www.jped.com.br
REVIEW
ARTICLE
Prevalence
of
asthenopia
in
children:
a
systematic
review
with
meta-analysis
夽
Manuel
A.P.
Vilela
a,∗,
Lucia
C.
Pellanda
b,c,
Anaclaudia
G.
Fassa
a,
Victor
D.
Castagno
aaUniversidadeFederaldePelotas(UFPel),Pelotas,RS,Brazil
bGraduationPrograminHealthSciences:Cardiology,InstitutodeCardiologia,Fundac¸ãoUniversitáriadeCardiologia,Porto
Alegre,RS,Brazil
cUniversidadeFederaldeCiênciasdaSaúdedePortoAlegre(UFCSPA),PortoAlegre,RS,Brazil
Received26September2014;accepted31October2014 Availableonline16May2015
KEYWORDS
Asthenopia;
Eyefatigue;
Visualfatigue;
Eyestrain; Fatigue; Visual
Abstract
Objective: Toestimatetheprevalenceofasthenopiain0---18year-oldchildrenthrougha
sys-tematicreviewandmeta-analysisofprevalencestudies.
Sources: Inclusioncriteriawerepopulation-basedstudiesfrom1960toMayof2014reporting
theprevalence ofasthenopiainchildren. Thesearch wasperformed independently by two
reviewersinthePubMed,EMBASE,andLILACSdatabases,withnolanguagerestriction.This
systematicreviewwas performedinaccordancewith theCochraneCollaboration guidelines
andthePRISMAStatement.DownsandBlackscorewasusedforqualityassessment.
Summaryoffindings: Out of 1692 potentially relevant citations retrieved from electronic
databasesandsearchesofreference lists,26were identifiedaspotentiallyeligible.Fiveof
thesestudiesmettheinclusioncriteria,comprisingatotalof2465subjects.Pooledprevalence
ofasthenopiawas19.7%(12.4---26.4%).Themajorityofchildrenwithasthenopiadidnotpresent
visualacuityorrefractionabnormalities.Thelargeststudyevaluated1448childrenaged6years
andestimatedaprevalenceof12.6%.Associatedriskfactorswerenotclearlyestablished.
Conclusion: Althoughasthenopiaisafrequentandrelevantclinicalprobleminchildhood,with
potentialconsequencesforlearning,thescarcityofstudiesabouttheprevalenceandclinical
impactofasthenopiahinderstheeffectiveplanningofpublichealthmeasures.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:VilelaMA,PellandaLC,FassaAG,CastagnoVD.Prevalenceofasthenopiainchildren:asystematicreviewwith meta-analysis.JPediatr(RioJ).2015;91:320---5.
∗Correspondingauthor.
E-mail:[email protected](M.A.P.Vilela).
http://dx.doi.org/10.1016/j.jped.2014.10.008
PALAVRAS-CHAVE
Astenopia;
FadigaOcular;
FadigaVisual;
Tensãoocular;
Fadiga; Visual
Prevalênciadeastenopiaemcrianc¸as:análisesistemáticacommeta-análise
Resumo
Objetivo: pretendemosestimaraprevalênciadeastenopiaemcrianc¸asde0a18anosdeidade
pormeiodeumaanálisesistemáticaeumameta-análisedosestudosdeprevalência.
Fontesdosdados: oscritériosdeinclusãoforamestudosdebasepopulacionalde1960amaio
de2014querelataramprevalênciadeastenopiaemcrianc¸as.Abuscafoirealizadademaneira
independentepordoisanalisadoresnasbasesdedadosPubMed,EMBASEeLILACS,semrestric¸ão
deidioma.EssaanálisesistemáticafoirealizadadeacordocomasdiretrizesdaColaborac¸ão
Cochrane ecomaDeclarac¸ãodosItensdeRelatório Preferidospara AnálisesSistemáticase
Meta-Análise(PRISMA).AescalaDowns&Blackfoiusadaparaavaliac¸ãodaqualidade.
