cleft soft palate. The
patients were subjected to partial adenoidectomy in the
period from January 2008 to July 2013. The indication
forsurgerywashypertrophiedadenoidcausingobstructive
sleepapnea(OSA)thatwasdiagnosedbypolysomnography;
however, sleep apnea was not the objective issue of the
study.Patientswhounderwentsecondarycorrectivesurgery
for VPI, and who presented with craniofacial anomalies,
wereexcluded.Toexcludetonsillarhypertrophyasacause
ofairwayobstruction,childrenwithtonsillarsizemorethan
grade2onBrodskygradingscalewereexcluded.9Informed
consentswereobtained fromtheparents of thepatients,
and the principlesoutlined in the Declaration of Helsinki
were followed. In addition, the research protocol was
approvedbytheresearchethicscommitteeofourinstitute
(N-23-2008).
Allpatientsweresubjectedtothefollowing.
Otolaryngologicexamination
Fullear,noseandthroat,andheadandneckexaminations
wereperformed.Earexamination,includingtympanometry,
wasperformedfordetectionofmiddleeareffusion,aswell
asoral examination to assess the condition of the palate
andsizeofthetonsils,andtoexcludeanyother causeof
airwayobstruction.Also,nasalexaminationwasperformed
toexcludeanyothercauseofnasalobstruction.
Lateralneckradiography
AnX-rayofthenasopharyngealaircolumnwasperformed.
Onlypatients withcompletely obliteratednasopharyngeal
aircolumnwithadenoidaltissuewereincludedinthestudy.
Preoperativeassessmentofspeech
Patients underwent auditory perceptual assessment of
speech(APA) and nasometricassessment. Due tothe
dif-ficulty to see the velopharyngeal valve in patients with
obstructedchoanaecausedbyadenoidhypertrophy,flexible
nasopharyngoscopywasnotused.
Auditoryperceptualassessmentofspeech
Hypernasality,nasalemissionofair,andweakpressure
con-sonants were analyzed in each patient. Parameters were
gradedonafive-pointscale(0---4)inwhich0indicates
nor-maland4indicatesseverehypernasality,withatotalscore
of 12 on thethree elements. A lowerscore on thisscale
indicateslessdysfunction.
Nasometricassessment
Assessmentofnasalancewasperformed usinganasometer
(Model6200;KayElemetricsCorp.,LincolnPark,NJ),which
provides an acoustic measure of movement of the
vibra-tionalenergythroughthevocaltract.Nasometricdatawere
obtainedwhilethepatientsreadorrepeatedstandardized
Arabicnasalandoralsentences.
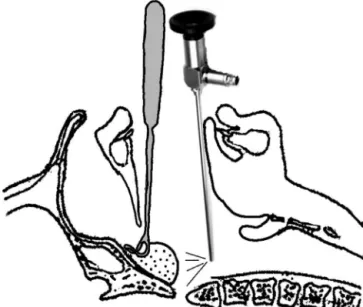
Operativeprocedure
Undergeneralanesthesiawithoralendotrachealintubation,
aBoyle---Davismouthgagwasusedtoopenthemouth.After
retractionofthesoft palatewithtworubber catheters,a
70◦ Hopkins4mmnasalendoscopewasintroducedthrough
the mouth (Fig.1).A camera(KarlStorzGmbH& Co KG;
Tuttlingen,Germany) wasmountedonthe endoscopeand
the endoscopic viewwas projectedon a monitor.
Transo-ral endoscopic partial adenoidectomy was performed, in
which the upper part of the adenoid was removed using
adenoid curette and St. Claire Thompson forceps, while
the lower part wasretained tomaintain the
velopharyn-geal competence.10 Coagulation diathermy was used for
hemostasis.Thetechniquewasstandardizedforallpatients
and it wasperformed by thefirst fiveauthors. After
par-tial adenoidectomyand insertionof nasopharyngeal pack,
patientswithmiddleeareffusionunderwentmyringotomy
andinsertionofventilationtubes.Uponawakening,patients
wereextubatedandplacedinthelateralposition,andthen
transferredtothepostanesthesiacareunitforobservation
ofrespirationandoxygensaturation.
Figure1 Anillustrationfortheprocedureshowstheadenoid curette is insertedinto the nasopharynxwhile the70◦ nasal
Postoperativeassessmentofvelopharyngeal function
Followingroutinepostoperativeinstructionsandfollowup,
patientsweredirectedtoreturnaftersixmonthsforAPAand
nasometricassessmentusingthesameparametersemployed
preoperatively.
Statisticalmethods
DatawerecodedandsummarizedusingStatisticalPackage
for Social Sciences version 17.0 for Windows (SPSS Inc.,
Chicago, IL). Quantitative variables are presented as
mean±standarddeviation.Comparisonofpreoperativeand
postoperativeresultsofauditoryperceptualassessmentand
nasometricassessmentwasdoneusingpairedtwo-samplet
test.p<0.05wasconsideredstatisticallysignificant.
