www.jped.com.br
ORIGINAL
ARTICLE
Peri-intraventricular
hemorrhage
and
oxidative
and
inflammatory
stress
markers
in
very-low
birth
weight
newborns
夽
,
夽夽
Jamil
P.S.
Caldas
a,∗,
Carolina
A.
Braghini
b,
Taís
N.
Mazzola
b,
Maria
M.S.
Vilela
c,
Sérgio
T.M.
Marba
caNeonatologyDivision,HospitaldaMulherProf.Dr.JoséAristodemoPinotti,CentrodeAtenc¸ãoIntegralàSaúdedaMulher (CAISM),UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
bCentrodeInvestigac¸ãoemPediatria(CIPED),UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
cDepartmentofPediatrics,FaculdadedeCiênciasMédicas,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
Received7July2014;accepted22September2014 Availableonline23April2015
KEYWORDS Oxidativestress; Reactiveoxygen species; Interleukin-6; Glutathione; Intraventricular hemorrhage; Newborn
Abstract
Objectives: Toevaluate theassociationbetween oxidativeandinflammatorystress markers
withperi-intraventricularhemorrhage(PIVH)invery-lowbirthweightnewborns.
Methods: ThiswasaprospectivestudyconductedinalevelIIIneonatalunit.Basaland
stimu-latedreactiveoxygenintermediates(ROIs),reducedglutathione(GSH),andinterleukin-6(IL-6)
levelsweremeasuredinumbilicalcordblood.Newborns underwentserialultrasoundatthe
bedside,at6,12,24,and72hoursoflifeandatsevendaysforthediagnosisofPIVH,classified
asgradesItoIV.Twogroupswereassessed,thosewithandwithoutPIVH;maternalandneonatal
controlvariableswereusedforcomparison.Univariateandmultipleregressionanalyseswere
applied.
Results: Atotalof125newbornswereassessed.PIVHincidenceratewas12.0%.Intheunivariate
analysis, basalROI, theuse oftwo ormoredoses ofcorticosteroids, birthweight<1,000g,
ventilatory support use,and SNAPPEII value ≥22 were significantly associated withPIVH.
However,inthemultivariateanalysis,onlyantenatalsteroidusewasindependentlyassociated
withthedisease(OR0,194;95%CI:0,048to0,773;p=0,02).
夽 Pleasecitethisarticleas:CaldasJP,BraghiniCA,MazzolaTN,VilelaMM,MarbaST.Peri-intraventricularhemorrhageandoxidativeand
inflammatorystressmarkersinvery-lowbirthweightnewborns.JPediatr(RioJ).2015;91:373---9.
夽夽StudyconductedattheSchoolofMedicalSciences,UniversidadeEstadualdeCampinas,CentrodeInvestigac¸ãoemPediatria(CIPED),
UniversidadeEstadualdeCampinas,andHospitaldaMulherProf.Dr.JoséAristodemoPinotti,CentrodeAtenc¸ãoIntegralàSaúdedaMulher
(CAISM),UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
∗Correspondingauthor.
E-mails:[email protected],[email protected](J.P.S.Caldas). http://dx.doi.org/10.1016/j.jped.2014.09.008
Conclusion: ROI,GSH,andIL-6levelswerenotassociatedwiththeoccurrenceofPIVHin
very-lowbirthweightinfants
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Estresseoxidativo; Espéciesdeoxigênio reativas;
Interleucina-6; Glutationa;
Hemorragiacerebral; Recém-nascido
Hemorragiaperi-intraventricularemarcadoresdeestresseoxidativoeinflamatório emRNsdemuitobaixopesoaonascer
Resumo
Objetivos: avaliaraassociac¸ãoentremarcadoresdeestresseoxidativoeinflamatóriocoma
hemorragia peri- eintraventricular (HPIV) em recém-nascidos(RN) demuito baixopeso ao
nascer.
Métodos: estudoprospectivoemunidadeneonatalnívelIII.Foifeitadosagememsanguede
cordãoumbilical deintermediáriosreativosdeoxigênio (ROI)basaleestimulado,glutationa
reduzida(GR)einterleucina-6(IL-6).Recém-nascidosforamsubmetidosàultrassonografia
seri-ada,àbeira doleito,com6, 12,24 e72 horasdevidae7diasparaodiagnósticodeHPIV,
classificadaemgrausdeIaIV.Foramavaliadosdoisgrupos:comesemHPIVevariáveisde
con-trolematernaseneonataisforamusadasparacomparac¸ão.Análiseunivariadaederegressão
múltiplaforamaplicados.
