Ulisses Alexandre Croti
1, Kathy J. Jenkins
2, Domingo Marcolino Braile
1Rev Bras Cir Cardiovasc 2011;26(3):511-5 MULTIMEDIA
Checklist em Cirurgia Cardíaca Pediátrica no Brasil: uma adaptação útil e necessária do International
Quality Improvement Collaborative for Congenital Heart Surgery in Developing Countries
Checklist in pediatric cardiac surgery in Brazil: an
useful and necessary adaptation of the Quality
Improvement Collaborative International
Congenital Heart Surgery in Developing Countries
In May 2009, a partnership was signed between the Children’s HeartLink Foundation and Pediatric Cardiovascular Surgery Department of São Jose do Rio Preto, in the Base Hospital of the Medical School of São José do Rio Preto (FAMERP). Since then, we have introduced changes in order to identify predictors of morbidity and mortality, establish appropriate routines and improve the quality of care for children with heart disease - congenital and acquired in childhood - in our environment [1].
One of the opportunities offered by the Children’s HeartLink Foundation was participation in International Quality Improvement Collaborative for Congenital Heart Surgery in Developing Countries, program form the Boston Children’s Hospital - Harvard Medical School - United States, coordinated by Dr. Kathy Jenkins [1].
With this program, we began to participate in a worldwide database, based on RACHS-1 [2]. All surgical patients receive a number to prevent identification and information
of the first 30 days or until hospital discharge are sent via Internet to the group at the Boston Children’s Hospital, which periodically informs us about our results so we can identify gaps and correct them.
The same group also minister videoconferences each month (called webinars), previously scheduled and with defined themes, which allows distance learning and facilitate dialogue between our group in Brazil and the group in the United States of America.
The primary aim of these classes and the program is to reduce mortality in 30 days and, therefore, three major themes have been presented and discussed throughout the year: basic practices for staff, reduction of surgical site infection and bacterial sepsis and safe practices during the operation. The checklist for pediatric cardiac surgery, adapted, which we present below is part of safe practices during operation. It should be used to improve patient care, improve communication and team work dynamics in the
RBCCV 44205-1315 DOI: 10.5935/1678-9741.20110034
THE VIDEO PERTINENT TO THE TEXT IS PUBLISHED ON THE JOURNAL WEBSITE: http://www.rbccv.org.br/video/v26n4/
1 . São José do Rio Preto Pediatric Cardiovascular Surgery Service -Hospital de Base – São José do Rio Preto Medical School, SP, Brazil.
2 . São José do Rio Preto Medical School, SP, Brazil. Children’s Hospital Boston – Harvard Medical School, Boston, MA, USA.
Correspondence address: Ulisses Alexandre Croti
Hospital de Base – Faculdade de Medicina de São José do Rio Preto (FAMERP) – Avenida Brigadeiro Faria Lima, 5544 – São José do Rio Preto, SP, Brasil – CEP 15090-000.
E-mail: [email protected]
CONFLICT OF INTEREST: The authors declare that they have conflict of interests; Braile Biomédica® provided the material used and supplied the video images of the operation, presenting its commercial products.