Results
Twenty children with repaired cleft palate and adenoid
hypertrophywereenrolledinthestudy.Partial
adenoidec-tomy was performed to relieve the airway obstruction;
theprocedurewasdoneendoscopicallythroughthemouth
under complete visualization. Middle ear effusion was
detectedbilaterallyinsixpatients whoweretreatedwith
myringotomyandinsertionofventilationtubes.No
intraop-erativeorpostoperativecomplicationswereencountered.
Speech was not adversely affected after surgery
(Table 1). The mean preoperative baseline of auditory
perceptual assessment was 4.26±0.07, whereas
post-operatively it was 4.28±0.39. The difference between
preoperative and postoperative scores was insignificant.
Also,nasalance wasnot worsened after surgery.The
pre-operative scores were 30.1±6.7 for the nasal sentences
and13.88±0.198for theoralsentences, whereas
postop-erativescoreswere31.3±1.59forthenasalsentencesand
13.78±0.216fortheoralsentences.Thechangeswere
sta-tisticallyinsignificantforbothnasalandoralsentences.
Discussion
Patientswith cleft palate mayhave narrow airway space
when compared with non-cleft palate patients, although
there are no differences in the size of the tonsils and
adenoids between both groups.11 After palatoplasty, the
narrowing is increased, which may lead to OSA in some
Table 1 Pre- and postoperative assessment of speech parameters.
Preoperative Postoperative p-value
APA 4.26±0.07 4.28±0.39 0.231 Nasalance
scoreforNS
30.1±6.7 31.3±1.59 0.442
Nasalance scoreforOS
13.88±0.198 13.78±0.216 0.118
APA,auditoryperceptualassessment;NS,nasalsentences;OS, oralsentences.
patients.12,13However,conventionaladenoidectomyis
con-traindicatedincleftpalatepatientsevenafterrepair,asit
mayleadtoVPI,withconsequenthypernasalspeech.
Hyper-trophied adenoidal tissue may facilitate velopharyngeal
closure especially in patients with palatal abnormalities,
anditsremovalmayuncovertheproblem.2,3Toavoid
post-operative VPI in thosepatients, partial adenoidectomy is
recommended,in whichtheupperpartthat obstructsthe
choanaeisremoved,andthelowerpartthatmaysharein
velopharyngealclosureisretained.2,8
Many authors have discussed partial adenoidectomy in
submucouscleftpalatepatients.4---6Aconditionthatis
char-acterized by deficiency of muscles in the midline of the
softpalate,itleavesacentralgaponvelopharyngeal
clo-sure. In patients with adenoid hypertrophy, the disease
is usually asymptomatic, as the gap may be occupied by
the adenoidal tissue. So, partial adenoidectomy is
rec-ommended for adenoid hypertrophy of those patients.6,8
Althoughpatients withrepaired cleft palate areprone to
developpost-adenoidectomyVPI,littleismentionedinthe
literature about partial adenoidectomy after cleft palate
repair.Thepalatalmusclesofthecleftpalatepatientsare
usuallyhypoplasticandweakerthannormal,aproblemthat
isnot corrected by repair.2,4 Forthis reason,theadenoid
hypertrophyofrepairedcleftpalatepatientsshouldbe
man-agedlikethoseofpatientswithsubmucouscleftpalate.
This studywasconductedon20 childrenwithrepaired
cleftpalateandadenoidhypertrophy;transoralendoscopic
partialadenoidectomywasperformed.Theprocedure was
completelyvisualizedwithstrictinspectionofthe
velopha-ryngealvalve.The choanaewereclearedoutofadenoidal
tissuestoensureapatentairway,whilethelowerpartofthe
adenoidwasretainedtoavoiddisruptionofthe
velopharyn-gealvalve.Auditoryperceptualassessmentandnasometric
assessmentwereperformedpreandpostoperativelybythe
lastauthor;therewerenosignificantchangesinboth
param-eters.Flexiblenasopharyngoscopywasnotperformedinthe
assessmentofvelopharyngealfunction,asthechoanaewere
completely obstructed by adenoid that is seen
radiologi-cally,soitwould bedifficult toperform themaneuver in
awakepatients who shouldrepeat oral consonants tosee
thevelopharyngealclosure.
Endoscopicpartialadenoidectomyfor patientswhoare
pronetodeveloppostoperativeVPIisagoodtechniqueas
ithelpsthesurgeontoaccomplishhisgoal,whichisrelief
ofnasalobstruction withoutdisruptionof the
velopharyn-gealvalve.Itwasperformedtransnasally,usingthe4mm0◦
nasalendoscope,andtheadenoidaltissues wereremoved
by a cutting forceps.6,8 However,our patients underwent
theprocedure transorally,usingthe4mm 70◦ nasal
endo-scope, andthe adenoidal tissue wasremoved by adenoid
curetteandSt.ClaireThompsonforceps.Thesurgicalfield
iswiderwithtransoralthanwiththetransnasal approach,
soourtechniquefacilitateseasyclearanceofthechoanae
withgoodhemostasisifneededandstrictinspectionofthe
velopharyngealvalve.Inaddition,trans-oraladenoidectomy
ismorefamiliartotheotolaryngologists.