Resultados: foramavaliados125recém-nascidos.AtaxadeincidênciadeHPIVfoide12,0%.Na
análiseunivariadaovalorbasaldeROI,ousodeduasoumaisdosesdecorticosteroide,pesoao
nascermenorque1.000g,ousodeassistênciarespiratóriaevalordeSNAPPEIImaiorouigual
a22foramsignificativamenteassociadosàHPIV.Porém,naanálisemultivariada,apenasouso
antenataldeesteroidessemostrouindependentementeassociadoàdoenc¸a(OR0,194IC95%
0,048-0,773p=0,02).
Conclusão: ROI,GReIl-6nãoforamassociadosàocorrênciadeHPIVemRN demuitobaixo
pesoaonascer
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
Peri-intraventricular hemorrhage (PIVH) remains a high-prevalencedisease in pretermnewborns, especially those withbirth weight<1,500gandgestationalage<34weeks. Thediseaseisassociatedwiththedevelopmentof posthe-morrhagic hydrocephalus, neurodevelopmental disorders, needforspecializedrehabilitationtherapies,andhighsocial costs.1,2
The most commonsiteof PIVHis the germinalmatrix, whichislocatedintheperiventricularsubependymalregion andisirrigatedbyfragileandimmaturevasculature.Itisan importantproliferation siteof neuronalprecursors before theirmigrationtotheirfinallocationinthecerebralcortex. Severalfactors,especiallythoserelatedtocerebral hypo-perfusionandreperfusionphenomena,canresultinbleeding atthissite.2,3
Inadditiontothemechanismofvascularrupture associ-atedwithcerebralblood flowimpairment,PIVHcanoccur duetoothermechanisms,whichmaybeofvascularorigin ornot.2
Experimentalstudiesandthosewithhumanshaveshowed anassociationbetweenPIVHandoxidativestress.In exper-imental studies in preterm newborn dogs, Ment et al. demonstrated that blocking the production of free rad-icals with etamsylate and indomethacin, or the use of superoxide-dismutase, had a protective effect on PIVH
occurrence after reperfusion injury due to hypovolemic hypotension.3---5
Morerecently,therehasbeenevidenceofanassociation between PIVH with intrauterine inflammatory-infectious processes,6---8 as well as an association between serum
interleukin-6(IL-6)levelsandvascularendotheliummatrix lesionsbycytokines.9---11
However, the specific evaluation of oxidative stress markers such as reactive oxygen species and glutathione antioxidant enzyme has not been assessed regarding the developmentofPIVH.
This study aimedto evaluate theassociation of oxida-tivestressmarkers,specificallytheproductionofreactive oxygenintermediates(ROIs)andreducedglutathione(GSH) levels,withinflammationmarkers, namelyserumIL-6 lev-elsmeasuredinumbilicalcordblood,asriskfactorsforthe developmentofPIVH.
Methods
centralnervoussystem;andneonataldeathwithinsixhours of life, preventing the performance of the first cerebral ultrasound.
Sample size was calculated according to the umbili-cal cord serum levels of IL-6 as a marker of PIVH onset in very-low birth weight newborns, based on the study by Heep et al.,9 in which IL-6 was categorized into
val-ues>100pg/mL or ≤ 100pg/mL, with PIVH rates of 63%
and 38% in these groups, respectively. Considering a 5% significance level, a test power of 80%, and a local PIVH incidencerateof20%,thecalculatedminimumsamplesize wasn=125.9
The assessed outcome was the presence of peri-intraventricularhemorrhage (PIVH), dividing patients into twogroups:withandwithout PIVH,classifiedaccordingto Papileetal.12
ForthediagnosisofPIVH,newbornsunderwentcerebral ultrasoundatthebedside,aftersix,12,24,and72hoursof life andat seven daysofage, usingthe anteriorfontanel as acoustic window and a Xario® (Toshiba®, CA, United States)echographwitha5-mHztransducer.Theexamswere recordedandstoredonCD-ROMsandreviewedbytwo expe-rienced evaluators. In case of doubt, a third expert was calledtogivehis/heropinion.
Umbilicalcordbloodwascollectedatbirthforthe mea-surementof biochemicalmarkers, after theinfant’s birth withthe placenta stillattached, throughpuncture of the umbilicalvessels,thusyieldingamixedsample,botharterial andvenous.Then,thematerialwasdistributedintothree vials,twowithananticoagulantandonecontainingsilicon oxalateandthesampleswereprocessedimmediately.
