www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
CASE
REPORT
Hearing
rehabilitation
in
Treacher
Collins
Syndrome
with
bone
anchored
hearing
aid
José
Fernando
Polanski
a,b,∗,
Anna
Clara
Plawiak
a,b,
Angela
Ribas
caFaculdadeEvangélicadoParaná,Curitiba,PR,Brazil bUniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil cUniversidadeTuiutidoParaná(UTP),Curitiba,PR,Brazil
Received21October2014;accepted18January2015 Availableonline28August2015
KEYWORDS
Mandibulofacial dysostosis; Hearing
loss/rehabilitation; Child
Abstract
Objective: Todescribeacaseofhearing rehabilitationwithboneanchoredhearing aidina
patientwithTreacherCollinssyndrome.
Casedescription: 3 years old patient, male, with Treacher Collins syndrome and severe
complicationsduetothesyndrome,mostlyrelatedtotheupperairwayandhearing.Hehad
bilateralatresiaofexternalauditorycanals,andmalformationofthepinna.Theinitialhearing
rehabilitationwaswithbonevibrationarch,buttherewaspooracceptanceduethediscomfort
causedbyskullcompression.Itwasprescribedamodelofbone-anchoredhearingaid,insoft
bandformat.Theresultswereevaluatedthroughbehavioralhearingtestsandquestionnaires
MeaningfulUseofSpeechScale(MUSS)andInfant-ToddlerMeaningfulAuditoryIntegrationScale
(IT-MAIS).
Comments: Thepatienthadahigheracceptanceofthebone-anchoredhearingaidcomparedto
thetraditionalbonevibrationarch.Audiologicaltestsandthespeechandauditoryskills
assess-mentsalsoshowedbettercommunicationandhearingoutcomes.Thebone-anchoredhearing
aidisagoodoptioninhearingrehabilitationinthissyndrome.
©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-license(https://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Disostose mandibulofacial; Deficiência
auditiva/reabilitac¸ão; Crianc¸a
Reabilitac¸ãoauditivanaSíndromedeTreacherCollinspormeiodepróteseauditiva ancoradanoosso
Resumo
Objetivo: Descrever um casode reabilitac¸ão auditivapor meio douso de prótese auditiva
ancoradanoossoemumpacienteportadordaSíndromedeTreacherCollins.
Descric¸ãodocaso: Pacientede3anos,masculino,portadordasíndromedeTreacherCollins,
com complicac¸ões graves relacionadas à síndrome, principalmente de vias aéreas altas
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2015.01.010
∗Correspondingauthor.
E-mail:[email protected](J.F.Polanski).
e audic¸ão. Apresentava atresia de condutos auditivos externos bilateralmente, além de
malformac¸ãodospavilhõesauditivos.Parareabilitac¸ãoauditivainicialfoiindicadoaparelho
auditivoemarcodevibrac¸ãoóssea,porémhouvepéssimaaceitac¸ãopelodesconfortocausado
pelacompressãonocrânio.Foiindicadocomométodoalternativoummodelodeprótese
audi-tivaancoradanoosso,noformatosoftband.Osresultadosforamavaliadospormeiodetestes
auditivoscomportamentaiseatravésdosquestionáriosMeaningfulUseofSpeechScale(MUSS)
eInfant-ToddlerMeaningfulAuditoryIntegrationScale(IT-MAIS).
Comentários: opacienteteveumaexcelenteaceitac¸ãodapróteseauditivaancoradanoosso
quandocomparadaaotradicionalarcodevibrac¸ãoóssea.Ostestesaudiológicosbemcomoas
avaliac¸õesdehabilidadesdefalaedeaudic¸ãotambémdemonstrarammelhorescapacidadesde
comunicac¸ãoeaudic¸ão.Esseequipamentomostra-seumaboaopc¸ãonareabilitac¸ãoauditiva
deportadoresdessasíndrome.