Síntesedosachados: deumtotalde1692citac¸õespossivelmenterelevantesrecuperadasde
basesdedadoseletrônicasebuscasdelistasdereferência,26foramidentificadascomo
pos-sivelmenteelegíveis.Cincodessesestudosatenderamaoscritériosdeinclusão,incluindoum
totalde2465indivíduos.Aprevalênciatotaldeastenopiafoide19,7%(12,4---26,4%).A
maio-riadascrianc¸ascomastenopianãoapresentavamanomaliasdeacuidadevisualourefrac¸ão.O
maiorestudoavaliou1448crianc¸asde6anosdeidade,comprevalênciaestimadade12,6%.Os
fatoresderiscoassociadosnãoforamclaramenteestabelecidos.
Conclusão: emboraaastenopiasejaumproblemaclínicofrequenteerelevantenainfância,
compossíveisconsequênciasparaoaprendizado,aescassezdeestudossobreaprevalênciaeo
impactoclínicodaastenopiaprejudicaoplanejamentoefetivodasmedidasdesaúdepública.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
Asthenopia, defined as a subjective sensation of visual
fatigue, eye weakness, or eyestrain, is a common
condi-tion in adults1---4 and can result froma variety of causes,
includinguncorrectedrefractiveerrors,imbalanceofextra ocularmuscles,accommodativeimpairment,andimproper lighting.5,6 It can manifest itself through different
symp-toms,suchaswateryeyes,itching,doublevision, blurred vision, sore eyes, headache, dry eye sensation, and redness.6
Asthenopiaisfrequentlyassociatedwithsituationswhere the accommodative and vergence processes are more intense,suchasinthosewhoworklongperiodslookingat videodisplayunits(VDU).Althoughchildrenareusing elec-tronic devices, such as computers and videogames, with increasingfrequency,theprevalence ofasthenopia in this agegroupisunknown.1---5
Thisisanimportantgapintheliterature,becausewhen itaffectschildren,visualfatiguemayberelatedtoproblems involvingreading,writingandlearningdisability,attention, andmemory,aswellasschoolperformance.5Visualfatigue
mayalsoindicatetheexistenceofcomplexconditionssuch asdyslexia,whichrequirespecialhandling.5---8
Most studies of children have small samples and are highlyheterogeneousregardingevaluationmethods,withno standardizedtools fordiagnosis,population, andexposure conditions.
This study aimed to describe the prevalence of asthenopia and its relatedfactors in childhoodthrough a systematicreviewandmeta-analysisofobservational stud-ies.
Methods
Thissystematic reviewwasperformed in accordancewith
the Cochrane Collaboration guidelines and the PRISMA
Statement.9,10
Eligibilitycriteria
Eligibility criteria were: studies describing asthenopia
prevalence in children aged 0---18 years. Asthenopia was
definedby thepresenceofvisual fatigueor eyeweakness
during the performance of near visual tasks, writing, or
readingasreporteddirectlybychildren.Casereports,case
series,andcase-controlstudiesinwhichnodataon
preva-lencecouldbeestimatedwereexcluded.Studiesofchildren
referredtoophthalmiccareduetoeyesymptomswerealso
excluded.
If a study contained multiple publications (or
sub-studies), only the most recent publication was included,
while the other publications were used for supplemental
information.
Informationsources
The review protocol wasregistered with the institutional
researchcommittee.Thesearchcomprisedonlinedatabases
---MEDLINE(accessedviaPubMed),CochraneLibrary,LILACS,
Google Scholar, SCIELO, and EMBASE, using MeSH terms
for PubMed and Embase, and DeCS for LILACS and
SCI-ELO.The searchincluded references from1960toMay of
‘‘eyestrain’’,and‘‘visualfatigue’’(Annex1).Articlesin lan-guagesotherthanEnglishwereincluded.Toidentifyprimary studies,theauthorssearchedandcheckedforreferencelists ofpreviouslypublishedpapersandabstracts.Full-text ver-sionsofallpotentiallyrelevantarticleswereobtainedfrom electronicdatabases.