ThemeasurementofROIproductionfrom polymorphonu-clear leukocytes wasdetermined using flow cytometryin twodifferentmoments:spontaneous(orbasal)production, withleukocytesincubatedonly inHanks solution;and the stimulated sample, with leukocytes incubatedin Phorbol-myristate acetate.13 Values were expressed in nMol ×106
cells.
The measurement of erythrocyte GSH levels was per-formed by spectrophotometry: the assays performed in duplicateandresultswereexpressedinmg%inrelationto hematocrit.14
IL-6wasmeasuredinsamplesfrozenat-80◦
Cbyenzyme linkedimmunosorbentassay(ELISA),accordingtothe manu-facturer’sinstructions(R&DSystems®,MN,UnitedStates).15
Forcomparisonbetweengroups,thefollowingmaternal andneonatalcontrolvariablesthatcouldinterferewiththe PIVHoutcomewerefurtheranalyzed:primiparity, hyperten-sive disease,use of antenatalcorticosteroids and number of doses ≥ 2, vaginal delivery, cephalic presentation,
chorioamnionitis, twin pregnancy, birth weight<1,000g, gestationalage<30weeks,malegender,Apgarscore<7at thefirstandfifthminutes,needforresuscitation,smallfor gestationalage,ventilatorysupport,useofsurfactant,and ScoreforNeonatalAcutePhysiologyandPerinatalExtension (SNAPPE)IIvalue.
Maternalhypertensive diseasewasdefinedasthe pres-enceofsystolicbloodpressure(SBP)≥140mmHgorhigher
anddiastolicbloodpressure(DBP)≥90mmHg,intwo
mea-surements,withanintervalofatleastfourhoursbetween them, or the presence of SBP ≥ 160mmHg and DBP ≥
110mmHginasinglemeasurement.16Chorioamnionitiswas
definedasthepresenceof maternalfever (maternal tem-perature ≥ 37.8◦ C) combined with two or more of the
following signs: pain onuterine palpation, fetid/purulent amniotic fluid, fetal tachycardia (> 160 bpm), maternal tachycardia(>100 bpm)andleukocytosis (totalleukocyte count>15,000/mL).17Smallforgestationalagewasdefined
asthenewbornwithbirthweight<10thpercentile,according
tothefetalgrowthcurveofAlexanderetal.18
ForSNAPPEII,ROI,GSH, andIL-6values,thecutofffor categorizationwas obtained through the maximization of theareaunderthecurve(AUC).
Clinicalvariableswereonlyconsideredpresentorabsent atthetimeofdetectionofPIVHbyserialultrasound.Incase ofabsence ofPIVH development,variables wereassessed untiltheseventhdayoflife.
For statistical analysis, birth weight, gestational age, maternalage,andROIproductionvalues,aswellasblood levelsofGHSandIL-6,wereexpressedasmediansand25th
and75th percentiles, andwereassessed by Mann-Whitney
test. The chi-squared test or Fisher’s test were used to comparecategoricalvariables.Step-by-stepmultiple logis-ticregressionanalysiswasappliedtoverifytheindependent variableswiththeoccurrenceofPIVHoutcome,adaptedfor thecalculation of incidenceratiousingthe variablesthat showedsignificancelevel≥ 0.2intheunivariateanalysis.
Thesignificancelevelwassetatp<0.05.
TheSPSS,release15.0forWindows(SPSSInc.Statistics forWindows,Chicago,UnitedStates)wasusedinall statisti-calanalyses.Parentssignedaninformedconsent.Thestudy wasapprovedbythelocalResearchEthicsCommitteeunder No.971/2008.
Results
During the study period, 138 children with birth weight<1,500g were eligible for inclusion. Of these, 13 were not included in the present study, as umbilical cordblood collectionwasnotpossible in12children; two ofthesehadPIVH(16.66%),onewithgradeIandanother, grade III. One newborn was excluded because, although cordbloodhadbeencollected,hediedwithinlessthansix hoursoflife,whichpreventedtheultrasoundassessment.
Atotalof125childrenwereincluded inthestudy.The numberofmotherswas111,astherewere14multiple preg-nancies,11twinandthreetripletpregnancies.Therewas nomaternalrefusaltoparticipate.
Ofthe125childrenstudied,15hadPIVH(12.0%),sixof themwithgradeI,twowithgradeII,fourwithgradeIII,and threewithgradeIV.Themildformofthedisease(gradesI andII)occurredoneightcases(53.33%),andthesevereform (gradesIIIandIV)insevennewborns(46.66%).ThePIVHrate inthegroupthatwasnotincludedwassimilartothatofthe studygroup(16.6%vs.12.0%;p=0.342).