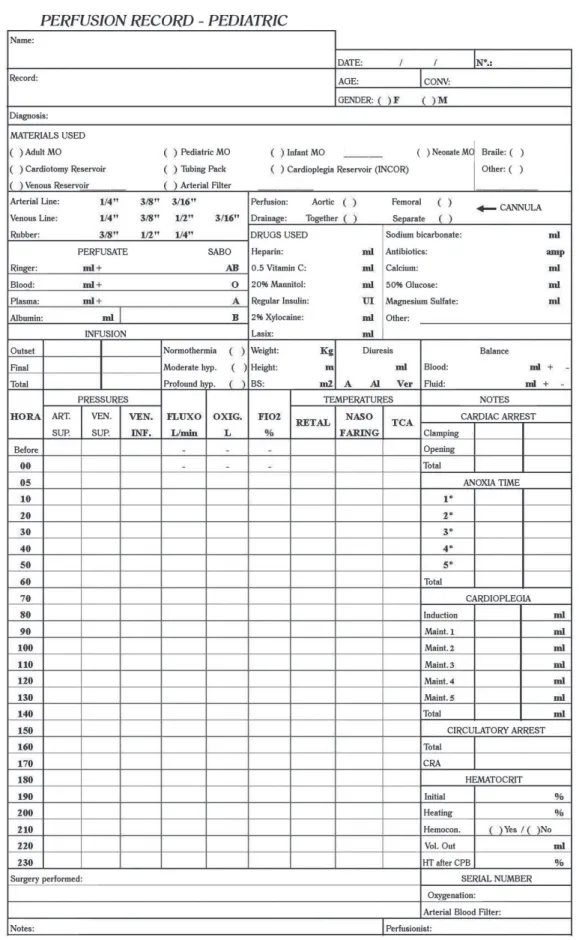
Fig. 2 - Checklist of cardiopulmonary bypass previously checked by perfusionist
Croti UA, et al. - Checklist in pediatric cardiac surgery in Brazil: an useful and necessary adaptation of the Quality Improvement Collaborative International Congenital Heart Surgery in Developing Countries
REFERENCES
1. Croti UA, Braile DM. Cooperação Internacional no Brasil: Children´s HeartLink. Rev Bras Cir Cardiovasc. 2010;25(1):VIII-IX.
2. Jenkins KJ, Gauvreau K, Newburger JW, Spray TL, Moller JH, Iezzoni LI. Consensus-based method for risk adjustment for surgery for congenital heart disease. J Thorac Cardiovasc Surg. 2002;123(1):110-8.
3. Pinto Jr VC, Daher CV, Sallum FS, Jatene MB, Croti UA. Situação das cirurgias cardíacas congênitas no Brasil. Rev Bras Cir Cardiovasc. 2004;19(2):III-VI.
4. Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Breizat AH, Dellinger EP, et al; Safe Surgery Saves Lives Study Group. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009;360(5):491-9.
Croti UA, et al. - Checklist in pediatric cardiac surgery in Brazil: an useful and necessary adaptation of the Quality Improvement Collaborative International Congenital Heart Surgery in Developing Countries
Rev Bras Cir Cardiovasc 2011;26(3):511-5
Thus, all being in agreement and aware of the procedure, the start of the operation is authorized simultaneously by the team.
PART III - AFTER THE END OF THE SURGERY The surgeon, instrumentist and circulating nurse, together with staff confirms the procedure that has been performed and make the conference of gauze and other materials.
PART IV – PASSAGE OF THE CASE TO ICU
In the ICU, the surgeon explains to the whole team he is receiving the patient with the surgery performed, possible complications and risks.
The anesthesiologist explains the care with ventilation, drug administration, hemodynamic stability, echocardiogram findings - when performed in the operating room -, availability of blood products and other data he may consider important.
The surgeon, anesthesiologist, intensivist, physiotherapist and nurses together discuss the case of the patient and do the planning for the first 24 hours in the ICU. Thus, the checklist for pediatric cardiac surgery is conclude.
ACKNOWLEDGEMENTS
The family, which authorized the use of images and data dissemination of the patient, Children’s HeartLink Foundation, Boston Children’s Hospital - Harvard Medical School, Boston, MA, USA; Mayo Clinic - Rochester, MN, USA; Children’s Hospitals and Clinics of Minnesota - Minneapolis , MN, USA and the staff of Pediatric Cardiovascular Surgery Department of SÃo Jose do Rio Preto, Brazil.
operating room, representing safety in the workplace for patients and professionals.
The video of this article is self explanatory and shows one of the routines that we use and believe that helps to prevent gaps in child care, allowing real and effective continuity during the treatment of heart defect in the preoperative, intraoperative and immediate postoperative period in Intensive Care Unit (ICU).
