r e v b r a s o r t o p . 2017;52(1):61–68
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Clinical
evaluation
of
arthroscopic
treatment
of
shoulder
adhesive
capsulitis
夽
Alberto
Naoki
Miyazaki,
Pedro
Doneux
Santos,
Luciana
Andrade
Silva
∗,
Guilherme
do
Val
Sella,
Leonardo
Carrenho,
Sergio
Luiz
Checchia
FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),DepartamentodeOrtopediaeTraumatologia,GrupodeCirurgia doOmbroeCotovelo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29October2015 Accepted11April2016
Availableonline20December2016
Keywords:
Shoulderpain Arthroscopy Bursitis
a
b
s
t
r
a
c
t
Objective:Toevaluatetheresultsofarthroscopicreleasesperformedinpatientswith adhe-sivecapsulitisrefractorytoconservativetreatment.
Methods:Thiswasaretrospectivestudy,conductedbetween1996and2012,whichincluded 56shoulders(52patients)thatunderwentsurgery;38werefemale,and28hadthe domi-nantsideaffected.Themeanagewas51(29–73)years.Themeanfollow-upwas65(12–168) monthsandthemeanpreoperativetimewas8.9(2–24)months.AccordingtoZukermann’s classification,23caseswereconsideredprimaryand33secondary.Withthepatientinthe lateraldecubitusposition,circumferentialreleaseofthejointcapsulewasperformed:joint debridement;rotatorintervalopening;coracohumeralligamentrelease;anterior,posterior, inferior,andfinallyantero-inferiorcapsulotomy.Asubscapularistenotomywasperformed whennecessary.Allpatientsunderwentintensephysicaltherapyintheimmediate post-operativeperiod.In33shoulders,aninterscalenecatheterwasimplantedforanesthetic infusion.FunctionalresultswereevaluatedbytheUCLAcriteria.
Results:Improvedrangeofmotionwasobserved:meanincreaseof45◦ofelevation,41◦of externalrotationandeightvertebrallevelsofmedialrotation.AccordingtotheUCLAscore excellentresultswereobtainedin25(45%)patients;good,in24(45%);fair,intwo(3%);and poor,intwo(7%).Patientswhohadundergoneinferiorcapsulotomyachievedbetterresults. Only8.8%ofpatientswhousedtheanestheticinfusioncatheterunderwentpostoperative manipulation.Sevenpatientshadcomplications.
Conclusion: Therewasimprovementinpainandrangeofmotion.Inferiorcapsulotomyleads tobetterresults.Theuseoftheinterscaleneinfusioncatheterreducesthenumberof re-approaches.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),DepartamentodeOrtopediae Trau-matologia,GrupodeCirurgiadoOmbroeCotovelo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.A.Silva). http://dx.doi.org/10.1016/j.rboe.2016.12.004
62
rev bras ortop.2017;52(1):61–68Avaliac¸ão
dos
resultados
do
tratamento
artroscópico
da
capsulite
adesiva
do
ombro
Palavras-chave:
Dordeombro Artroscopia Bursite
r
e
s
u
m
o
Objetivo: Avaliarosresultadosdasliberac¸õesartroscópicasfeitasempacientescom cap-suliteadesivarefratáriaaotratamentoconservador.
Métodos: Trabalhoretrospectivofeitoentre1996e2012,com56ombros(52pacientes) sub-metidosacirurgia;38eramdosexofemininoe28tinhamoladodominanteacometido. Amédiadeidadefoide51(29-73)anos.Oseguimentomédio,de65(12-168)meseseo tempomédiodepré-operatório,de8,9(2-24)meses.Pelaclassificac¸ãodeZukermann,23 casosforamconsideradosprimáriose33secundários.Comopacienteemdecúbitolateral, fizemosaliberac¸ãocircunferencialdacápsulaarticular:desbridamentoarticular,abertura dointervalorotador,liberac¸ãodoligamentocoracoumeral,capsulotomiaanterior, poste-rior,inferiorefinalmente,anteroinferior.Atenotomiadosubescapularfoifeitaquando necessária.Todosforamsubmetidosafisioterapiaintensanopós-operatórioimediato.Em 33ombrosfoiimplantadoocatéterinterescalênicoparainfusãodeanestésico.Os result-adosfuncionaisforamavaliadospeloscritériosdoescoredaUniversityofCaliforniaatLos Angeles(UCLA).
Resultados: Obtivemosmelhoriadoarcodemovimento:aumentomédiode45◦deelevac¸ão, 41◦derotac¸ãolateraleoitoníveisvertebraisderotac¸ãomedial.PeloescoredaUCLA,tivemos 25resultadosexcelentes(45%),25bons(45%),doisrazoáveis(3%)equatroruins(7%).Os pacientesquefizeramcapsulotomiainferiorevoluírammelhordoqueosquenãofizeram. Apenas8,8%dospacientesqueusaramcateterdeinfusãoanestésicoforamsubmetidosa manipulac¸ãonopós-operatório.Setepacientesapresentaramcomplicac¸ões.