In four cases (26.67%), PIVH was diagnosed within six hoursoflife,includingthesevereformofthedisease,and nearlyhalf(46.6%)wasobservedatupto24hoursoflife.
Table1 BasalandstimulatedROIvalues,glutathione,andIL-6levelsinumbilicalcordbloodofverylowbirthweightpreterm
newborn,accordingtotheoccurrenceofPIVH.
PIVH pa
Markers N Present n Absent
bROI 14 0.50(0.4-0.6) 103 0.40(0.4-0.5) 0.045
sROI 14 38.65(17.15---66.70) 103 39.60(18.60-138.25) 0.355
GSH 13 67.25(56.71-78.31) 103 71.03(63.37-80.83) 0.337
IL-6 14 24.34(14.42-72.15) 107 34.20(13.98-62.58) 0.903
aMann-Whitneytest.
Valuesinmedian(p25-p75).
N,numberofcases;bROI,basalROI;sROI,stimulatedROI(valuesinnMol×106cells);GSH,reducedglutathione(valuesinmg%);Il-6,
interleukin-6(valuesinpg/mL)
life,one of themalready hada diagnosis of parenchymal hemorrhageatthecerebralultrasound(gradeIVofPapille etal.)12andwasclassifiedas‘‘presenceofPIVH’’.Theother
twocasesdiedafter31and43hoursoflife,without hem-orrhagiclesion at the ultrasoundat 6/12/24hoursof life, withnoPIVHat necropsy,andwerethereforeclassifiedas ‘‘absenceofPIVH’’.
When assessing the markers, it was observed that the basalROIproduction showedastatistically highermedian inthegroupwithPIVH(p=0.045).However,thestimulated production showed no statistical difference. The median glutathioneandIL-6valuesalsoshowednostatistically sig-nificantdifferencebetweenthegroups(Table1).
Regardingcontrolclinicalvariables,thegroupwith signif-icantlyPIVHhadthelowestmedianbirthweight(870versus 1,042g; p=0.017), gestational age (27 versus 29 weeks; p=0.014) and higher values of SNAPPE II (26 versus 17; p=0.016).
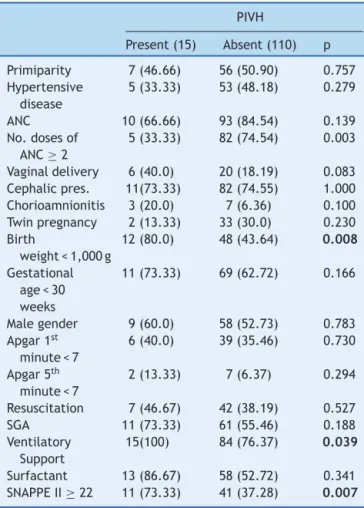
Regarding the use of antenatal betamethasone, it was observedthat82.4%(103/125)ofthenewbornsreceivedthe medication,and87 ofthem receivedthecomplete cycle, butnosignificantdifferencewasobservedintheincidence ofPIVH(10/15 versus93/110;p=0.1395).However,when the use of corticosteroids was assessed according to the numberofdosesused,itwasobservedthattheuseoftwo ormoredosesofbetamethasonewasmorestatistically fre-quent(p=0.003)inthegroupwithoutPIVH(Table2).
Regarding the other control variables, in the univari-ate analysis, PIVH was significantly associated with birth weight<1,000g,useoftwoormoredosesofantenatal cor-ticosteroids, respiratory assistance, and SNAPPE-II values
≥22. The other variables werenot significantlydifferent
betweenthetwogroups(Table2).