©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo
OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
The TreacherCollinssyndrome, firstdescribed in 1900 by aBritishopticianEdwardTreacherCollins,isanautosomal dominantdisorderthataffectsonein50,000livebirths.1
In this syndrome, there is a mutation in the TCOF1
(5q32locus)gene, responsible for encodingthe nucleolar phosphoproteinTreacle,whichisdirectlyinvolvedwiththe developmentofthefirsttwopharyngealarches.2,3 Approx-imately60%ofcasesdonothaveapositivefamilyhistory, butareduetoadenovomutation.4
The phenotype of these patients is diverse. There are cases in which the patient is mildly affected, and there may be a difficulty in establishing the diagnosis; on the otherhand,somepatientshaveearlydeathintheperinatal period,usuallycaused bythe severe airwayimpairment.3 Among the main malformations found are the downward-slanting of palpebral fissure or antimongoloid inclination, mandibular hypoplasia, ear, external auditory canal and middle ear deformities, cleft palate and choanal atresia, amongothers.5
Between 30% and 50% of the affected children have severe bilateral conductive hearing loss, as a result of stenosis or atresia of the external auditory canal or mid-dle ear malformations.6 Hearing rehabilitation should be performedasearlyaspossible,inordertoensurethe ade-quatedevelopmentof languageandlearning.1 Becauseof thesevere malformations affecting the patients’hearing, surgicalreconstructiondoesnotusuallyhavegoodresults.6 Asaresultofthemalformationoftheexternalauditory canal,theuseoftraditionalhearingaids,canrarelybe indi-cated.Themostcommonalternativeforrehabilitationisthe bonevibration arch.This typeofprosthesis hassome dis-advantages,mainlyrelatedtoexcesspressureofthearch, poorestheticalappearanceanddifficultyinmaintainingthe archinplacewhenthepatientisachild,asitcanbeeasily removed(Fig.1).7
A recent alternative for the auditory rehabilitation of thesepatients is the Bone AnchoredHearing Aid (BAHA), whichconsistsofanoptionincasesofconductiveormixed hearinglossandhasalowrateofcomplicationsassociated withgoodfunctionalresults.1
Figure1 Typeofprosthesis.
The present study reports the use of BAHA in hearing rehabilitationofachildwithTreacherCollinssyndromewith bilateral atresia of the external auditory canal. We also describethe methodsusedin theauditory evaluationand rehabilitationresultmeasurementforpatientswiththis syn-dromeandatthisagegroup.
Case
report
Case report based on medical file review, approved by the institution’s ethics committee under number 24692213.7.0000.0103 and with Informed Consent form signedbythepatient’sguardian.
Figure2 Blepharoplasties.
The most severe complications associated with the syndromewereintheupperairwaysandthehearing impair-ment. Tracheostomy wasperformed soon after birth, and gastrostomyat3monthsofage.Orthognathicsurgerieswere performedat1yearand3months,1yearand8monthsand3 yearsand10months.Heiscurrentlystableandwelladapted regardingthe airways.Additionally, blepharoplasties were performedat6months,8months,1yearand8monthsand 1yearand10months(Fig.2).
AtthehearingassessmentperformedonApril2012,at1 yearand7months,theobjectiveandsubjectivetestswere used,asdescribedbelow:
• BrainstemAuditoryEvokedPotential:thechildhadabsent airwaythresholdsin90dBAandpresent bonethresholds in35dBA,onbothsides;
• Behavioralnote:thistestprovidescluesandinformation onglobaldevelopmentand,especially,theexpected audi-tory behaviorfor theageof thechild, andhelpsinthe diagnosisofhearinglossandotherassociateddisorders.8 At thefirstexamination, asshownin Table1, thechild showed lack of response to low and medium intensity sounds(rattle---50dB;rattle---70dB;bell---82dB), pres-enceofauditoryattentionandsearchofthesoundsource for highintensity sounds(castanets--- 92dB; agogobells --- 100dB)andabsenceofcochleopalpebralreflextohigh intensitysound(110dB).
After these initial assessments, on August 2012, at 1 yearand10months,ahearingaidwithbone vibratorwas adapted.Atthetest,afunctionalgainof40dBwasrecorded (Table2);however,deviceacceptancewaspoorduetothe compressionof theskull, andthepatient discontinuedits use.Asaresult,theuseofabone-anchoredhearingaidwas indicated.On August2013,at 2yearsand10months,the BAHAsystemmodelBP100withsoftbandwasactivatedand adapted. The behavioral observation recorded functional gainof60dB(Table3).
During consultation one month after the BAHA system activation,weappliedtwoprotocolstomeasurethespeech andlisteningskills:MeaningfulUseofSpeechScale(MUSS) and Infant-Toddler Meaningful Auditory Integration Scale (IT-MAIS).9,10 Regarding MUSS, which consists of a struc-turedinterviewwiththeparentsaimedtoevaluatetheuse ofspeech in everyday situations, themother wasable to identifyimprovementinthechild’scommunicativeintent, includingspeakingsmallisolatedwords.Thehearing capac-ities were analyzed and measured by the IT-MAIS, which consistsofastructuredinterviewwiththeparents,inorder toassess thechild’s spontaneousresponses tothe sounds inhisdailylifeenvironment.Thechildreached,onemonth aftertheuseofBAHA,ascoreof100%intheIT-MAIS, man-agingtodirectattention tothesound source,detect and recognizeverbalsoundsandreacttocomplexorders.
