jcoloproctol(rioj).2014;34(4):250–253
Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Original
article
Assessment
of
LIFT
(ligation
of
the
intersphincteric
fistula
tract)
technique
in
patients
with
perianal
transsphincteric
fistulas
Caroline
Sauter
Dalbem,
Sérgio
Danilo
Tanahara
Tomiyoshi,
Carlos
Henrique
Marques
dos
Santos
∗UniversidadeFederaldeMatoGrossodoSul(UFMS),CampoGrande,MS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26March2014 Accepted4September2014 Availableonline22October2014
Keywords:
Fistula Treatment Colorectalsurgery
a
b
s
t
r
a
c
t
PerianalfistulasarearelativelycommonconditioninProctologyoffices,rangingfrom sim-plecaseswitheasilypalpablesuperficialtractstocomplexproblemswithdeeptractsacross significantportionsoftheanalsphincter,whichsectioncanleadtovaryingdegreesof incontinenceduringafistulotomy.
Objective:ToevaluatetheeffectivenessoftheuseoftheLIFT(ligationoftheintersphincteric fistulatract)techniqueinpatientswithperianaltranssphinctericfistulas.
Method:Aprospectivestudyofpatientswithperianaltranssphinctericfistulawho under-wentLIFT.Patientswithperianalfistulasofcryptoglandulartranssphinctericoriginwithno previoussurgicalinterventionswereincludedinthestudy.Patientswithperianalfistulas fromanothersource,suchasCrohn’sdisease,tuberculosis,analcancerandrecurrent fistu-las,wereexcluded.Allpatientsunderwentthesameanesthetictechnique,withsubsequent surgicaltreatmentintwostages:setonplacementand,after6weeks,completionofLIFT.
Results:Weevaluated22patients;themeanagewas45.6years.Thepost-LIFToutpatient follow-uprangedfrom4to24monthswithameanfollow-upof14months.Thehealing timevariedfrom4to8weeksaftertheprocedure.Seventeenpatientswerecured(77%)and fiverelapsed(23%);however,allofthemexhibitedtheintersphincterictype,havingbeen treatedbyfistulotomyandalsoachievingcompletecure.Onefemalepatientdevelopedmild fecalincontinence.
Conclusion:The LIFT technique proved to be safe and effective in the treatment of transsphinctericperianalfistulas.
©2014SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](C.H.M.dosSantos).
http://dx.doi.org/10.1016/j.jcol.2014.09.001
jcoloproctol(rioj).2014;34(4):250–253
251
Avaliac¸ão
da
técnica
LIFT
(Ligation
of
the
Intersphincteric
Fistula
Tract)
em
pacientes
com
fístulas
perianais
transesfincterianas
Palavras-chave:
Fístula Tratamento Cirurgiacolorretal
r
e
s
u
m
o
Asfístulasperianaissãoumacondic¸ãorelativamentecomumemconsultóriode proctolo-gia,podendovariardesdecasossimples,comtrajetossuperficiaisfacilmentepalpáveis, atécasoscomplexos,comtrajetosprofundos,atravessandoporc¸õesconsideráveisdo apar-elhoesfincteriano,cujasecc¸ãopodelevaragrausvariáveisdeincontinênciaduranteuma fistulotomia.
Objetivo: AvaliaraefetividadedoempregodatécnicaLIFT(ligationoftheintersphincteric fistulatract)nospacientesportadoresdefístulasperianaistransesfincterianas.
Método: Estudoprospectivocompacientesportadoresdefístulaperianal transesfincteri-anasubmetidosàtécnicaLIFT.Foramincluídosnoestudopacientesportadoresdefistulas perianaisdeorigemcriptoglandulartransesfincterianasemintervenc¸õescirúrgicasprévias. Foramexcluídospacientesportadoresdefístulasperianaisdeoutraorigem,comodoenc¸ade Crohn,tuberculose,neoplasiaanalefístulasrecidivadas.Todosospacientesforam submeti-dosàmesmatécnicaanestésicaeposteriortratamentocirúrgicoemdoistempos:colocac¸ão desedenhoeapósseissemanasrealizac¸ãodeLIFT.
Resultados: Foramavaliados22pacientes;amédiadeidadeobservadafoide45,6anos.O seguimentoambulatorialpós-LIFTvarioude4a24meses,commédiadeacompanhamento de14meses.Otempodecicatrizac¸ãovarioude4a8semanaspós-procedimento.Dezessete pacientesficaramcurados(77%)ecincoapresentaramrecidiva(23%),porém,todosnaforma interesfincterianaeforamtratadosporfistulotomia,alcanc¸andotambémacuracompleta. Umapacienteevoluiucomincontinênciafecalleve.