Studyselectionanddataextraction
Two investigators (MAPV and LCP), independently
evalu-ated titles and abstracts of all articles retrieved by the
searchstrategy. Allabstracts providingsufficient
informa-tionregardinginclusionandexclusioncriteriawereselected
for full-text evaluation. In the second phase, the same
reviewersindependently evaluatedthesefull-textarticles
andmade their selection in accordance withthe
eligibil-itycriteria.Disagreementsbetweenreviewersweresolved
byconsensus,and,ifadisagreementpersisted,byathird
reviewer(VDC).Patientrecruitmentperiodsandareaswere
evaluated in order to avoid possible double counting of
patients included in more than one report by the same
authors/workinggroups.
Thesametworeviewersindependentlyconducteddata
extraction,includingmethodologicalcharacteristicsofthe
studies,prevalenceofasthenopiaandrelatedfactorsusing
standardizedforms.Disagreementsweresolvedby
consen-sus.
Assessmentofriskofbias
StudyqualitywasassessedusingDownsandBlack’squality
scorefor non-randomized studies11 andcomprised of five
sections:(1)Studyquality(tenitems)---toassesstheoverall qualityof the study; (2)external validity(three items) ---todetermine the ability togeneralize thefindings of the study;(3) studybias(seven items)--- toassessbias inthe interventionandoutcomemeasure(s);(4)confoundingand selectionbias(sixitems)---todeterminebiasfromsampling orgroupassignment;(5)powerofthestudy(oneitem)---to determinewhetherfindingsareduetochance.
Tworeviewers independently performedquality assess-mentandclassifiedthestudiesasadequate,inadequate,or unclear/notreportedaccordingtoeachcriterion.
As no intervention study was selected, the maximum score possible in the present review was 12 points. Any scoresunder7pointswereconsideredinadequatefor inclu-sioninthemeta-analysis.
Dataanalysis
The outcome of meta-analysis is the summary effect or
singlegroupssummary.Inthiscase,theoutcomewas
com-binedprevalence. Prevalences werecalculatedusingdata
extractedfromtheoriginalstudies,expressedasthenumber
ofcasesdividedbytotalnumberofparticipantsevaluated.
Standard errors, variance, andweighted effectsize were
calculated,andforestplotswereproducedusingthemethod
describedbyNeyeloffetal.12
Using this model, it is possible toobtain the result of the meta-analysis of descriptive data through both fixed
and random effects. Furthermore, the model also calcu-latesheterogeneityandinconsistency(Cochran’sQtestand
I2inconsistency test)andenablestheproductionofforest
plots basedonprevalence. Dependingonthe heterogene-ityandinconsistency results,Neyeloffetal.12 proposethe
useoftherandomeffectsmodelwhenheterogeneityishigh (above 50%) or when it is believed that thereare signifi-cantdifferencesbetweenpopulations.Thus,randomeffects measureswereadoptedinthepresentstudy,consideringthe differencesamongthestudiedpopulations.Sincevariability wasassumedtobenotonlyduetosamplingerrors,butalso tovariabilityofeffectsinthepopulation,inthismodelthe weightofeachstudywasadjustedwithaconstant(v) rep-resentingvariability.11 Whennecessary,sensitivityanalysis
wasperformed, removing one study at atime and evalu-ating thepossible changesthatcouldleadtoasignificant difference.
Results
Out of 1692 potentially relevant citations retrieved from
electronic databases and searches of reference lists, 26
were identified as potentially eligible. Five of these met
theinclusioncriteria, comprisingatotalof2465subjects.
Fig.1showsthestudyflowdiagraminthisreview.The maxi-mumDownsandBlackscorewas12pointsandtheminimum was 7 points (mean=8.4). Tables 1 and 2 summarize the characteristicsofthesestudiesandmethodologicalquality. Combinedasthenopia frequency of was 19.7% (SD 6.7; 12.4---26.4%). Fig. 2 shows the prevalence forest plot. Heterogeneity measured by random effects was very low (I2=
−13.03).
The authors used different questionnaires to detect cases,andonly Tiwaryetal.adopted controlgroups.The onlypopulation-basedsamplewasthatdescribedbyIpetal. Theotherauthorsusedconveniencesamples.