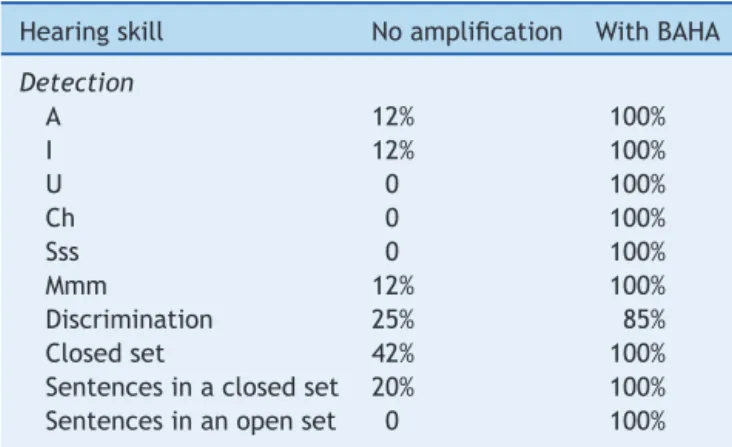
AtanassessmentonOctober2014,at4yearsofage, dur-ingahearingperceptiontestwithnovisualcues,heattained theresultsshown in Table4. Thechild remains in speech
Table1 Behavioralresponseswithoutamplification.
Uncalibratedsounds O CPR S A SS LS LD LU
50dBrattle X
75dBrattle X
82dBbell X
92dBblack---black X
100dBlargeagogobells X
110dBdrum X
Calibratedsounds 500Hz 1000Hz 2000Hz 4000Hz
Rightear 80 80 ↓ ↓
Leftear 80 80 ↓ ↓
Table2 Behavioralresponseswithamplificationthroughhearingaidwithbonevibrationarch.
Uncalibratedsounds O CPR S A SS LS LD LU
50dBrattle X
75dBrattle X
82dBbell X
92dBblack---black X
100dBlargeagogobells X
110dBdrum X
Calibratedsounds 500Hz 1000Hz 2000Hz 4000Hz
Rightear 40 40 60 ↓
Leftear 40 60 60 ↓
O,noresponse; CPR,cochleopalpebral reflex;S,startled response;A, attention;SS, seekssource;LS,lateralizes totheside;LD, lateralizesdownward;LU,lateralizesupward.
Table3 Behavioralresponseswithamplificationthroughbone-anchoredhearingaid.
Uncalibratedsounds O CPR S A SS LS LD LU
50dBrattle X
75dBrattle X
82dBbell X
92dBblack---black X
100dBlargeagogobells X
110dBdrum X
Calibratedsounds 500Hz 1000Hz 2000Hz 4000Hz
Rightear 20 20 20 40
Leftear 20 20 30 40
O,noresponse; CPR,cochleopalpebral reflex;S,startled response;A, attention;SS, seekssource;LS,lateralizes totheside;LD, lateralizesdownward;LU,lateralizesupward.
therapyfor auditoryandlanguagestimulation,in addition toamultidisciplinarymedicalfollow-up.
Discussion
Cases of external auditory canal malformation or atresia often remain without adequate hearing rehabilitation, or endupbeingrehabilitatedinanunsatisfactorymanner,with theuse of bone vibrationarches. These arches,the most oftenusedwaytoproviderehabilitationinthesecases,are frequentlypoorlyacceptedbytheuser,duetoesthetic rea-sons or mainly due toexcessive compression onthe skin.
Table4 Auditory perceptioncomparing noamplification
andbone-anchoredhearingaid(BAHA).
Hearingskill Noamplification WithBAHA
Detection
A 12% 100%
I 12% 100%
U 0 100%
Ch 0 100%
Sss 0 100%
Mmm 12% 100%
Discrimination 25% 85%
Closedset 42% 100%
Sentencesinaclosedset 20% 100%
Sentencesinanopenset 0 100%
Inadditiontothestructuralissue ofthisequipment,they have olderandlimitedaudiological technology,promoting hearinggainsthatareoftenineffective.
ThefirstmodelsofBAHAbecamecommerciallyavailable abroadon1987.11InBrazil,itsuseismorerecent.12Asthe systemdirectlystimulatesthecochleawithoutinvolvingthe airconductionhearing,i.e.theexternalauditorycanaland middle ear, it is in an excellent option for patients with deformitiesofthehearingsystem.