Transnasal endoscopic partial adenoidectomy has been
performed for patients with submucous cleft palate
by Finkelstein et al.6; relief of nasal obstruction was
achievedin allpatients,buttwooutoftendemonstrated
hypernasalitymaybeattributedtotheinabilityofthe
sur-geontoinspectthevelopharyngealvalvetransnasallyduring
theprocedure,asthevalvemaybehiddenbytheretained
lowerpartoftheadenoid,withdifficultytofreely
manip-ulatetherigidendoscope.However,Sternetal.8usedthe
samemaneuver,andnoneoftheirpatientsdeveloped
post-operativeVPI.Kakanietal.14usedaSt.Clairadenoidforceps
forremovalofadenoidinpatientswithpalatalabnormality,
underindirect vision with a laryngeal mirror. All patients
experiencedacompleteornear-completeresolutionoftheir
nasalobstruction,andnonedevelopedpermanentVPI.Also,
Tweedieetal.4performedtransoralpartialadenoidectomy
usingamalleablesuctioncoagulatorunderindirectvision.
They achieved complete relief of nasal obstruction
with-outworseningofpatients’speech.Ourmethodenablesthe
surgeontocompletely visualizethewholeprocedure,and
consequently todetermine precisely howmuchadenoidal
tissueisneededtoberemoved,toperformbetter
hemosta-sis,andtoavoidinjuryofthevelopharyngealarea.
It is worth mentioning that we did not use flexible
nasopharyngoscopy in the assessment of velopharyngeal
function,asourpatientshadcompletelyobstructedchoanae
by the hypertrophied adenoidal tissue. Also, we did not
presentOSA data,becausetheobjectiveofthestudy was
toassess theeffectof partialadenoidectomyon
velopha-ryngealfunction.Forastrongstatisticalimpact,thestudy
shouldbeappliedonalargesample ofpatients.However,
adenoidhypertrophyinpatientswithrepairedcleftpalateis
notcommon,sowerecommendalargermulticenterstudy.
Conclusion
Transoral endoscopic partial adenoidectomy is a safe
method; it does not worsenthe speechof repaired cleft
palate patients.It enables the surgeonto strictly inspect
thevelopharyngealvalveduringtheprocedurewithbetter
determinationoftheadenoidalpartthatmaycontributein
velopharyngealclosure.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TankelJW,CheesmanAD.Symptomreliefbyadenoidectomyand relationshiptoadenoidandpost-nasalairwaysize.JLaryngol Otol.1986;100:637---40.
2.Abdel-Aziz M. The effectiveness of tonsillectomy and par-tialadenoidectomyonobstructivesleepapneaincleftpalate patients.Laryngoscope.2012;122:2563---7.
3.MarynY, VanLierde K,De BodtM,Van Cauwenberge P.The effectsofadenoidectomyandtonsillectomyonspeechandnasal resonance.FoliaPhoniatrLogop.2004;56:182---91.
4.TweedieDJ,SkilbeckCJ,WyattME,CochraneLA.Partial ade-noidectomybysuctiondiathermyinchildrenwithcleftpalate, toavoidvelopharyngealinsufficiency.IntJPediatr Otorhino-laryngol.2009;73:1594---7.
5.Shapiro RS. Partial adenoidectomy. Laryngoscope. 1982;92:135---9.
6.FinkelsteinY,WexlerDB,NachmaniA,OphirD.Endoscopic par-tialadenoidectomyforchildrenwithsubmucouscleftpalate. CleftPalateCraniofacJ.2002;39:479---86.
7.El-BadrawyA, Abdel-AzizM.Transoralendoscopic adenoidec-tomy. Int J Otolaryngol. 2009, http://dx.doi.org/10.1155/ 2009/949315.
8.SternY,SegalK,YanivE.Endoscopicadenoidectomyinchildren withsubmucosal cleftpalate. IntJPediatr Otorhinolaryngol. 2006;70:1871---4.
9.BrodskyL.Modernassessmentoftonsilsandadenoids.Pediatr ClinNorthAm.1989;36:1551---69.
10.Abdel-Aziz M. Hypertrophied tonsils impair velopharyngeal functionafterpalatoplasty.Laryngoscope.2012;122:528---32. 11.RoseE,ThissenU,OttenJ,JonasI.Cephalometricassessment
oftheposteriorairwayspaceinpatientswithcleftpalateafter palatoplasty.CleftPalateCraniofacJ.2003;40:498---503. 12.Antony AK, Sloan GM. Airway obstruction following
palato-plasty: analysis of 247 consecutive operations. Cleft Palate CraniofacJ.2002;39:145---8.
13.LiaoYF,YunC,HuangCS,ChenPK,ChenNH,HungKF,etal. Lon-gitudinalfollow-upofobstructivesleepapneafollowingFurlow palatoplastyinchildrenwithcleftpalate:apreliminaryreport. CleftPalateCraniofacJ.2003;40:269---73.