Thelargeststudy,conductedbyIpetal.13evaluated1448
childrenaged6yearsandestimatedaprevalenceof12.6%. 82%ofchildrenwitheyefatiguesymptomshadnormal ocu-larexamination.Adbi14evaluated216childrenaged6to16
anddetected23.1%asthenopiaprevalence. Thesymptoms wererelatedtorefractiveerrors(myopiaandastigmatism), lowvisualacuity,andaccommodativeinsufficiency.Sterner et al.15 evaluated 72 children, aged 5---9 years, and
esti-mated an asthenopia prevalence of 26.4%, with relevant influenceofaccommodativeinsufficiency.
Tiwarietal.16,17evaluatedchildreninveryunusual
con-ditionswhoworkedasstonepolishersorintheshoe-making industry. The control groups used in both studies did not comprise workingchildrenandwere thereforeincluded in thisanalysis.Prevalencesof24.1%16and12.4%17werefound,
respectively.
Discussion
The combined frequency of asthenopia was 19.7% in this
systematic review and meta-analysis of population-based
prevalencestudies.Genderwasnotassociatedwith
differ-encesinprevalence,butchildrenagedover7yearsshowed
Records identified through database searching
(n=1692)
Screening
Included
Eligibility
Identification
Records after duplicates were removed (n=1627)
Records screened (n=1627)
Records excluded (n=1493)
Full-text articles assessed for eligibility
(n=134)
Full-text articles excluded, with reasons
(n=129) 110 inadequate design 8 full article not retrieved 1 duplicated publication
Studies included in the qualitative synthesis
(n=5)
Studies included in the quantitative synthesis
(meta-analysis) (n=5)
Figure1 PRISMA2009flowdiagram.
The relation between asthenopia and visual acuity,
binocular dysfunctions or refraction abnormalities was
controversial.Ipetal.13demonstratedthat82%ofchildren
aged6yearshavenormalocularexamination.Inthestudy conductedbyAbdi,astrongassociationwasobservedin chil-drenagedbetween6and15yearsbetweensymptomsand refractive problems (specially in myopic or astigmatic
children), low visual acuity, and accommodative insufficiency.14
Reversecausalitycouldexplainwhyasthenopiawasmore prevalentinthosewhoworeopticalcorrection.Thelower prevalenceamongchildrenundertheageof7yearsmaybe underestimatedduetothedifficultiesinunderstandingthe questionsusedfor diagnosis bysaidchildren.In thestudy
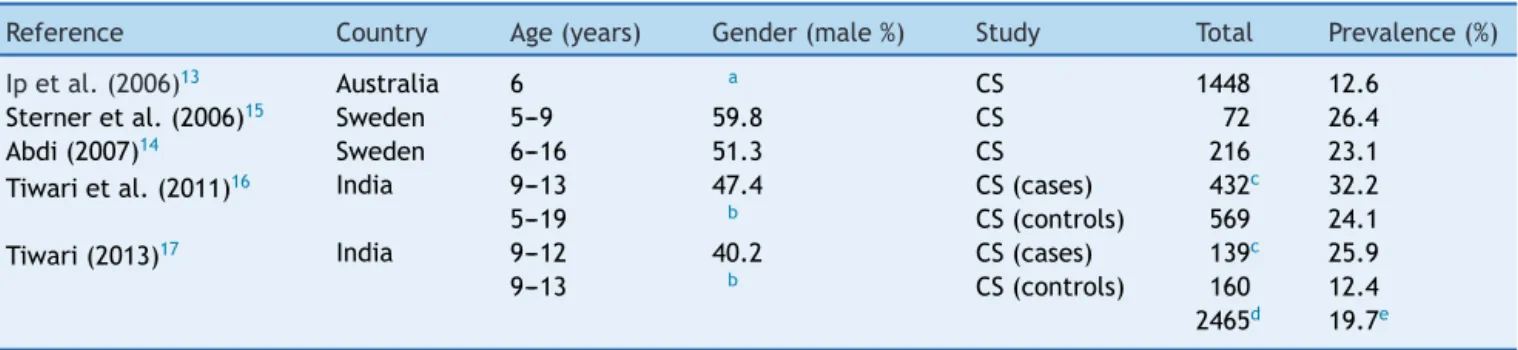
Table1 Descriptiveresultsoftheselectedstudiesofasthenopiainchildren.