In the studied case, due to the child’s young age, we chosetouse theequipmentin itssoftbandformat, which is an option for using the same device with an elastic band. As thechildgrowsand skullthicknessconsequently increases,thesameequipmentcanbeused,butattached toatitaniumimplantthatissurgicallyinsertedintotheskull bone.Generally,theadequatebonethicknesstoreceivethis implantshouldbeapproximately5mm,whichisthe thick-nessattainedataround5yearsofage.13Itisknownthatthe implant fixation failure rate is higher in children younger than 5years.13 Inaddition,patients withTreacherCollins syndromehavedelayedgrowthoftheskullbones,whichmay further accentuate the difficulty of fixing the implants.14 The surgicalprocedureisplanned,inthiscase, tobe per-formedafter5yearsofage,whentheimplantthatwillbe usedtoattachthesamesoundprocessor,previouslyusedin softbandformat,willbeinserted.
by BAHA use through objective auditory tests is not feasible,duetothechild’syoungage---hencethe perfor-manceofbehavioraltestsandspeechandhearingcapacity protocols.9,10
We considerthis report to be important, asthere are few studies in our country using this technology in hear-ing rehabilitation. In addition, as far as the literature search demonstrated, no study in our language on the use of such equipment, specifically for auditory rehabili-tationinTreacherCollinssyndrome,wasidentified.Inthe international literature, the studies are not very numer-ous either.1,13---19 Onthe other hand, thesechildren, given the degree of multiple disorders, are always followed by multidisciplinary teams, in which the pediatrician is the head of the group and often the main responsible for decision-makingandtreatment plan.Thus,itis important foreveryoneinvolvedinthecareofthesepatientstoacquire informationonthesenewtechnologies.
Asourfinalconsiderations,wereaffirmtheimportanceof disseminatingknowledgeabouttheuseofthisequipment, asitisanewandeffectivealternativetoauditory rehabili-tation.PatientswithTreacherCollinssyndromecomprisea groupofindividualsthatcanlargelybenefitfromtheuseof thistechnology.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MarsellaP,ScorpecciA,PacificoC,TieriL.Bone-anchored hear-ingaid(Baha)inpatientswithTreacherCollinssyndrome:tips andpitfalls.IntJPediatrOtorhinolaryngol.2011;75:1308---12. 2.Jensen-SteedG.TreacherCollinssyndrome:acasereview.Adv
NeonatalCare.2011;11:389---94.
3.DixonJ,TrainorP,DixonMJ.TreacherCollinssyndrome.Orthod CraniofacRes.2007;10:88---95.
4.SheteP,TupkariJV,BenjaminT,SinghA.TreacherCollins syn-drome.JOralMaxillofacPathol.2011;15:348---51.
5.Thompson JT, Anderson PJ, David DJ. Treacher Collins syn-drome: protocol management from birth to maturity. J CraniofacSurg.2009;20:2028---35.
6.Lesinska E,StankeviciuteV,PetrulionisM.Applicationofthe Vibrant Soundbridge middle-ear implant for aural atresia in patients with Treacher Collins syndrome. J Laryngol Otol. 2012;126:1216---23.
7.HåkanssonB,TjellströmA,RosenhallU.Hearingthresholdswith directboneconductionversusconventionalboneconduction. ScandAudiol.1984;13:3---13.
8.AzevedoMF.Desenvolvimentoauditivodecrianc¸asnormaisede altorisco.SãoPaulo:Plexu;1995.
9.NascimentoLT.Umapropostadeavaliac¸ãodalinguagemoral (Monografia).Bauru(SPSP):USP;1997.
10.Fortunato-TavaresT,Befi-LopesD,BentoRF,AndradeCR. Chil-drenwithcochlearimplants:communicationskillsandquality oflife.BrazJOtorhinolaryngol.2012;78:15---25.
11.TietzeL,PapsinB.Utilizationofbone-anchoredhearingaidsin children.IntJPediatrOtorhinolaryngol.2001;58:75---80. 12.PedrialiIV,BuschleM,MendesRC,etal.Implantedprosthetics
osseousconduction(BAHA):reportedcases.ArqInt Otorrino-laringol.2011;15:249---55.
13.McDermottAL,WilliamsJ,KuoM,ReidA, ProopsD.The bir-minghampediatricbone-anchoredhearingaid program:a 15 yearexperience.OtolNeurotol.2009;30:178---83.
14.ZeitounH, De R,Thompson SD, Proops DW.Osseointegrated implantsinthemanagement ofchildhoodear abnormalities: with particularemphasis on complications. J Laryngol Otol. 2002;116:87---91.
15.RamakrishnanY,MarleyS,LeeseD,DavisonT,JohnsonIJ. Bone-anchoredhearingaidsinchildrenandyoungadults:theFreeman Hospitalexperience.JLaryngolOtol.2011;125:153---7. 16.HabalM,FransN, ZelskiR,Scheuerle J.Percutaneous
bone-anchoredhearingaid.JCraniofacSurg.2003;14:637---42. 17.Granström G, Jacobsson C. First and second branchial arch
syndrome: aspects on the embryogenesis, elucidations, and rehabilitationusingtheosseointegrationconcept.ClinImplant DentRelatRes.1999;1:59---69.
18.Van der Pouw KT, Snik AF, Cremers CW. Audiometric resultsof bilateralbone-anchoredhearing aid applicationin patientswithbilateralcongenitalauralatresia.Laryngoscope. 1998;108:548---53.