Conclusão: Houvemelhoriadadoredoarcodemovimento.Acapsulotomiainferiorleva amelhoresresultados.Ousodocatéterinterescalênicodeinfusãoanestésicadiminuio númerodereabordagens.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theterm“adhesivecapsulitis”wasfirstdescribedbyNeviaser in1945,asaninflammatorydiseaseoftheshoulderjoint cap-sulethatdevelopswithcontractureandresultsinstiffness andpain.1
Treatment aims to control pain and recover range of motion. Initially, treatment is conservative, especially in the acute phase2,3; there are several therapeutic options,
suchasphysicaltherapy,corticosteroidsand/ornon-steroidal anti-inflammatorydrugs(NSAIDs),andsuprascapularnerve blocks.4–7 Inreview articles,Checchia etal.7 and Robinson
etal.5demonstratedgoodresultswhentreatingpatientswith
physical therapy associated with anti-inflammatory drugs (hormonalandnon-hormonal)andserialsuprascapularnerve blocks.
Invasivetreatmentisindicatedincaseoffailureof con-servativetreatmentconductedforaminimumperiodofsix months;however, accordingtotheliteraturereviewed,this intervalmayrangefromsixweeksto12months.8–13
Proce-duresdescribedasinvasiveincludehydraulicdistentionofthe capsule(theliteraturedifferonitseffectivenessduetohigh recurrencerates),jointmanipulationunderanesthesia,and capsularrelease,whichcanbedonethroughopenor arthro-scopicsurgery.4–6,14
Joint manipulation under anesthesia, which was once widelyused,iscurrentlybeingdiscontinuedduetoits com-plications: fractures, glenoid labrum injuries, neurapraxis, rotatorcufftear,andpersistentpain.14–17
One of the first descriptions of the surgical technique for shoulder release through the open access route was made by Ozaki et al.,18 who advocated resection of the
coracohumeral ligament and opening of the rotator inter-val. Literature shows that open surgery presents good results, but adds a greater morbidity than arthroscopy: it is difficult to release the posterior capsule and the intraoperative bleeding is greater, as well as postoperative pain, whichextendshospitalstay;furthermore, itis neces-sary to restrictmovements untilthe subscapularistendon heals.4,5,8,14,19
Recentstudieshaveshownexcellentresults,bothinterms of pain relief and range ofmotion gain,with arthroscopic releaseofadhesivecapsulitis.Itiscurrentlyconsideredtobe a reproduciblemethod, whichenables betteraccessto the entirejointcapsuleoftheshoulderwithlowratesof com-plications, sincethe release isdone graduallyunderdirect visionthroughaminimallyinvasivemethod,which nonethe-lessrequirespropertraining.8–11,19–21Literaturementionsas
complicationsofthisproceduretheriskofiatrogenicinjury to the axillary nerve,22 chondral lesion due to the
rev bras ortop.2017;52(1):61–68
63
chondrolysisduetothermalinjurycausedbytheuseof intra-articularradiofrequency.23
Thisstudy aimedtoevaluatethe resultsofarthroscopic releasesperformedinthisdepartmentinpatientswith adhe-sivecapsulitisrefractorytoconservativetreatment.
Material
and
methods
Thisstudyretrospectivelyanalyzed56shouldersof52patients who underwent arthroscopic release due to adhesive cap-sulitisrefractoryto conservative treatment. Surgerieswere performedbetweenFebruary1996andMay2012bythe Shoul-derandElbowGroupoftheSantaCasadeSãoPauloSchoolof MedicalSciences–FernandinhoSimonsenPavilion.
Patientswithadhesivecapsulitisrefractorytoconservative treatment,withaminimumfollow-upperiodofoneyear,with nootherabnormalitiesthatcouldjustifythelossofrangeof motion(osteoarthritis, malunion,andnecrosis,among oth-ers)wereincluded.Theclinicalandepidemiologicaldataare showninTable1.
Patients underwent conservative treatment for a mean periodof8.9months(2–24).Mostofthem(66%)weretreated withserialsuprascapularnerveblocksassociatedwith physio-therapy,withameanof12.2blocks.2–23Surgerywasindicated
whentherewasnoresponsetoconservativetreatment,i.e., therewasimprovementinpain but patientremained with limitedjointmobility,whichhinderedtheirday-to-day activ-ities or even work activities. It was also indicated when patientcouldnotattendtheofficewiththeregularityneeded forundergoingblocks,thatis,every15daysuntilcomplete improvementofthecondition,whichtakessevenmonths,on average.7
Meanpostoperativefollow-upwas65months(12–168)and patients’ age ranged from 29 to 73 years (mean 51.2); 38 patientswere female (73%) and 14 male(27%). In 28 (54%) patients,thedominantlimbunderwentarthroscopicrelease; infourpatients(threefemaleandonemale),involvementwas bilateralandbothshouldersweresubjectedtothisprocedure (8%).
Regardingtheetiology,23shoulderswereclassified accord-ing toZuckermanand Rokito24 asprimary capsulitis (41%)
and33assecondary(59%),20ofsystemicorigin.Ofthese,15 patientswerediabetic(29%oftotal),12hadintrinsiccauses (92.3%),andonehadextrinsiccauses(3.7%).