Conclusão:AtécnicaLIFTdemonstrouserseguraeeficaznotratamentodasfístulasperianais transesfincterianas.
©2014SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Theoccurrenceofperianaldiseasedatesbackfromantiquity. For the treatment of anal fistulas, Hippocrates recom-mended,amongotherprocedures,cauterizingandanodizing the fistula – which can be understood today as seton application.1
Overthe years,various studies and surgicaltechniques havebeendevelopedwiththeaimtofindthemostappropriate treatmentforthisdisease,whichhasanincidenceof1/10,000 inhabitantsperyearandrepresents5%ofallColoproctology officevisits.2,3
These defects are distributed in the following propor-tion,usingtheclassificationdescribedbyParksetal.(1976): intersphincteric(60–75%),transsphincteric(15–20%), supras-phincteric(5%)andextrasphincteric(1–3%)fistulas.2
Currently,thereislittledoubtastotheindicationof sur-gicaltreatmentasthebesttreatmentoption,andfistulotomy isthetechniqueofchoiceforthevastmajorityofcases. How-ever,morecomplexfistulae, whentreatedsimilarly,canbe cured–butonlyattheexpense ofvaryingdegreesoffecal incontinence.
Thus,manyother techniqueshavebeen developedwith theaimtoachievethesamecurerateforfistulotomy,but with-outcausingfecalincontinenceincasesofgreatercomplexity. However,thereisstillnocleardefinitionofthebestoptionin thesecases.
In2007,Rojanasakuletal.4 described anewtherapeutic
optionforcaseslikethese,withverypromisinginitialresults. TheLIFT(ligation oftheintersphinctericfistulatract) tech-nique,asitbecameknown,hasshowngoodresultsalsoin otherstudies,5notinferiortotraditionaltechniques,andstill
havingasgreatmeritthefactof(theoretically)notcausing fecalincontinence,consideringthatnosectionofthe sphinc-teroccurs.Astherearestillfewstudiesonthesubject,theaim ofthisresearchistoevaluatetheresultsofLIFTinpatients withtranssphinctericperianalfistulas.
Method
ThestudywasapprovedbytheEthicsCommitteeonResearch oftheUniversidadeFederaldeMatoGrossodoSul.For inclu-sion,thepatientswereinformedbytheresearchteamonthe surgicaltechniqueusedandonthepossiblecomplicationsof thesurgery;andagreedtoparticipateinthestudy,completing thefreeandinformedconsentterm.
252
jcoloproctol(rioj).2014;34(4):250–253Coloproctology,HospitalRegionaldeMatoGrossodoSul,and fromtheprivatepracticeofoneoftheauthors.
Thestudy was conducted from May 2012 toSeptember 2013. Patients with perianal fistulas from another source, individuals with Crohn’s disease,tuberculosis, anal cancer andwhohadrecurrentfistulaswereexcluded.Patientswith intersphincteric,suprasphinctericandextrasphincteric peri-analfistulaswerealsoexcluded.Allpatientswere operated under spinal blockwith morphine. The surgicaltreatment wasperformedintwostages: first,theidentification ofthe fistula,thusconfirmingatranssphincteric tract.Thefistula wasthenrepairedbyapplyingalatexseton.Theplacementof thesetonwasintendedtoinduceamoreconsistentfibrosis, makingthefistuloustractwelldefined.Thesecondstepwas performedafter6weeks:theremovalofthelatexseton, curet-tageofthetract,anopeningoftheskinapproximately1cm perpendiculartothe fistuloustractand dissectionbetween the internal and external sphincters, to the identification and repair of the fistula. Then a transfixing ligature with polyglactin zero and the section of the tract between the sphincterswereperformed,followed bythe introductionof aprobe toconfirm the closing ofthe segments ofthe fis-tuloustractandofskinclosure.Thecrypt(innerhole)was cauterizedwithelectrocauteryandtheexternaloswaskept open.
Thepostoperativefollow-upwasperformedinan outpa-tientcliniconthe15thdayandthenevery30daysuntilthe completehealingofthefistula.Thereafter,thevisitsoccurred bimonthlyorbeforethattime,ifnecessary.
Intheoutpatientfollow-up,perioperativeinfection, heal-ingtime,pain,recurrenceandfecalcontinencechangewere evaluated.
Results
During the study period, 41 patients with transsphinc-teric perianal fistulaswere selected, of which 22 met the inclusion and exclusion criteria and were kept in the study.