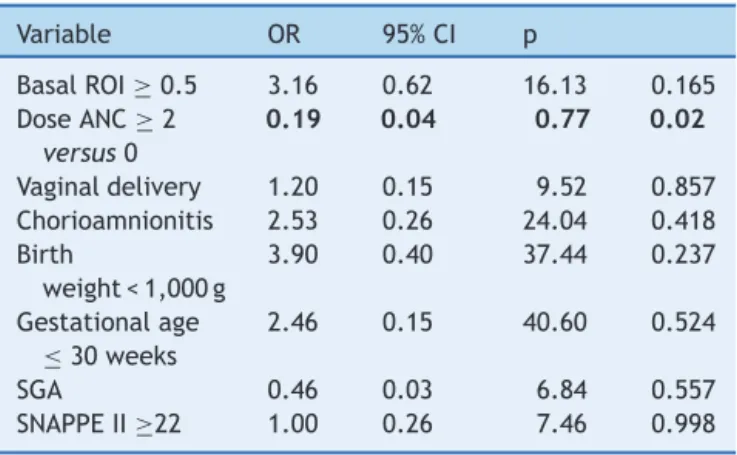
The following variables remained in the multivari-ate analysis: basal ROI (> 0.5 nMol×106 cells), two
or more doses of corticosteroids, vaginal delivery, birth weight<1,000g,gestationalage≤30weeks,nutritional
sta-tus,and SNAPPE ≥ 22.At the final resultof the multiple
analysis,ROIproductionwasnotindependentlyassociated withtheoccurrenceofthedisease.Itwasobservedthatonly theantenataluse oftwoor moredosesof corticosteroids was independently associated with PIVH, as a protective factor(OR0.194;95%CI:0.048to0.773;p=0.02;Table3). Glutathioneand IL-6levelswerenot included in thefinal multivariateregressionmodel,astheydidnotshow statis-ticaldifferenceintheunivariatemodel.
Discussion
The study compriseda population of newborns at riskfor PIVH.Birthweightwasusedastheinclusioncriterion,since although prematurityitself is themain risk factor for the disease,thedefinitionofgestationalagemaynotbeexact due totheinaccuracy of measurement methods.National and international researchnetworks have also used birth
Table2 DistributionofPIVHoccurrenceaccordingtothe
categoricalcontrolvariables.
PIVH
Present(15) Absent(110) p
Primiparity 7(46.66) 56(50.90) 0.757
Hypertensive disease
5(33.33) 53(48.18) 0.279
ANC 10(66.66) 93(84.54) 0.139
No.dosesof
ANC≥2
5(33.33) 82(74.54) 0.003
Vaginaldelivery 6(40.0) 20(18.19) 0.083
Cephalicpres. 11(73.33) 82(74.55) 1.000
Chorioamnionitis 3(20.0) 7(6.36) 0.100
Twinpregnancy 2(13.33) 33(30.0) 0.230
Birth
weight<1,000g
12(80.0) 48(43.64) 0.008
Gestational
age<30
weeks
11(73.33) 69(62.72) 0.166
Malegender 9(60.0) 58(52.73) 0.783
Apgar1st
minute<7
6(40.0) 39(35.46) 0.730
Apgar5th
minute<7
2(13.33) 7(6.37) 0.294
Resuscitation 7(46.67) 42(38.19) 0.527
SGA 11(73.33) 61(55.46) 0.188
Ventilatory Support
15(100) 84(76.37) 0.039
Surfactant 13(86.67) 58(52.72) 0.341
SNAPPEII≥22 11(73.33) 41(37.28) 0.007
Categoricalvariablesexpressedasapercentage.
ANC,antenatalcorticosteroid;SGA,smallforgestationalage;
SNAPPE II,Score for NeonatalAcutePhysiology and Perinatal
Table 3 Multiple regression analysis to assess variables
associatedwithPIVHinvery-lowbirthweightnewborns.
Variable OR 95%CI p
BasalROI≥0.5 3.16 0.62 16.13 0.165
DoseANC≥2
versus0
0.19 0.04 0.77 0.02
Vaginaldelivery 1.20 0.15 9.52 0.857
Chorioamnionitis 2.53 0.26 24.04 0.418
Birth
weight<1,000g
3.90 0.40 37.44 0.237
Gestationalage
≤30weeks
2.46 0.15 40.60 0.524
SGA 0.46 0.03 6.84 0.557
SNAPPEII≥22 1.00 0.26 7.46 0.998
OR,oddsratio;95%CI,95%confidenceinterval,ROI,reactive
oxygenintermediates;ANC,antenatalcorticosteroid;SGA,small
forgestationalage;SNAPPEII,ScoreforNeonatalAcute
Physi-ologyandPerinatalExtension.