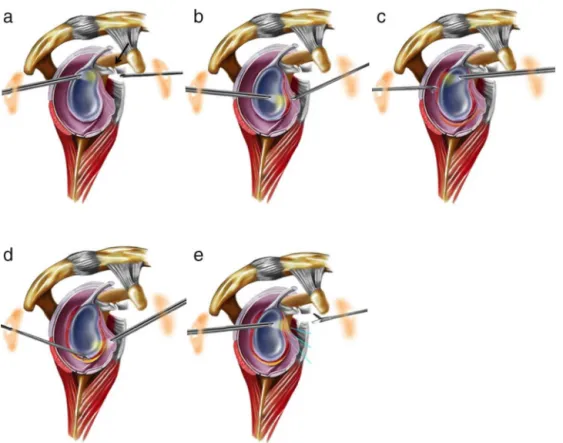
Patients underwent several arthroscopic procedures, whichvariedaccordingtotheneedandimprovementofthe surgicaltechnique,asshowninTable2.Withthepatient pos-itionedinlateraldecubitus,thefollowingstepsweretaken: through the anterior portal, joint debridement was made, therotatorintervalwasopened,thecoracohumeralligament wasreleased, and aninterior capsulotomywasperformed. Then,portalwaschanged.Throughtheposteriorportal, pos-teriorand inferiorcapsulotomies weremade. Finally,again through the anteriorportal, an anteroinferior capsulotomy was made with the aid of a basket-type forceps to avoid axillarynerveinjury.Attheendoftheseprocedures, circum-ferentialrelease of the joint capsulewas achieved. Lateral rotationwasclinicallyassessed;ifthegain wasconsidered
tobeinsufficient,apartialtenotomyofthesubscapulariswas made(Fig.1).
Fromthefirstdaypost-operativeonwards,patientswere subjectedtoanintensivephysicaltherapyworkwithpotent analgesia. An interscalene catheter was used in 33 shoul-ders(59%)foranesthesiainfusion(bupivacaine).Atdischarge, thecatheterwasremovedandpatientwasreferredfor out-patient physiotherapy sessions and received guidelines for performing capsular stretching exercisesathome. Patients werehospitalizedanaverageoffourdays.Inthefirstweeks, patientswereinstructed toattend4–5therapysessions per week; this schedule was modified according to patient’s improvement. On average, patients attended 53.4 sessions (12–139).
Theshoulder functional analysis criteriaby the Univer-sityofCaliforniaatLosAngeles(UCLA)25wasusedtoassess
thepresentresults;shoulderrangeofmotionwasmeasured accordingtothecriteriasetforthbytheAmericanAcademy ofOrthopedicSurgeons.26
For thestatistical analysis,the followingprogramswere used:SPSS(StatisticalPackageforSocialSciences)version17, Minitab16,andExcelOffice2010,andthefollowingtestswere applied:ANOVA,Student’st-testforpairedsamples,equality oftwoproportions,andPearson’scorrelation.Toobtain the results,the95%confidenceintervalwasconsidered statisti-callysignificant(p<0.05).
Thisstudywasapprovedbythehospital’sethicscommittee underCAAENo.14412713.2.0000.5479.
Results
Patientspresentedanimprovedrangeofmotion.Mean pre-operativerangeofmotionwas96◦ofelevation,16◦oflateral rotation, andL5 medialrotation; afterarthroscopicrelease, meansbecame141◦ ofelevation,57◦ oflateralrotation,and T9medialrotation(p<0.001).
Whenpostoperativeresultswerecomparedwiththe con-tralaterallimb,excluding patientswho underwent bilateral arthroscopic release, a mean deficit of3◦ ofelevation was observed(p=0.03).
Regarding the procedures, patients undergoing inferior capsulotomyhad ameanof8◦ ofelevation(p=0.057,close tosignificancemargin),13◦oflateralrotation(p=0.003),four vertebrallevels(p=0.002),and3.2pointsintheUCLAscore (p=0.021)morethanthosepatientswhodidnotundergo infe-riorcapsulotomy.
Patientsundergoingpartialtenotomyofthesubscapularis (25%)had lower preoperativelateral rotation(p=0.010)and elevation(p=0.062).Themeanelevationforthisgroupwas86◦, andmeanlateralrotationwas5◦,whichwaslowerthanthe 99◦ofelevationand20◦oflateralrotationobservedinpatients whodidnotundergothisprocedure.
64
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
7;
5
2(1)
:61–68
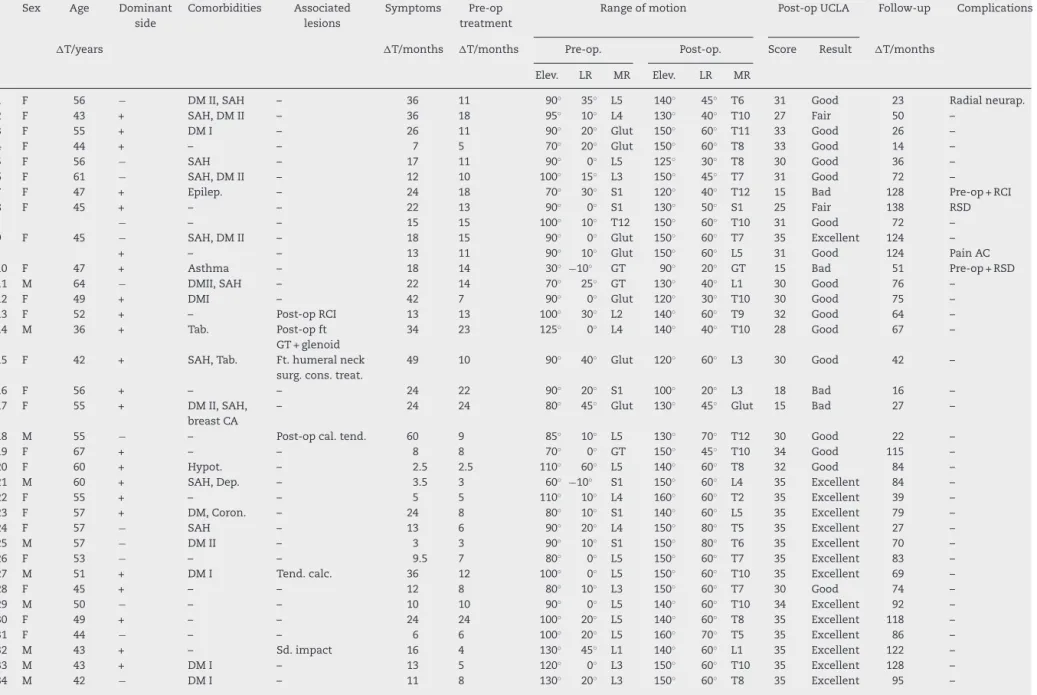
Table1–Patientclinicaldata.