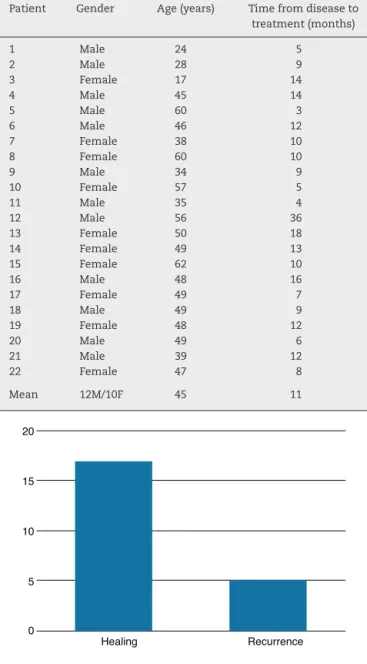
Ofthese22patients,12(55%)weremaleand10(45%)were female.Theagerangedfrom17to62years,withameanof45 years.Thetimeelapsedfromtheonsetofacomplaint com-patiblewithperianalfistulatothediagnosisrangedfrom3to 36months,withameanof11months(Table1).
Ineachcase,thepatientwasdischargedwithin24h.During theoutpatientfollow-up,localinfection(drainageofpusfrom surgicalwound)occurredinfivepatients(23%),whowereonly followedwithoutfurtherinterventionandwithspontaneous resolution.
Thepost-LIFT outpatientfollow-up rangedfrom 4to24 months,withameanfollow-up of14months.Thehealing timevariedfrom4to8weeksaftertheprocedure.
Seventeen(77%)patientsobtainedcompleteresolutionof their fistula with the technique adopted, while five (23%) relapsed.Ofthesefive,allhadarecurrenceintheformofan intersphinctericfistula,beingsubsequentlyoperatedby fis-tulotomy,with complete resolution– thus,athird surgical procedure. A female patient developed mild fecal inconti-nence(Fig.1).
Table1–Patientswithperianaltranssphinctericfistula treatedwithLIFTtechnique.
Patient Gender Age(years) Timefromdiseaseto treatment(months)
1 Male 24 5
2 Male 28 9
3 Female 17 14
4 Male 45 14
5 Male 60 3
6 Male 46 12
7 Female 38 10
8 Female 60 10
9 Male 34 9
10 Female 57 5
11 Male 35 4
12 Male 56 36
13 Female 50 18
14 Female 49 13
15 Female 62 10
16 Male 48 16
17 Female 49 7
18 Male 49 9
19 Female 48 12
20 Male 49 6
21 Male 39 12
22 Female 47 8
Mean 12M/10F 45 11
20
15
10
5
0
Healing Recurrence
Fig.1–AssessmentofprimaryhealingindexafterLIFTin thetreatmentofperianaltranssphinctericfistulas.
Discussion
Many studies on the LIFT surgical technique are still in progress;thisisstillconsideredanoveltechniqueforusein thetreatmentofperianalfistulas.
In the original publication describing the technique, Rojanasakulet al.4 appliedLIFT in18consecutive patients,
observingprimaryhealingin17ofthem.Thisresult encour-agedotherauthorstoevaluateLIFTinstudiesworldwide.
Inthisseriesofcases,aprimaryhealingrateof77%was observed. InAmerican studies that included patients who failedaprevioustreatment,thehealingraterangedfrom55 to 64%.6 In Australia, Ooiet al.,7 who alsoincludedin the
jcoloproctol(rioj).2014;34(4):250–253
253
other hand,Shanwanietal.5 reported curein82%oftheir
sample.Europeanstudiesshowedresolutionratesof71–83% forprimaryhealing,andinsomeofthemupto100% heal-inginthesample,inthosestudiesthatconsideredsecondary healingpatients.Thisdemonstratesthattheresultsobtained inthisstudywerewithintheexpected,accordingtothe avail-ableliterature,whichcanbeconsideredagoodoutcomefora stillrecenttechnique.6
Themeanfollow-upinthisserieswas14monthsandthe relapseratewas23%.InstudiesofYassinetal.6andLiuetal.8
themeanfollow-upwas19and28months,respectively,and therecurrenceratewas36%and32%,respectively. Possibly thelowerrelapseseen inthispaperisinferiortotheother studiespresentedhereduetoashorterfollow-up,although themostimportantpublicationsonLIFTdemonstratenolate recurrenceoffistulas.Whenrelapseoccurs,itisusuallyinthe firstweeks,afactalsoobservedinourfivepatientsinwhom recurrencewasobserved.
