w w w . r b o . o r g . b r
Case
Report
Sternoclavicular
dislocation:
case
report
and
surgical
technique
夽
Bernardo
Barcellos
Terra
∗,
Leandro
Marano
Rodrigues,
David
Victoria
Hoffmann
Pádua,
Marcelo
Giovanini
Martins,
João
Carlos
de
Medeiros
Teixeira,
Anderson
De
Nadai
HospitalSantaCasadeMisericórdiadeVitória,Vitória,ES,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29June2014 Accepted29July2014 Availableonline10July2015
Keywords:
Dislocation Tendontransfer Shoulder
a
b
s
t
r
a
c
t
Sternoclaviculardislocationsaccountforlessthan5%ofalldislocationsofthescapularbelt. Mostcasesofanteriordislocationofthesternoclavicularjointdonotpresentsymptoms. However,somepatientsmaydevelopchronicanteriorinstabilityandremainsymptomatic, andsurgicaltreatmentisindicatedinthesecases.Thereisascarcityofreportsinthe liter-aturerelatingtoreconstructionusingthelongpalmartendonincasesoftraumaticanterior instability.Althoughrare,theseinjuriesdeserverapiddiagnosisandefficienttreatmentin ordertoavoidfuturecomplications.Theaimofthisreportwastoreportonacaseofa motocrosscompetitorwhodevelopedchronictraumaticanteriorinstabilityofthe stern-oclavicularjointandunderwentsurgicalreconstructionusingtheautogenouslongpalmar tendon.
Thepatientwasa33-year-oldmanwithahistoryofanteriordislocationofthe sternoclav-icularsubsequenttoafallduringamaneuverinamotocrosscompetition.Conservative treatmentwasinstitutedinitially,consistingofuseofafunctionalslingtotreatthe symp-tomsfor3weeks,alongwithphysiotherapeuticrehabilitationfor3months.Wechosetouse amodificationofthe“figureofeight”techniquebasedonthestudiesbySpencerandKuhn. Alongitudinalincisionofapproximately10cmwasmadeatthelevelofthesternoclavicular joint.Thegraftfromtheipsilaterallongpalmartendonwaspassedthroughtheorificesin theformofamodified“figureofeight”anditsendsweresuturedtogether.Thepatientwas immobilizedusinganAmericanslingfor4weeks.After6monthsoffollow-up,thepatient nolongerpresentedpainorinstabilitywhenmovementofthesternoclavicularjointwas required.Minordiscomfortandslightprominenceofthesternoclavicularjointcontinued tobepresentbutdidnotaffectthepatient’sactivities.Thus,thepatientwasabletoreturn toracing6monthsaftertheoperation.Ourstudypresentedacaseofchronicanterior dis-locationofthesternoclavicularjointthatwassuccessfullytreatedbyusingamodification ofthe“figureofeight”reconstructiontechnique.Thistechniquewasshowntobesafeand effective,anditallowedthepatienttofullyreturntohissportsactivities.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedintheDepartmentofOrthopedicsandTraumatology,HospitalSantaCasadeMisericórdiadeVitória,Vitória,ES, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](B.B.Terra). http://dx.doi.org/10.1016/j.rboe.2015.06.019
tratamentoeficazparaevitarcomplicac¸õesfuturas.Oobjetivodestetrabalhofoirelatarum casodeumatletademotocrossqueevoluiucominstabilidadeanteriortraumáticacrônica da articulac¸ãoesternoclavicularefoisubmetidoareconstruc¸ãocirúrgicacomousodo tendãopalmarlongoautógeno.