Sex Age Dominant
side
Comorbidities Associated
lesions
Symptoms Pre-op
treatment
Rangeofmotion Post-opUCLA Follow-up Complications
T/years T/months T/months Pre-op. Post-op. Score Result T/months
Elev. LR MR Elev. LR MR
1 F 56 − DMII,SAH – 36 11 90◦ 35◦ L5 140◦ 45◦ T6 31 Good 23 Radialneurap.
2 F 43 + SAH,DMII – 36 18 95◦ 10◦ L4 130◦ 40◦ T10 27 Fair 50 –
3 F 55 + DMI – 26 11 90◦ 20◦ Glut 150◦ 60◦ T11 33 Good 26 –
4 F 44 + – – 7 5 70◦ 20◦ Glut 150◦ 60◦ T8 33 Good 14 –
5 F 56 − SAH – 17 11 90◦ 0◦ L5 125◦ 30◦ T8 30 Good 36 –
6 F 61 − SAH,DMII – 12 10 100◦ 15◦ L3 150◦ 45◦ T7 31 Good 72 –
7 F 47 + Epilep. – 24 18 70◦ 30◦ S1 120◦ 40◦ T12 15 Bad 128 Pre-op+RCI
8 F 45 + – – 22 13 90◦ 0◦ S1 130◦ 50◦ S1 25 Fair 138 RSD
− – – 15 15 100◦ 10◦ T12 150◦ 60◦ T10 31 Good 72 –
9 F 45 − SAH,DMII – 18 15 90◦ 0◦ Glut 150◦ 60◦ T7 35 Excellent 124 –
+ – – 13 11 90◦ 10◦ Glut 150◦ 60◦ L5 31 Good 124 PainAC
10 F 47 + Asthma – 18 14 30◦ −10◦ GT 90◦ 20◦ GT 15 Bad 51 Pre-op+RSD
11 M 64 − DMII,SAH – 22 14 70◦ 25◦ GT 130◦ 40◦ L1 30 Good 76 –
12 F 49 + DMI – 42 7 90◦ 0◦ Glut 120◦ 30◦ T10 30 Good 75 –
13 F 52 + – Post-opRCI 13 13 100◦ 30◦ L2 140◦ 60◦ T9 32 Good 64 –
14 M 36 + Tab. Post-opft
GT+glenoid
34 23 125◦ 0◦ L4 140◦ 40◦ T10 28 Good 67 –
15 F 42 + SAH,Tab. Ft.humeralneck
surg.cons.treat.
49 10 90◦ 40◦ Glut 120◦ 60◦ L3 30 Good 42 –
16 F 56 + – – 24 22 90◦ 20◦ S1 100◦ 20◦ L3 18 Bad 16 –
17 F 55 + DMII,SAH,
breastCA
– 24 24 80◦ 45◦ Glut 130◦ 45◦ Glut 15 Bad 27 –
18 M 55 − – Post-opcal.tend. 60 9 85◦ 10◦ L5 130◦ 70◦ T12 30 Good 22 –
19 F 67 + – – 8 8 70◦ 0◦ GT 150◦ 45◦ T10 34 Good 115 –
20 F 60 + Hypot. – 2.5 2.5 110◦ 60◦ L5 140◦ 60◦ T8 32 Good 84 –
21 M 60 + SAH,Dep. – 3.5 3 60◦ −10◦ S1 150◦ 60◦ L4 35 Excellent 84 –
22 F 55 + – – 5 5 110◦ 10◦ L4 160◦ 60◦ T2 35 Excellent 39 –
23 F 57 + DM,Coron. – 24 8 80◦ 10◦ S1 140◦ 60◦ L5 35 Excellent 79 –
24 F 57 − SAH – 13 6 90◦ 20◦ L4 150◦ 80◦ T5 35 Excellent 27 –
25 M 57 − DMII – 3 3 90◦ 10◦ S1 150◦ 80◦ T6 35 Excellent 70 –
26 F 53 − – – 9.5 7 80◦ 0◦ L5 150◦ 60◦ T7 35 Excellent 83 –
27 M 51 + DMI Tend.calc. 36 12 100◦ 0◦ L5 150◦ 60◦ T10 35 Excellent 69 –
28 F 45 + – – 12 8 80◦ 10◦ L3 150◦ 60◦ T7 30 Good 74 –
29 M 50 − – – 10 10 90◦ 0◦ L5 140◦ 60◦ T10 34 Excellent 92 –
30 F 49 + – – 24 24 100◦ 20◦ L5 140◦ 60◦ T8 35 Excellent 118 –
31 F 44 − – – 6 6 100◦ 20◦ L5 160◦ 70◦ T5 35 Excellent 86 –
32 M 43 + – Sd.impact 16 4 130◦ 45◦ L1 140◦ 60◦ L1 35 Excellent 122 –
33 M 43 + DMI – 13 5 120◦ 0◦ L3 150◦ 60◦ T10 35 Excellent 128 –
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
7;
5
2(1)
:61–68
65
Table1–(Continued)