Reference Country Age(years) Gender(male%) Study Total Prevalence(%)
Ipetal.(2006)13 Australia 6 a CS 1448 12.6
Sterneretal.(2006)15 Sweden 5---9 59.8 CS 72 26.4
Abdi(2007)14 Sweden 6---16 51.3 CS 216 23.1
Tiwarietal.(2011)16 India 9---13 47.4 CS(cases) 432c 32.2
5---19 b CS(controls) 569 24.1
Tiwari(2013)17 India 9---12 40.2 CS(cases) 139c 25.9
9---13 b CS(controls) 160 12.4
2465d 19.7e
a Informednogenderdifference(p=0.39). b Notinformed.
Table2 Methodologicalevaluationofincludedstudies.
Authoryear Study
quality External validity Internal validity Confusion and selection bias Sample power Downsand Blackmean score
Ipetal.(2006)13 Adequate
(5/6) Adequate (2/2) Adequate (2/2) Adequate (2/2) Adequate (1/1) 12
Sterneretal. (2006)15 Adequate (5/6) Not Adequate (0/2) Not adequate (1/2) Adequate (1/2) Not adequate (0/1) 7
Abdi(2007)14 Adequate
(5/6) Not adequate (0/2) Adequate (2/2) Not adequate (0/2) Not adequate (0/1) 7
Tiwarietal. (2011)16 Adequate (5/6) Not adequate (0/2) Not adequate (0/2) Adequate (2/2) Not adequate (0/1) 7
Tiwari(2013)17 Adequate Not
Adequate Not Adequate Adequate Not Adequate 7
8a(
±2.23)
aMeanandstandarddeviation.
conductedbySterner etal.15 thesample wasselectedby
invitation.Thisisarelevantlimitationandprobablyledto selectionbias.
Insymptomaticchildren orinchildren referredto oph-thalmic care, some associated causes were described, suchasheterophoria(1.4---8.8%),convergenceinsufficiency (6---11%), accommodative insufficiency (11.1%), amblyopia (3.6%),andstrabismus(7.3%).Simplemeasurescouldtreat most of these causes, which highlights the importance ofearlydetection.7,8,13,15,18 Notwithstanding,thesefactors
occuratthesame frequencyinchildren withnormal oph-thalmicexamination.13
Itwouldalsobeinterestingtostudychildrenwith learn-ingdisabilitiestoevaluatetheproportionoftheseproblems thatcouldbeattributedtoasthenopia. Sincemoststudies showednoimportantrelationshipbetweenasthenopiaand visualacuity,screeningonlychildrenwithvisualimpairment wouldnotdetect a significantproportion ofchildren with
asthenopia.7,8,18 The truefrequency of othersymptoms of
asthenopia and their consequences need to bestudied in greaterdetail.