Pacientemasculino,33anos,comhistóriadeluxac¸ãoanteriordaarticulac¸ão estern-oclavicularapósquedadurantemanobraemumcampeonatodemotocross.Inicialmente foiempregadootratamentoconservador,comusodetipoiafuncionalportrêssemanas,e sintomático,alémdareabilitac¸ãocomfisioterapiaportrêsmeses.Optamosporusaruma modificac¸ãodatécnicado“oito”,baseadosnosestudosdeSpencereKuhn.Aincisão lon-gitudinaldeaproximadamente10cmfoifeitanoníveldaarticulac¸ãoesternoclavicular.O enxertodotendãopalmarlongoipsilateralfoipassadopelosorifíciosemformade“oito” modificadoesuasextremidadesforamsuturadasconjuntamente.Opacientefoi imobi-lizadocomtipoiaamericanaporquatrosemanas.Nofimdeseismesesdeseguimentonão apresentavadorouinstabilidadequandosolicitadaaarticulac¸ãoesternoclavicular.Um dis-cretodesconfortoeligeirasaliênciadaarticulac¸ãoesternoclavicularpermaneceu,masnão afetaramsuasatividades,oquepermitiuaopacientevoltaràspistasdecorridacomseis mesesdepós-operatório.Nossoestudoapresentouumcasodeluxac¸ãoanteriorcrônicada articulac¸ãoesternoclaviculartratadocomsucessocomousodeumamodificac¸ãodatécnica dereconstruc¸ãoem“oito”.Essatécnicamostrouserseguraeeficazepermitiuumretorno totalàsatividadesesportivasdopaciente.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Sternoclaviculardislocationsaccountforfewerthan5%ofall dislocationsofthescapularbelt.Mostcasesofanterior dislo-cationofthesternoclavicularjointdonotpresentsymptoms. However,somepatientsmaydevelopchronicanterior insta-bilityandmaycontinuetopresentsymptoms.Inthesecases, surgicaltreatmentisindicated.1–3
Thesternoclavicular jointis morecommonlydislocated anteriorly, given that the force required to dislocate the clavicleposteriorlyis50%greaterbecauseofthehigher resis-tance of the posterior joint capsule. Many techniques for reconstructingthesternoclavicularjointhavebeendescribed, such as intramedullary suturing, medial resection of the clavicle,fixationusingaplate,reinforcementusingthe sub-claviantendonandreinforcementusingthesemitendinosus tendon.4–6
Theliteraturerelatingtoreconstructionusingthelong pal-martendonincasesoftraumaticanteriorinstabilityissparse. Althoughrare,theselesionsdeservetobediagnosedrapidly withefficienttreatmentinordertoavoidfuturecomplications. The objective of this study was to report a case of a motocrosscompetitor who evolved withchronic traumatic
anterior instabilityof thesternoclavicular joint and under-went surgical reconstruction using the autogenous long palmartendon.
Case
report
Fig.1–Photographillustratingthechronicdislocationof
thesternoclavicularjointoftherightshoulder.Notethe
medialprominenceofthemiddlethirdoftheipsilateral
clavicle.
Surgical
technique
We chose to use a modification of the “figure of eight” technique,7 based on the studies by Spencer et al.,8,9 who
usedcadaverstocompare the resistanceofthreedifferent reconstruction techniques: reconstruction using the semi-tendinosus tendon in a “figure of eight”; reinforcement using the subclavian tendon; and reconstruction of the intramedullaryligament.Theyconcludedthatreconstruction ina“figureofeight”wasthetechniquethatwasmostresistant toanteriorsternoclaviculardislocation.
Generalanesthesia wasinduced withthe patientinthe dorsal decubitusposition withthetrunkinclinedat40◦. A longitudinalincisionof10cmwasmadeatthelevel ofthe sternoclavicular joint. The joint was then completely dis-located anteriorlyin order to separate out the disk ofthe clavicle.Thejointspaceandtheadjacenttissueswerefilled
Fig.2–Radiographinserendipityview,onwhichanterior
displacementoftherightsternoclavicularjointcanbeseen.
Fig.3–Imagefromcomputedtomographywith3D
reconstruction,showingthedisplacementofthe
sternoclavicularjointandbonefragments.
withscartissueandtheanteriorandposterior sternoclavicu-larligamentandthecostoclavicularligamenthadbeentorn. Thescar tissuewas removedand subtle subperiosteal dis-section ofthe proximalclaviclewas performedin orderto avoid damagetothe brachiocephalic trunkand other pos-terior structures.This restored the mobility ofthe clavicle and enabled reduction. Weremoved a 20cm lengthof the ipsilateral long palmar tendon (Fig. 6) and performed the repair bymeans ofaKrakow suture, usinghigh-resistance polyethylenethread.Two3.5mmtunnels(anterosuperiorand anteroinferior)weremadeattheproximalendoftheclavicle andsternum,15mmfromthejointface.Theholeswereput into communicationintheintramedullaryregionand were broughttotheexteriorthroughthejointfaceonbothsides. Thegraftwaspassedthroughtheorificesinamodifiedfigure ofeightanditsendsweresuturedtogether(Figs.7and8).The stabilityofthesternoclavicularjointwasthentestedthrough shouldermovementsandmaximumextensionwasavoided.