weightasaninclusioncriterion,facilitatingdatacomparison betweentheunits.19---21
Cerebralultrasoundwasperformedwithinthefirsthours oflife,astheearlyperinatalandneonatalriskfactorsare veryimportantfortheonsetofPIVH;therefore,the analy-sisofbloodmarkersforPIVHcouldbetimelyconducted.In thepresentstudy,thediseasewasdetectedwithinthefirst hoursoflife,asalmost50%of hemorrhagecasesoccurred up to 24hours of life, which is in agreement with other studies.22 In additiontothediagnostic aspect,performing
an early serial ultrasound assessment allowed for a more appropriateselectionof neonatalrisk factorspresentat a certainmoment, aswell asfor establishing their associa-tion withthe disease diagnosis. Many of the studies that assessedtheriskfactorsforPIVHconsideredtheoccurrence of thediseasewithinseven daysoflife and,therefore,it wasnotpossible toaccurately identifythedecisivefactor inthediseasegenesis.23
BasalROIproductionwassignificantlyhigherinnewborns wholaterdevelopedPIVH.Thisfactimpliesthatleukocytes hadasignificantactivationpotentialatbirthandcould par-ticipateineventsrelatedtooxidativedamage.
Studies haveshown thatin normalfull-termnewborns, theproductionofsuperoxideanionsbypolymorphonuclear leukocytesfrombloodoftheumbilicalcordwassignificantly higherwhenthedeliverywasvaginal,whencomparedwith blood samples fromnewborns whose mothers had under-gone cesarean delivery, without labor. This suggests that leukocyteactivationispartofthemechanismsofparturition andnormalbirthprocesses.However,inpretermlabor,that leukocyteactivationinthefetuscouldcausetissuecell dam-age,eitherduetointensityofthereactionorthefunctional immaturity.24,25
Perroneetal. evaluatedthebasal andstimulated pro-ductionofsuperoxideanionsin168pretermnewbornswith 24-32 weeks gestation. When assessing several neonatal oxidative diseases relatedtooxidative stress,the authors foundnodifferenceinsuperoxideanionproductionbycord bloodleukocytes.However,theauthorsdidnotcommenton thedataregardingPIVHalone,duetothesmallnumberof cases.26
Stimulated ROI production was not different in both groups.Thisfactcouldbeexplainedeitherbecausethe pro-ductioninthegroupwithPIVHwasalreadyatitsmaximum, or, as this is an artificialin vitro stimulation, it may not reflect the complex conditions in vivo biological stimuli. In a study of polymorphonuclear leukocytes in full-term newborns,itwasdemonstratedthatthegenerationof super-oxideradicalsincreasedsignificantlyafterstimulationwith itsN-formyl-methionyl-leucyl-phenylalanine,buttherewas noadditional increase when IL-10 or dexamethasone was addedtotheculturemedium.27
As for glutathione,therewasnodifferencein the val-uesobserved in both groups. Studieshave shown that, as thepregnancyreachesterm,theantioxidantsystemblood levels,bothenzymaticornot,increasegraduallyandactas aprotectivefactor for therelativehyperoxiathatfollows birth.Therefore,thelowreserveofanon-enzymatic antiox-idantsystematapretermbirth exposesthenewborntoa greaterriskofoxidativedamage.28,29However,thelow
sam-plepower ofthetestforglutathionefound inthepresent study(11.5%),preventsgeneralizationsregardingthe exist-enceofaprotectiveeffectornot.
TheIL-6serumlevelswerenotdifferentinpatientswith andwithoutPIVH.This resultcouldbejustifiedbythelow incidenceofclinicalchorioamnionitisinthepopulation(8%). Furthermore,theprioreffectiveantimicrobialtreatmentof themothers,whichisroutinepracticeinourservice,could havereducedfetallevelsofcytokines,astheyhave short half-lives.30---32
The high incidence of hypertension in the sample (46.4%),mayalsoexplainthelack ofassociation between inflammation markers and PIVH. Experimentally, Kauma etal.demonstrated thathypertensive women’splacentas producedloweramountsof IL-6whencomparedwith nor-motensivepregnantwomen.33Antenatalcorticosteroiduse
couldalsoalterplacentalIL-6production,asshownin pla-centalcellcultures34andinastudywithhumans.32
Studies that have shown an association of PIVH with increased levels of IL-6 have some aspects that justify such difference, such as more premature newborns and, therefore, more susceptible to PIVH, selected population (pregnantwomenwithclinicalsuspicionof chorioamnioni-tis),higherincidenceofhistologicalchorioamnionitisinthe sampleandIL-6measurementin thenewborn’s bloodand notumbilicalcordblood.9---11InthestudybyBhandarietal.,
IL-6 levels in cord blood were significantly higher in the groupthat developed PIVH,but in the regressionanalysis usingclinicalvariableswithcorrectionforgestationalage, IL-6levelswerenotindependentlyassociatedwithPIVH.35
administration of the first dose (RR 0.26; 95%CI: 0.09 to 0.75).36
Steroidusealoneiscapableofalteringtheresponseof theassessedbiomarkers,withdecreasedproductionofROI andIL-6,27,32,34,37 andmaythereforepreventsuchmarkers
fromexpressingthemselvesandbeingfactorsindependently associated with PIVH. However, studies with controlled exposuretoantenatalsteroiduse,incaseofprematurebirth danger,wouldnotbeethical.