Sex Age Dominant
side
Comorbidities Associated
lesions
Symptoms Pre-op
treatment
Rangeofmotion Post-opUCLA Follow-up Complications
T/years T/months T/months Pre-op. Post-op. Score Result T/months
Elev. LR MR Elev. LR MR
35 F 42 − – – 30 6 140◦ 45◦ T10 150◦ 60◦ T6 35 Excellent 70 –
36 M 29 − Tab. Ft.GT(cons.
treat.)
3 3 100◦ 10◦ L2 140◦ 30◦ T12 28 Good 168 –
37 F 35 − Hypot. – 5 3 80◦ 0◦ S1 160◦ 45◦ T5 35 Excellent 16 –
38 F 73 − SAH,DMII OsteoarthritisAC 4 3 130◦ 60◦ S1 140◦ 60◦ L4 34 Excellent 12 –
39 F 65 − – – 3 3 70◦ 0◦ S1 150◦ 70◦ T7 34 Excellent 25 Axillaryneurap.
40 M 58 + – – 5 5 120◦ 30◦ L4 140◦ 30◦ L1 32 Good 69 –
41 F 52 − Dep. – 4 4 40◦−20◦ Glut 160◦ 80◦ T5 34 Excellent 107 Radialneurap.
42 F 55 − Hypot. – 8 6 100◦−10◦ L4 150◦ 60◦ T6 33 Good 44 –
43 F 57 − DLP Tend.calc. 12 6 120◦ 45◦ L5 150◦ 70◦ T7 33 Good 14 –
44 F 56 + DLP – 12 8 120◦ 60◦ T12 160◦ 80◦ T3 35 Excellent 19 –
45 M 52 + SAH,Hypot. – 7 2 100◦ 20◦ L4 150◦ 80◦ T7 34 Excellent 85 –
M − SAH,Hypot. – 3 3 120◦ 30◦ L5 150◦ 80◦ T6 35 Excellent 54 –
46 F 51 − – Wristft.+imob. 8 6 90◦ 10◦ L2 150◦ 70◦ T5 35 Excellent 96 –
F + – – 6 2 130◦ 45◦ L3 140◦ 70◦ T6 34 Excellent 49 –
47 F 49 + – Sd.impact 6 2 150◦ 20◦ L4 140◦ 70◦ T5 32 Good 52 –
48 F 53 + Sd.Panic Cal.tend.ofthe
sub.
5 2 100◦ 10◦ L4 150◦ 70◦ T5 33 Good 72 –
49 F 48 − Tob. – 5 7 90◦ 0◦ L3 130◦ 70◦ T5 28 Good 14 –
50 M 46 + – Post-opSLAP 8 12 140◦ 45◦ T8 145◦ 70◦ T5 35 Excellent 19 –
51 F 51 + BreastCA Post-op
epiphysealft
12 12 90◦−10◦ Glut 130◦ 30◦ T9 29 Good 21 –
52 F 50 + DMI – 6 8 80◦ 0◦ Glut 110◦ 60◦ T10 30 Good 13 –
Means 51.2 15.3 8.9 96◦ 16◦ L5 141◦ 57◦ T9 31.4 64.8
Source:SantaCasadeSãoPauloArchives.
AC,acromioclavicularjoint;CA,cancer;dep.,depression;RSD,reflexsympatheticdystrophy;DLP,dyslipidemia;DM,diabetesmellitus;elev.,elevation;epilep.,epilepsy;F,female;ft.,fracture;glut,
gluteus;GT,greatertrochanterofthefemur;SAH,systemichypertension;hypot.,hypothyroidism;imob.,immobilization;RCI,rotatorcuffinjury;neurap.,neurapraxia;post-op.,post-operativeperiod;
pre-op.,pre-operativeperiod;LR,lateralrotation;MR,medialrotation;sd,syndrome;sub,subscapularistendon;tob,tobaccosmoker;cal.tend.,calcareoustendinitis.;GT,greatertuberosity;cons.
66
rev bras ortop.2017;52(1):61–68Fig.1–Surgicalstepsofthearthroscopicreleasefortreatingadhesivecapsulitis.Sagittalsectionoftheleftshoulder showing(a)releaseofcoracohumeralligament(arrow),(b)anteriorcapsulotomyperformedthroughtheanteriorportal,(c) posterosuperiorcapsulotomy,and(d)anteroinferiorcapsulotomy,alongtheaxillarynerve,withbothcapsulotomies performedusingtheposteriorportal,and(e)tenotomyofthesuperiorquarterofthesubscapularismuscletendon,again throughtheanteriorportal.
Table2–Proceduresperformedduringarthroscopy.
Procedures Numberofshoulders %
Openingoftherotatorinterval 56 100
Coracohumeralligamentrelease 55 98
Anteriorcapsulotomy 52 93
Posteriorcapsulotomy 44 78
Inferiorcapsulotomy 20 36
Subscapularistenotomy 14 25
Acromioplasty 24 43
Mumford 11 19
Calcareoustendinitisdrainage 2 3.5
Source:SantaCasadeSãoPauloArchives.