Thehealingtimeobservedinthisstudyrangedfrom4to8 weeks.Ooietal.7andShanwanietal.5reportedamean
heal-ingtimeof6and5weeks,respectively,i.e.,thesamemean hereobtained.Theoccurrenceofslightvariationsis proba-bleinaccordancewithwhatisconsideredas“healing”.Here, weconsideredas“completehealing”theinterruptionofthe flowofpurulentsecretionwithcoaptationoftheedgesofthe wound.
Intheliterature,dataarelackingforcomparisonwiththe resultspresentedherewithrespecttopostoperativeinfection, probablybecausethisanalysisisquitesubjective.Moreover, this analysisisless importantcompared withfistula heal-ingandthe evaluationofcontinence–parametersthatare effectivelyanalyzedbymostpublicationsonLIFT.
Although generally the results obtained in this study demonstratethatLIFTisaverypromisingtechnique,inline withdatafromtheliterature,weconsiderasbeingquite dis-turbingtheobservationoffecalincontinenceinoneofour patients, bybeing ayoung woman withno other risk fac-tors for this condition. Considering that one of the main expectedadvantagesofthe techniqueisaloworzero pos-sibilityofanimpairedsphincterfunction(sincethereisno sectionofthesphincter),thisresultwasquitesurprising.That patienthasbeentreatedwithpelvicfloorphysicaltherapy, withimprovement.NoAmerican, Asianor Oceanian study reported damage to the sphincter function. However, in a reviewconductedbyYassinet al.,6 it wasobservedthat in
11%oftheirsampletherewassomesortofchangein con-tinence.Thismaybeassociatedwiththeinclusionofpatients withrecurrentperianalfistulawhohadgonethroughprevious treatments.
Ofthefivepatientswhodidnotachieveaprimaryhealing inthisstudy,allshowedrecurrenceintheincisionforligation ofthefistuloustract,i.e.,theirdefectsturnedinto intersphinc-tericfistulas,andcouldbesubsequentlytreatedbyfistulotomy withcompleteresolutionandwithnofecalincontinence.This developmenthasalreadybeenreportedbyothersandcanbe consideredanadvantageofthemethod,whichenablesa pri-marycureinmostcases,but,whenthisdoesnotoccur,atleast reducesthecomplexityofthefistuloustract.6–9
Conclusion
TheLIFTtechniquewaseffectiveinthetreatmentofperianal transsphinctericfistulas.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.Ahistóriadacoloproctologia[Internet].Availablefrom:
http://www.procto.net.br/page.html[accessed02.04.12]. 2.SobradoCW,NahasSC,MarquesCFS.FístulasAnorretais.In:
RodriguesJJG,MachadoMCC,RasslanS,editors.Clínica Cirúrgica,1.Barueri-SP:EditoraManole;2008.p.997–1007.
3.RochaJJR.ProcessosInfecciososPerianais,Abscessos Perianais,FístulasPerianaiseGangrenaperineal[Internet]. Availablefrom:http://www.fmrp.usp.br/cg/novo/images/ pdf/conteudodisciplinas/processosinfecciosos[accessed 30.03.12].
4.RojanasakulA,PattanaarunJ,SahakitrungruangC.Totalanal sphinctersavingtechniqueforfistula-in-ano;theligationof intersphinctericfistulatract.JMedAssocThai.2007;90:581–6.
5.ShanwaniAMS,NorAM,AmriNMK.Theligationofthe intesphinctericfistulatract(LIFT):asphincter-saving techniqueforfistula-in-ano.DisColonRectum.2010;53:39–42.
6.YassinNA,HammondTM,LunnissPJ,PhillipsRK.Ligationof theintersphinctericfistulatractinthemanagementofanal fistula.Asystematicreview.ColorectalDis.2013;15:527–35.
7.OoiK,SkinnerI,CroxfordM,FaragherI,McLaughlinS. Managingfistula-in-anowithligationoftheintersphincteric fistulatractprocedure:theWesternHospitalexperience. ColorectalDis.2012;14:599–603.
8.LiuWY,AboulianA,KajiAH,KumarRR.Long-termresultsof ligationofintersphinctericfistulatract(LIFT)forfistula-in-ano. DisColonRectum.2013;56:343–7.
9.VanOnkelenRS,GosselinkMP,SchoutenWR.Ligationofthe intersphinctericfistulatractinlowtranssphinctericfistulae:a newtechniquetoavoidfistulotomy.ColorectDis.