Conclusion
In conclusion, the basal production of ROI from umbili-cal cord blood was statistically higher in newborns that developedPIVH;however,inthemultivariateanalysis,the baseline ROI levelswere not statistically an independent riskfactorforHPIV.IL-6orglutathionelevelswerealsonot associatedwiththePIVH.
Funding
FundodeAmparoàPesquisadoEstadodeSãoPaulo(FAPESP) projeto08/57405-4.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Volpe JJ. Intracranial hemorrhage: germinal matrix-intraventricularhemorrhageoftheprematureinfant.In:Volpe JJ, editor. Neurology of the newborn. 5th ed.Philadelphia:
SaundersElsevier;2008.p.517---88.
2.Marba ST, Caldas JP, Vinagre LE, Pessoto MA. Incidence of periventricular/intraventricularhemorrhageinverylowbirth weight infants: a 15-year cohort study. J Pediatr (RioJ). 2011;87:505---11.
3.MentLR,StewartWB,DuncanCC.Beaglepuppymodelof intra-ventricularhemorrhage: ethamsylatestudies.Prostaglandins. 1984;27:245---56.
4.Ment LR, Stewart WB, Duncan CC. Beagle puppy model of intraventricular hemorrhage. Effect ofsuperoxide dismutase on cerebral blood flow and prostaglandins. J Neurosurg. 1985;62:563---9.
5.Ment LR, Stewart WB, Ardito TA, Huang E, Madri JA. Indomethacinpromotes germinalmatrix microvessel matura-tioninthenewbornbeaglepup.Stroke.1992;23:1132---7.
6.Dammann O, Leviton A. Maternal intrauterine infection, cytokines,andbraindamageinthepretermnewborn.Pediatr Res.1997;42:1---8.
7.deFeliceC,TotiP,LauriniRN,StumpoM,PiccioliniE,TodrosT, etal.Earlyneonatalbraininjuryinhistologicchorioamnionitis. JPediatr.2001;138:101---4.
8.Ogunyemi D, Murillo M, Jackson U, Hunter N, Alperson B. Therelationshipbetweenplacentalhistopathologyfindingsand perinataloutcomeinpreterminfants.JMaternFetalNeonatal Med.2003;13:102---9.
9.HeepA,BehrendtD,NitschP,FimmersR,BartmannP,Dembinski J.Increasedserumlevelsofinterleukin6areassociatedwith severeintraventricular haemorrhage inextremely premature infants.ArchDisChildFetalNeonatalEd.2003;88:F501---4.
10.TauscherMK,BergD,BrockmannM,SeidenspinnerS,SpeerCP, GroneckP.Associationofhistologicchorioamnionitis,increased levelsofcordbloodcytokines,andintracerebralhemorrhagein pretermneonates.BiolNeonate.2003;83:166---70.
11.KassalR, Anwar M, Kashlan F, Smulian J, Hiatt M, HegyiT. Umbilical vein interleukin-6 levels in very low birth weight infants developing intraventricular hemorrhage. Brain Dev. 2005;27:483---7.
12.PapileLA,BursteinJ,BursteinR,KofflerH.Incidenceand evolu-tionofsubependymalandintraventricularhemorrhage:astudy ofinfants withbirth weights less than 1.500 gm. J Pediatr. 1978;92:529---34.
13.RichardsonMP,AyliffeMJ,HelbertM,DaviesEG.Asimpleflow cytometryassayusingdihydrorhodamineforthemeasurement oftheneutrophil respiratoryburst inwhole blood: compari-sonwiththequantitativenitrobluetetrazoliumtest.JImmunol Methods.1998;219:187---93.
14.BeutlerE,editor.Redcellmetabolism.NewYork:Churchill Liv-ingstone;1986.p.126.
15.R&DSystemsDuoSet®ELISADevelopmentSystem.Human
IL-6---catalognumber:DY206.[cited2011Dec18].Availablefrom:
http://www.rndsystems.com.pdf./dy206.pdf
16.Marba ST, Parpinelli MA, Millen FC. Recém-nascido com hipertensãoarterial:conceitosatuais.In:SociedadeBrasileira dePediatria; ProcianoyRS,Leone CR,organizadores. PRORN Programa de Atualizac¸ão em Neonatologia: Ciclo 11. Porto Alegre: Artmed/Panamericana; 2014. p. 51-75 (Sistema de Educac¸ãoContinuadaàDistância,v.3).