Nostatisticalsignificancewasobservedinrelationshipto theresultsandvariablesage,sex,andcomorbiditiesamong thediabeticandnon-diabeticpopulationsandbetween pri-maryandsecondarycapsulitis.
BasedontheresultsoftheUCLAcriteria,25 25shoulders
wereclassified asexcellent (45%),25asgood (45%),two as fair(3%),andfouraspoor(7%).Sevenpatientshad compli-cations(12.5%),including two withradialneurapraxia, one withaxillaryneurapraxia,tworeoperations,twocasesofreflex sympatheticdystrophy,onerotatorcuffinjury,andonecase ofacromioclavicularpain.
Discussion
Theprimarygoaloftreatmentofadhesivecapsulitisispain reliefandrestorationofrangeofmotionintheshortesttime possible.
Initialtreatmentshouldbeconservative,becausethe lit-eratureshowsthatphysicaltherapyassociatedwithadjuvant methodsyieldsgoodresults.Theminimumduration recom-mendedbymostauthorsissixmonths,butitcanvaryfromsix weeksto12months.5,8,9,12,13,27Inthepresentstudy,themean
timeofevolutiontosurgicalindicationwas8.9(2–24)months. Inthisservice,casesofadhesivecapsulitisaretreatedwith physicaltherapyassociatedwithserialsuprascapularnerve blocks,andarateof84%goodresultswasobservedinastudy bythepresentauthorspublishedin20067;37(66%)patientsin
thecurrentstudyunderwentthistreatmentwithameanof12 (range:2–23)nerveblocksuntilsurgicalindication.Itis note-worthythatthenerveblockisdoneonanoutpatientbasis,in aminimallyinvasivemanner;however,itmustbedone regu-larlyevery15daysanditsinitialanalgesiceffect,onaverage, startsafterthefourthblock.7Forthesereasons,manypatients
refusedtofollowthetreatmentandchosesurgery,despitethe initialguidanceforconservativetreatment.
rev bras ortop.2017;52(1):61–68
67
Gerberetal.19reportedagainof38◦ofelevationand18◦ oflateralrotation;Warneretal.,9anincreaseof49◦ of flex-ion,42◦oflateralrotation,andeightlevelsofspinalprocesses inmedialrotation;Cohenetal.,21anincreaseof64◦of flex-ion,43.5◦oflateralrotation,andeightlevelsinspinalmedial rotation;otherauthorshavealsoreportedgoodresults.8,12,13,20
Thepresentresultsshowedanimprovementintheelevation of45◦,38◦ oflateral rotation,and eightlevelsinthe spinal medialrotation, withafinalmeanrangeofmotionof141◦ ofelevation,57◦ ofmedialrotation,and9Tmedialrotation, resultsthatareinagreementwiththeliterature.
Mean elevation and lateral and medial rotation of the contralateral limb of these patients, excluding those who underwentbilateralrelease,were143◦, 56◦,and T9, respec-tively. Comparing mean postoperative elevation, excluding patientswho had bilateral release,adeficit ofonly3◦ was observed (p=0.030). This demonstrates that, albeit with a smalldeficit ofelevation, generallyit ispossibletorestore rangeofmotioninthesepatients.
Regardingtheproceduresperformedduringarthroscopic release,initialcaseswere limitedtoopeningofthe rotator interval,resection ofthe coracohumeral ligament,anterior andposteriorcapsularreleases,andafinaljointmanipulation forruptureoftheinferiorcapsule.Intheirstudy,Pollocketal.20
performedarthroscopyimmediatelyaftermanipulationofthe shoulderjointandfoundarateof30%ofinferiorcapsule rup-turefailurewiththisprocedure.Studiesofthearthroscopic anatomyoftheaxillarynerve10,28,29providedabetter
under-standing,allowing the development ofsafe techniques for inferiorcapsularrelease;therefore, circumferentialreleases havebecomestandardintheservice.The20(36%)patients whounderwentinferiorcapsulotomyhadbetterresults com-paredwithother patientsinthefinalmean elevation(146◦
vs.138◦,p=0.057),meanlateralrotation(65◦vs.52◦,p=0.003), meanmedialrotation(T7vs.T11,p=0.002),andmean post-operativeUCLAscore25(33.4vs.30.2,p=0.021).Theauthors
believethatcircumferentialcapsulotomyreducestherisksof complicationsassociatedwithjointmanipulation,aswellas therecurrencerate,restoringmorefunctionalrangeofmotion inashortertime.Asforthetenotomyofthesubscapularis,the procedurewasperformedintheintra-articularportionofthe tendonthatisvisualizedduringarthroscopy;itwasindicated duringsurgery,aftercompletecapsularrelease,whenitwas notpossibletoachievethesamelateralrotation(indegrees) asthecontralateralside.
Pollock et al.20 and Cinar et al.30 observed worse
out-comesindiabeticpatientswhencomparedwithnon-diabetic patients after arthroscopic release. In the present study, resultsofarthroscopictreatmentwere similarinthesetwo populations, with no statistical significance, both in rela-tionship to the range of motion and final UCLA,2 which
was inagreement withresults observed withconservative treatment.7Regardingfinalmeanrangeofmotion,diabetics
showedaslightlimitationinrelationtonon-diabeticpatients, withmeanpost-operativeelevation(p=0.551),lateralrotation (p=0.357),andmedialrotation(p=0.154)of140◦,54◦,andT11. Inturn,theseresultsinnon-diabeticswere142◦,58◦,andT9, respectively.RegardingthemeanUCLA,25itwas31.4forboth
groups(p=0.995),althoughnoneofthesedatawere statisti-callysignificant.