Alimitationofthissystematicreviewisthesmall num-ber of studies included, even though the searches were conductedusingasensitivestrategyandwithnolanguage restrictions.Thequalityoftheindividualstudieswasquite heterogeneous regarding sample size, patient selection, methods of assessingasthenopia symptoms, andreporting bias. Nevertheless, the prevalences reported were simi-lar,exceptforthoseexposedtounusuallaboralconditions. Lowerprevalenceamongchildrenundertheageof7years mayrepresentanunderestimation,possiblybecauseofthe difficultiesinunderstandingthequestionsusedfor diagno-sisinchildrenunderthisage.Funnelplotsareappropriate andshouldbeinterpretedasrepresentativeforthis observa-tional(non-interventional)analysis.Theydonotreflectthe causaleffect,butratherdifferentprevalencevalues.Even
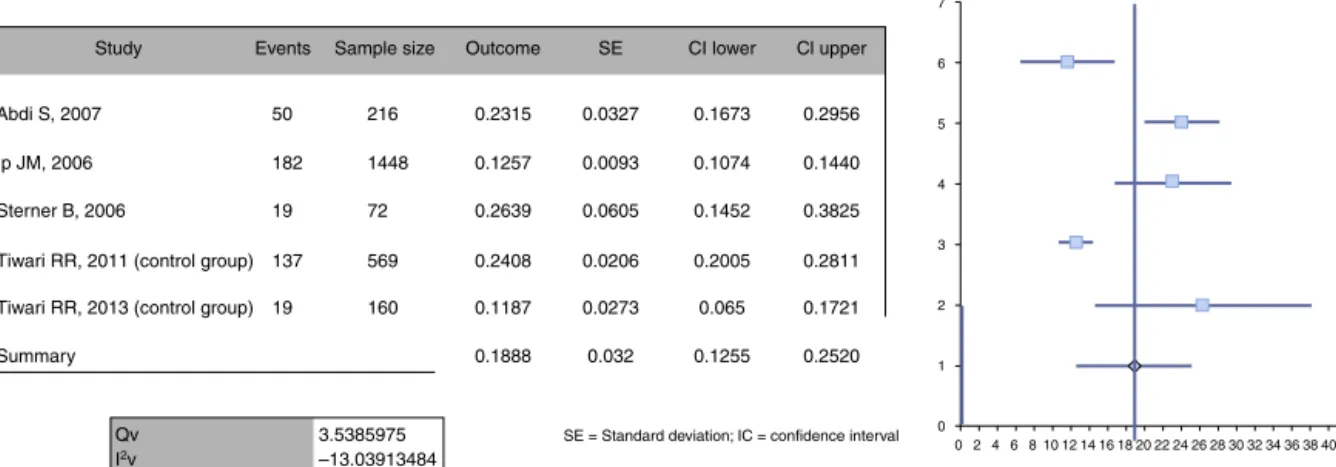
0 0 1 2 3 4 5 6 7
2468 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50
Study
Abdi S, 2007
Ip JM, 2006
50 182 19 137 19 216 1448 72 569 160 0.2315 0.1257 0.2639 0.2408 0.1187 0.1888 0.0327 0.0093 0.0605 0.0206 0.0273 0.032 0.1673 0.1074 0.1452 0.2005 0.065 0.1255 0.2956 0.1440 0.3825 0.2811 0.1721 0.2520 Sterner B, 2006
Tiwari RR, 2011 (control group)
Tiwari RR, 2013 (control group)
Summary
Qv I2v
3.5385975 –13.03913484
SE = Standard deviation; IC = confidence interval Events Sample size Outcome SE CI lower Cl upper
thoughthesquaresthatrepresentthestudieshavethesame
size,thestudyweightcanbeestimatedbytheconfidence
intervalwidth.
Themostimportantfindingofthisreviewisthescarcity
of studies enabling the evaluation of asthenopia
preva-lenceindifferentpediatricpopulations,aswellasthelack
of a standardized instrument that is quick to apply and
easy tounderstand.7,8,19---21 It is surprising thatmost
stud-ies are restricted to adults, since asthenopia in children mayhaveimportantclinicalconsequences,suchaslearning disabilities,with potentialimpactin their future.5,7,8 The
absenceof detailedknowledgeabout the trueprevalence ofasthenopiahindersaneffectiveplanningofpublichealth measuresforpreventionandtreatment.
There arelessons tobelearnedfromstudies inadults. Asthenopia symptomsin adultsincreasewithtimeof VDU
use.1---6Childrenworldwideareheavyusersofcomputersand
videogames, sometimeswithverylong periods ofuse and at increasingly earlier ages,which makesthem especially susceptible.Thus,itispossiblethatasthenopiaprevalence in children will increase in the near future, with addi-tionalconsequences for learningandschool performance. AsprevalenceisexpectedtorisewithincreasingVDUuse, more population-based studies are necessary to estimate asthenopiaprevalence andrelatedfactorsinthiscontext, aswell asitsconsequencesfor learninganddevelopment. Nonetheless,untilsuchstudieshave been conducted,this systematicreviewmayserveasareferenceforpublicand schoolpolicies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Annex
1.