17.Romero R, Sirtori M,Oyarzun E,Avila C,MazorM, Callahan R,etal.Infectionandlabor.V.Prevalence,microbiology,and clinicalsignificanceofintraamnioticinfectioninwomenwith pretermlaborand intactmembranes.AmJ ObstetGynecol. 1989;161:817---24.
18.AlexanderGR,HimesJH,KaufmanRB,MorJ,KoganM.AUnited States national reference for fetal growth. Obstet Gynecol. 1996;87:163---8.
19.FanaroffAA,StollBJ,WrightLL,CarloWA,EhrenkranzRA,Stark AR,etal.Trendsinneonatalmorbidityandmortalityforvery lowbirthweightinfants.AmJObstetGynecol.2007;196:e1---8. 20.Rede Brasileira de Pesquisas Neonatais. Rio de Janeiro. [cited2011Oct15].Availablefrom:http://www.redeneonatal. fiocruz.br
21.TheCanadian Neonatal Network. CNN Annual Report.[cited 2013 Mai 20]. Available from: http://www.canadianneo natalnetwork.org/portal/
22.Paneth N, Pinto-Martin J, Gardiner J, Wallenstein S, Kat-sikiotis V, Hegyi T, et al. Incidence and timing of germinal matrix/intraventricularhemorrhageinlowbirthweightinfants. AmJEpidemiol.1993;137:1167---76.
23.GleissnerM,JorchG,AvenariusS.Riskfactorsfor intraventric-ularhemorrhageinabirthcohortof3721prematureinfants.J PerinatMed.2000;28:104---10.
24.AmbrusoDR,StorkLC,GibsonBE,ThurmanGW.Increased activ-ityoftherespiratoryburstincordbloodneutrophils:kinetics oftheNADPHoxidaseenzymesysteminsubcellularfractions. PediatrRes.1987;21:205---10.
25.BuonocoreG,GioiaD,DeFilippoM,PiccioliniE,BracciR. Super-oxideanionreleasebypolymorphonuclearleukocytesinwhole bloodofnewbornsandmothersduringtheperipartalperiod. PediatrRes.1994;36:619---22.
26.Perrone S, Tataranno ML, Negro S, Longini M, Marzocchi B, Proietti F, et al. Early identification of the risk for free radical-relateddiseasesinpretermnewborns.EarlyHumDev. 2010;86:241---4.
28.Davis JM, Auten RL. Maturation of the antioxidant system andtheeffectsonpretermbirth.SeminFetalNeonatalMed. 2010;15:191---5.
29.BuhimschiIA,BuhimschiCS, PupkinM,Weiner CP.Beneficial impactoftermlabor:nonenzymaticantioxidantreserveinthe humanfetus.AmJObstetGynecol.2003;189:181---8.
30.ProcianoyRS,SilveiraRC.Theroleofsamplecollectiontiming oninterleukin-6levelsinearly-onsetneonatalsepsis.JPediatr (RioJ).2004;80:407---10.
31.LamH,NgPC.Biochemicalmarkersofneonatalsepsis. Pathol-ogy.2008;40:141---8.
32.AradI,Bar-Oz B, ErgazZ, NirA, Barak V. Interleukin-6and N-terminalpro-brainnatriuretic peptide cordbloodlevelsin prematureinfants:correlationswithperinatalvariables.IsrMed AssocJ.2010;12:419---23.
33.KaumaSW,WangY,WalshSW.Preeclampsiaisassociatedwith decreasedplacental interleukin-6production. J Soc Gynecol Investig.1995;2:614---7.
34.XuB,MakrisA,ThorntonC,HennessyA.Glucocorticoidsinhibit placentalcytokinesfromculturednormalandpreeclamptic pla-centalexplants.Placenta.2005;26:654---60.
35.Bhandari V, Buhimschi CS, Han CS, Lee SY, Pettker CM, CampbellKH,etal.Cordblooderythropoietinand interleukin-6 for prediction of intraventricular hemorrhage in the preterm neonate. J Matern Fetal Neonatal Med. 2011;24: 673---9.
36.Roberts D, Dalziel S. Antenatal corticosteroids for accel-erating fetal lung maturation for women at risk of preterm birth. Cochrane Database of Syst Rev. 2006;19: CD004454.