Another very important point inthe surgical treatment ofadhesivecapsulitisispostoperativerehabilitation.Physical therapyprotocol shouldbeinitiatedonthefirst postopera-tive day, in an intensive regimen associated with potent analgesia,inordertomaintainmovementgainachieved intra-operatively. Theuse ofinterscalenecatheter foranesthetic infusionintheearlypostoperativeperiodisrecommendedby someauthors.2,9,13Marianoetal.31concludedthatcontinuous
interscaleneblockissuperiortothesingleapplicationblock, providinggreaterpainrelief,minimizingtheuseofadditional opioids,improvingsleepquality,andincreasingpatient sat-isfactionaftershouldersurgery.Thisanalgesiafacilitatesthe physicaltherapyrehabilitationwork,thusleading toa bet-terresult.Inthepresentstudy,ofthe33shoulders(59%)in whichthiscatheterwasused,only8.8%patientsrequiredjoint manipulationduring thepostoperativefollow-up period:in onepatient,thecathetermovedoutoftheinterscalenespace andlostitsanalgesiceffectonthesecondpostoperativeday. Conversely,31.8%ofthoseinwhomthiscatheterwasnotused requiredjointmanipulationduetolossofmotioninthe post-operative follow-up, which provesthe effectivenessof this analgesiainpreventingrelapse(p=0.028).Thismanipulation isperformedwithinamaximumof30dayspostoperatively.
Complications were observed in seven patients: two patientsdevelopedradialneurapraxia,withreversalof symp-tomsafter2–3months.Thiscomplicationprobablyoriginated duringtheinterscaleneanestheticblock.Thispatientdidnot useinterscalenecatheterforanestheticinfusion.Onepatient developedaxillaryneurapraxiapostoperatively.Hepresented acompleterecoveryoffunctioninfourmonths.Thispatient didnotundergoinferiorcapsulotomy,butratherthe manipu-lationforinferiorcapsulerupture.Theauthorsbelievethat there was a probable traction of the axillary nerve during manipulation,causingsymptoms.Althoughmentionedasa possiblecomplicationofinferiorcapsulotomy,1 nocasesof
injuryorneurapraxiaofthisnervewereobservedinpatients whounderwentthisprocedure. Therefore,wecanconclude thatinferiorcapsulotomyisasafeprocedure,aslongasthe correctsurgicaltechniqueisperformed.
Regardingtheothercomplications,onepatienthad resid-ualpainintheacromioclavicularjoint(case9),two(cases8 and10)developedreflexsympatheticdystrophyinthe oper-ated limb, and one had a rotator cuff injury. This patient (case7)underwenttwoarthroscopicproceduresfortreatment of adhesive capsulitis with joint release; during follow-up aftersecondsurgery,asthepatientstillpresentedrangeof motionlimitation andpain, amagneticresonanceimaging examwasperformed,whichdisclosedrotatorcuffinjury.In thetwoprevioussurgicalprocedures,patienthadundergone joint manipulation tocomplement capsularrelease, which mayhavecontributedtothecauseofinjury.
Anotherpatient(case10)requiredreoperation,andawider capsularreleasewasperformed;nonetheless,patientstill pre-sented range of motion limitation and pain. In the initial surgery, joint access was difficultdue to the small articu-larspace,whicheventuallycompromisedtheprocedure:the releaseofthejointcapsulewasincomplete.Anotherpatient (case 16) had poor UCLAscore25 results; anosteochondral
68
rev bras ortop.2017;52(1):61–68Onepatient(case17),althoughtherangeofmotionwas satis-factorilyrestored,persistedinpainandwasdissatisfiedwith the results. The two patients (cases 2and 8) with regular resultsobtainedrangeofmotionimprovement;however,they stillhadrestrictionsandpainduringdailyactivities,andone ofthempresentedreflexsympatheticdystrophy(case8).
Conclusion
Arthroscopic release of patients with adhesive capsulitis refractorytoconservativetreatmentiseffectiveforimproving painandrangeofmotion.
Thebestresultswereobtainedinpatientswhounderwent inferiorcapsulotomy.
Lowerreoperationrateswereobservedinpatientsinwhom theinterscalene catheterforanesthetic infusionwasused, demonstratingitsimportanceinpostoperativerehabilitation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. NeviaserJS.Adhesivecapsulitisoftheshoulder.JBoneJoint SurgAm.1945;27:211–22.
2. ReevesB.Thenaturalhistoryofthefrozenshoulder syndrome.ScandJRheumatol.1975;4(4):193–6.
3. GreyRG.Thenaturalhistoryofidiopathicfrozenshoulder.J BoneJointSurgAm.1978;60(4):564.
4. EndresNK,ElHassanB,HigginsLD,WarnerJP.Thestiff shoulder.In:RockwoodCAJr,MatsenFA3rd,WirthMA, LippittSB,editors.Theshoulder.4thed.Philadelphia: Saunders;2009.p.1405–28.
5. RobinsonCM,SeahKT,CheeYH,HindleP,MurrayIR.Frozen shoulder.JBoneJointSurgBr.2012;94(1):1–9.
6. FerreiraFilhoAA.Capsuliteadesiva.RevBrasOrtop. 2005;40(10):565–74.
7. ChecchiaSL,FregonezeM,MiyazakiAN,SantosPD,SilvaL, OssadaA,etal.Tratamentodacapsuliteadesivacom bloqueiosseriadosdonervosupraescapular.RevBrasde Ortop.2006;41(7):245–52.