Determining a surgeon, an anesthetist and an instrumentist to be responsible for implementing the checklist is the first steps to success and adherence to all the team. Also, a large poster shall be posted on the wall of the operating room, so that at the time of completing the checklist no item is forgotten. The key word is: communication.
We believe that the checklist is easy to use, prevents errors and improves patient safety.
We expect all services in Brazil can use this process, which, as already demonstrated by the World Health Organization, saves lives and can be another tool to improve the situation of pediatric cardiac surgery in Brazil [3,4].
VIDEO DESCRIPTION
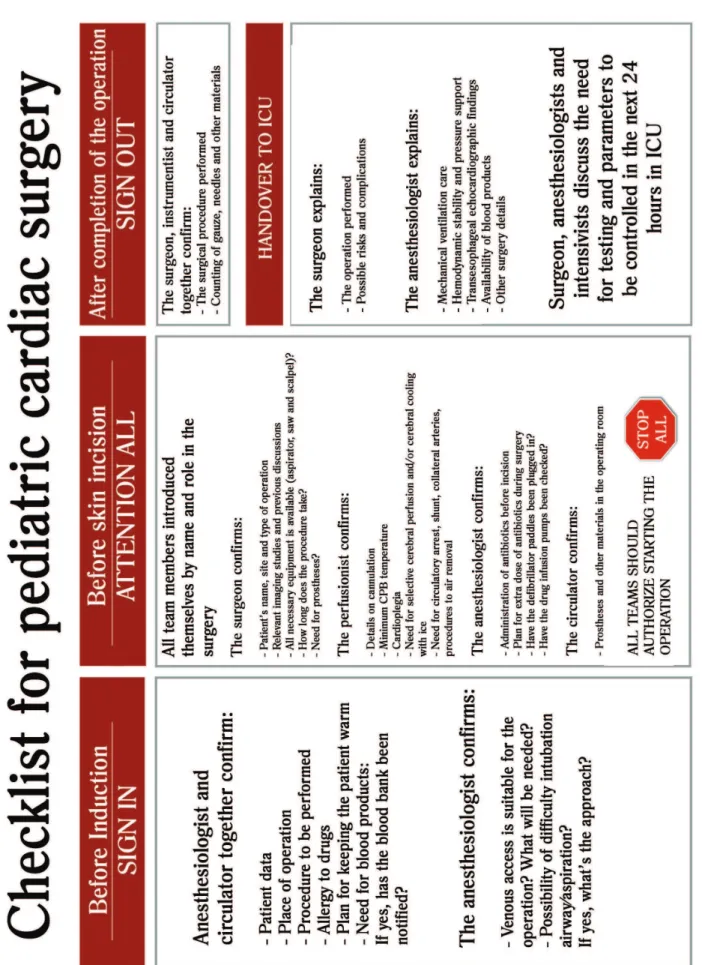
The checklist is basically divided into four parts: before induction of anesthesia, before skin incision, after the operation and during the passage of the operation performed to the ICU team (Figure 1).
PART I - PRIOR TO INDUCTION
The anesthesiologist and circulating nurse confirm together the patient data, the site of operation, the procedure to be performed, drug allergies, plan to keep the patient warm and the need for blood in the operating room. The anesthesiologist talks about intubation and venous access.
PART II - BEFORE THE SKIN INCISION
All team members present themselves by name and what role should play during the procedure.
The surgeon again confirms the patient’s name, location and type of operation. He explains the most important tests, verifies that all materials and equipment needed are available, time expected for the procedure and the need for prostheses. The perfusionist confirms details of cannulation, the minimum temperature during cardiopulmonary bypass, cardioplegia, need for circulatory arrest and other details necessary for adequate and safe perfusion, and may use a checklist of proper perfusion (Figure 2), different perfusion record should be completed during the procedure (Figure 3). The anesthesiologist confirms antibiotic administration and maintenance, the proper functioning of cardiac defibrillation paddles and drug infusion pumps.