Postoperative
period
ThepatientwasimmobilizedbymeansofanAmericansling for4weeks.Afterthisperiod,theslingwaswithdrawnand active movementswere allowed. After8weeks, aprogram ofmusclestrengtheningandexercisesagainstresistancewas started.
Attheendof6monthsoffollow-up,thepatientdidnot present anypainor instabilitywhenuseofthe sternoclav-icularjointwasrequired(Fig.9).Milddiscomfortandslight prominenceofthesternoclavicularjointremained,butthese did notaffectthe patient’s activities. Thus,hewas ableto returntohisracingactivities6monthsaftertheoperation.
Discussion
Fig.4–Imagefromcomputedtomographywith3Dreconstruction(viewfromabove),showingthedisplacementofthe
sternoclavicularjoint.
andimprovementofhissymptoms,includingtheuncommon difficultyinswallowingthathepresented.
Themajorityofthecasesofanteriordislocationofthe ster-noclavicularjointaretreatedconservatively.However,these injuriesmayoftenevolvetochronicinstability.Noadditional treatmentshouldbeappliedifthepatientdoesnotcomplain ofpainordiscomfort(rareincasesofanteriordislocation).10,11
Eachcaseneedstobecarefullyevaluated,inorderto differ-entiatechronicdislocationfromchronicinstability.Surgical interventions may be beneficial for patients with chronic anteriordislocationofthesternoclavicularjointwhopresent instability,discomfortorpain.3
Studies have shown good functional results from using autologousgrafts from the long palmar tendon for recon-structionofthesternoclavicularjoint.12–14Thistechniqueis
Fig.5–Imagefromcomputedtomographywith3D
reconstruction(viewfrombelow),showingthe
displacementofthesternoclavicularjoint.
biologicalandthereforesubjecttofewercomplicationsthan ifplatesandotherimplantsareused.Evenifplatesproduce goodresults,theymaycausethecomplicationsthatare inher-enttonon-biologicalimplants,alongwiththepossibleneed fortheirremoval.Useofallograftsalsoleadstotheriskof infection.Wechosetousethelongpalmartendonbecause thispresentslowmorbidityatthedonorsite,andisalsoeasily removed.Weareawarethatthelongpalmartendonisabsent inaround30%ofindividuals,andoursecondchoicewouldbe thesemitendinosus.
Several techniques forreconstructing the sternoclavicu-larjointhavebeenintroduced,includingfixationwithplates, fixationwithanchors,fixationofthecapsuleandjointdisk, reconstruction in a “figureof eight” using agraft from an autologous tendon and reconstruction using a graft from
Fig.6–Autologousgraftfromtheipsilaterallongpalmar
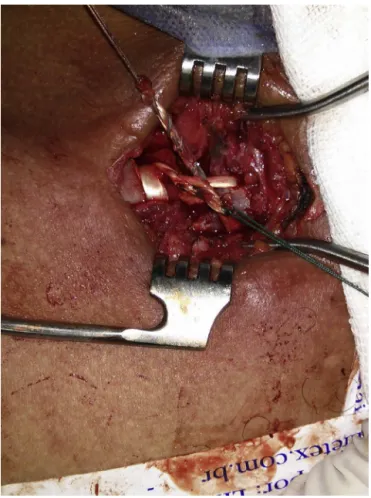
Fig.7–Intraoperativeviewshowingthepassageofthe
tendonthroughthebonetunnelsatthemedialendofthe
clavicleandthejointendofthesternum.
thesternocleidomastoidfascia.1,4,15Resectionofthemedial
portion of the clavicle has also been reported. The ideal treatmentstillremainsunknown,giventhatfewstudieshave presentedlong-termresults.Friedrichetal.15 reportedgood
clinicalresultsthroughusingtheautologousgracilistendon as the graft in “figure of eight” reconstruction for a case
Fig.8–Afterjointreduction,withthegraftboundup.