8. LafosseL,BoyleS,KordasiewiczB,Aranberri-GutiérrezM, FritschB,MellerR.Arthroscopicarthrolysisforrecalcitrant frozenshoulder:alateralapproach.Arthroscopy.
2012;28(7):916–23.
9. WarnerJJ,AllenA,MarksPH,WongP.Arthroscopicreleasefor chronic,refractoryadhesivecapsulitisoftheshoulder.JBone JointSurgAm.1996;78(12):1808–16.
10.JeroschJ.360degreesarthroscopiccapsularreleasein patientswithadhesivecapsulitisoftheglenohumeral joint-indication,surgicaltechnique,results.KneeSurgSports TraumatolArthrosc.2001;9(3):178–86.
11.HarrymanDT2nd,MatsenFA3rd,SidlesJA.Arthroscopic managementofrefractoryshoulderstiffness.Arthroscopy. 1997;13(2):133–47.
12.SegmüllerHE,TaylorDE,HoganCS,SaiesAD,HayesMG. Arthroscopictreatmentofadhesivecapsulitis.JShoulder ElbowSurg.1995;4(6):403–8.
13.BaumsMH,SpahnG,NozakiM,SteckelH,SchultzW,Klinger HM.Functionaloutcomeandgeneralhealthstatusin patientsafterarthroscopicreleaseinadhesivecapsulitis. KneeSurgSportsTraumatolArthrosc.2007;15(5):638–44. 14.TastoJP,EliasDW.Adhesivecapsulitis.SportsMedArthrosc.
2007;15(4):216–21.
15.LoewM,HeichelTO,LehnerB.Intraarticularlesionsin primaryfrozenshoulderaftermanipulationundergeneral anesthesia.JShoulderElbowSurg.2005;14(1):16–21. 16.KohKH,KimJH,YooJC.Iatrogenicglenoidfractureafter
brisementmanipulationforthestiffnessofshoulderin patientswithrotatorcufftear.EurJOrthopSurgTraumatol. 2013;23Suppl.2:S175–8.
17.MagnussenRA,TaylorDC.Glenoidfractureduring
manipulationunderanesthesiaforadhesivecapsulitis:acase report.JShoulderElbowSurg.2011;20(3):e23–6.
18.OzakiJ,NakagawaY,SakuraiG,TamaiS.Recalcitrantchronic adhesivecapsulitisoftheshoulder.Roleofcontractureofthe coracohumeralligamentandrotatorintervalinpathogenesis andtreatment.JBoneJointSurgAm.1989;71(10):1511–5. 19.GerberC,EspinosaN,PerrenTG.Arthroscopictreatmentof
shoulderstiffness.ClinOrthopRelatRes.2001;(390):119–28. 20.PollockRG,DuraldeXA,FlatowEL,BiglianiLU.Theuseof
arthroscopyinthetreatmentofresistantfrozenshoulder. ClinOrthopRelatRes.1994;(304):30–6.
21.CohenM,AmaralMV,BrandãoBL,PereiraMR,MonteiroM, MottaFilhoGR.Avaliac¸ãodosrersultadosdotratamento artroscópicodacapsuliteadesiva.RevBrasOrtop. 2013;48(3):272–7.
22.JeroschJ,FillerTJ,PeukerET.Whichjointpositionputsthe axillarynerveatlowestriskwhenperformingarthroscopic capsularreleaseinpatientswithadhesivecapsulitisofthe shoulder?KneeSurgSportsTraumatolArthrosc.
2002;10(2):126–9.
23.JeroschJ,AldawoudyAM.Chondrolysisoftheglenohumeral jointfollowingarthroscopiccapsularreleaseforadhesive capsulitis:acasereport.KneeSurgSportsTraumatol Arthrosc.2007;15(3):292–4.
24.ZuckermanJD,RokitoA.Frozenshoulder:aconsensus definition.JShoulderElbowSurg.2011;20(2):322–5. 25.EllmanH,HankerG,BayerM.Repairoftherotatorcuff.
End-resultstudyoffactorsinfluencingreconstruction.JBone JointSurgAm.1986;68(8):1136–44.
26.HawkinsRJ,BokosDJ.Clinicalevaluationofshoulder problems.In:RockwoodCAJr,MatsenFA3rd,editors.The shoulder.2nded.Philadelphia:Saunders;1998.p.175–80. 27.GreenS,BuchbinderR,HetrickS.Physiotherapyinterventions
forshoulderpain.CochraneDatabaseSystRev. 2003;(2):CD004258.
28.PriceMR,TillettED,AclandRD,NettletonGS.Determiningthe relationshipoftheaxillarynervetotheshoulderjoint capsulefromanarthroscopicperspective.JBoneJointSurg Am.2004;86(10):2135–42.
29.YooJC,KimJH,AhnJH,LeeSH.Arthroscopicperspectiveof theaxillarynerveinrelationtotheglenoidandarmposition: acadavericstudy.Arthroscopy.2007;23(12):1271–7.
30.CinarM,AkpinarS,DerincekA,CirciE,UysalM.Comparison ofarthroscopiccapsularreleaseindiabeticandidiopathic frozenshoulderpatients.ArchOrthopTraumaSurg. 2010;130(3):401–6.