Search
strategy
used
on
databases
#1 ‘‘Asthenopia’’[MeSH]OR‘‘astenopia’’OR‘‘visual
fatigue’’
#2 ‘‘Eyestrain’’[MeSH]
#3 #1AND#2
References
1.BergqvistUO,KnaveBG.Eyediscomfortandworkwithvisual displayterminals.ScandJWorkEnvironHealth.1994;20:27---33. 2.BhanderiDJ,ChoudharyS,DoshiVG.Acommunity-basedstudy of asthenopia in computer operators. Indian J Ophthalmol. 2008;56:51---5.
3.KowalskaM,ZejdaJE, BugajskaJ,BraczkowskaB,BrozekG, Mali´nskaM.Eyesymptomsinofficeemployeesworkingat com-puterstations.MedPr.2011;62:1---8.
4.NakazawaT,OkuboY,SuwazonoY,KobayashiE,KomineS,Kato N,etal.AssociationbetweendurationofdailyVDTuserand subjectivesymptoms.AmJIndMed.2002;42:421---6.
5.Handler SM,FiersonWM, Section on Ophthalmology, Council on Children with Disabilities, American Academy of Oph-thalmology,AmericanAssociationforPediatricOphthalmology and Strabismus, American Association of Certified Orthop-tics. Learning disabilities, dyslexia, and vision. Pediatrics. 2011;127:e818---56.
6.NeugebauerA, FrickeJ,RussmannW. Asthenopia: frequency andobjectivefindings.GerJOphthalmol.1992;1:122---4. 7.EvansBJ,PatelR,WilkinsAJ,LightstoneA,EperjesiF,
Speed-wellL,etal.Areviewofthemanagementof323consecutive patients seen in a specific learning difficulties clinic. Oph-thalmicPhysiolOpt.1999;19:454---66.
8.ConlonEG,LovegroveWJ,ChekalukE.Measuringvisual discom-fort.VisCogn.1999;6:637---66.
9.EggerM,Smith GD,AltmanDG.Systematicreviewsinhealth care:meta-analysisincontext.2nded.London:BMJPublishing Group;2001.
10.PRISMA --- preferred reporting items for systematic reviews
and meta-analyses [cited 2014 May 24]. Available from:
http://www.prisma-statement.org/index.htm
11.DownsSH,BlackN.Thefeasibilityofcreatingachecklistforthe assessmentofthemethodologicalqualitybothofrandomised andnon-randomisedstudiesofhealthcareinterventions.J Epi-demiolCommunityHealth.1998;52:377---84.
12.Neyeloff JL,Fuchs SC,Moreira LB. Meta-analysesand Forest plotsusingamicrosoftexcel spreadsheet:step-by-stepguide focusing on descriptive data analysis.BMC ResNotes. 2012; 5:52.
13.IpJM,RobaeiD,RochtchinaE,MitchellP.Prevalenceofeye disordersin young childrenwith eyestrain complaints.AmJ Ophthalmol.2006;142:495---7.
14.AbdiS[thesis]Asthenopiainschoolchildren.Stockholm, Swe-den:KarolinskaInstitutet;2007.
15.SternerB,GellerstedtM,SjöstromA.Accommodationandthe relationshiptosubjectivesymptomswithnearworkforyoung schoolchildren.OphthalmicPhysiolOpt.2006;26:148---55. 16.Tiwari RR,Saha A,Parikh J.Asthenopia (eyestrain)in
work-ing children of gempolishing industries. Toxicol Ind Health. 2011;27:243---7.
17.Tiwari RR.Eyestrain inworking childrenoffootwear making unitsofAgra,India.IndianPediatrics.2013;50:411---3. 18.DusekWA,PierscionekBK,McClellandJF.Anevaluationof
clin-icaltreatmentofconvergenceinsufficiencyfor childrenwith readingdifficulties.BMCOphthalmol.2011;11:21---30. 19.Felius J, Beauchamp GR, Stager DR, Van De Graaf ES,
Simonsz HJ. The amblyopia and strabismus questionnaire: Englishtranslation,validation,andsubscales.AmJOphthalmol. 2007;143:305---10.
20.KuttnerL,LePageT.Painmeasurementinchildren.CanJBehav Sci.1989;21:198---209.