Fig.9–Sixmonthsaftertheoperation,showinggood
reductionoftherightsternoclavicularjoint.The
prominenceoftherightclaviclecannolongerbeseen.
of chronic anterosuperior sternoclavicular dislocation. Bae etal.1reportedthatgoodstabilizationwasachievedinnine
patients who underwent reconstruction of the sternoclav-icular joint withthe graft interlaced ina “figureof eight”, through predrilled tunnels. Few studies have reported any advantagefrom “figureofeight” reconstruction,inrelation toprimary stability. Spencerand Kuhn9 conducteda study
using cadavers with the aim of comparing the resistance ofthreedifferentreconstructiontechniques:reconstruction usingthesemitendinosustendonina“figureofeight”; rein-forcementusingthesubclaviantendon;andreconstructionof theintramedullaryligament.Theyconcludedthat reconstruc-tionina“figureofeight”wasthemostresistanttechniquefor casesofanteriorsternoclaviculardislocation.Furthermore,a recentsystematicreviewofclinicalreportsshowedthatthe reconstructiontechniqueinvolvingatendongraftina“figure ofeight”wasmoreresistantthanothertechniquesfortreating chronicinstabilityofthesternoclavicularjoint.
Theautologousgraftscommonlyusedinreconstructions ofthesternoclavicularjointarethegracilis,semitendinosus, longpalmarandplantartendons.12,14,15Autologousgraftsare
usedinordertoavoidtherisksofinfectionandtofacilitate tis-sueintegration,withtheaimofobtainingapositiveresultover thelongterm.Amongautologousgrafts,webelievethatthe gracilistendonandthelongpalmartendon(whichweused) aretheidealgrafts,sincetheirdiameterresultsinlower mor-bidity.Themedium-termresultsfromourpatientconfirmed thesefindings,giventhattherewasnomorbidityinthedonor area.
Onepotentiallydangerousstepinourtechniquewasthe drillingofthetunnelsinthesternumandclavicular,because oftheriskofinjuringprimestructuresthatareposteriorto this.10Therefore,theexitpointsinthesternumandclavicle
needtobeprotectedthroughusingaspacer,soastoavoidthis typeofinjury.
Conclusion
resultsofsurgicalmanagement.JPediatrOrthop. 2006;26(1):71–4.
2. RockwoodCAJr,GrohGI,WirthMA,GrassiFA.Resection arthroplastyofthesternoclavicularjoint.JBoneJointSurg Am.1997;79(3):387–93.
3. GrohGI,WirthMA,RockwoodCAJr.Treatmentoftraumatic posteriorsternoclaviculardislocations.JShoulderElbowSurg. 2011;20(1):107–13.
4. AbiddinZ,SinopidisC,GrocockCJ,YinQ,FrostickSP.Suture anchorsfortreatmentofsternoclavicularjointinstability.J ShoulderElbowSurg.2006;15(3):315–8.
5. ArmstrongAL,DiasJJ.Reconstructionforinstabilityofthe sternoclavicularjointusingthetendonofthe
sternocleidomastoidmuscle.JBoneJointSurgBr. 2008;90(5):610–3.
6. SingerG,FerlicP,KrausT,EberlR.Reconstructionofthe sternoclavicularjointinactivepatientswiththe
figure-of-eighttechniqueusinghamstrings.JShoulderElbow Surg.2013;22(1):64–9.
7. KawaguchiK,TanakaS,YoshitomiH,NagaiI,SatoW,Karita T,etal.Doublefigure-of-eightreconstructiontechniquefor
medium-termtolong-termfollow-upresults.JShoulder ElbowSurg.2014;23(2):245–50.
11.DeJongKP,SukulDM.Anteriorsternoclaviculardislocation: along-termfollow-upstudy.JOrthopTrauma.1990;4(4): 420–3.
12.EskolaA,VainionpääS,VastamäkiM,SlätisP,RokkanenP. Operationforoldsternoclaviculardislocation.Resultsin12 cases.JBoneJointSurgBr.1989;71(1):63–5.
13.EskolaA.Sternoclaviculardislocation.Apleaforopen treatment.ActaOrthopScand.1986;57(3):227–8.
14.CastropilW,RamadanLB,BitarAC,SchorB,DeOliveiraD’Elia C.Sternoclaviculardislocation–reconstructionwith semitendinosustendonautograft:acasereport.KneeSurg SportsTraumatolArthrosc.2008;16(9):865–8.