Rev. Saúde Pública vol.46 número1
Texto
Imagem

Documentos relacionados
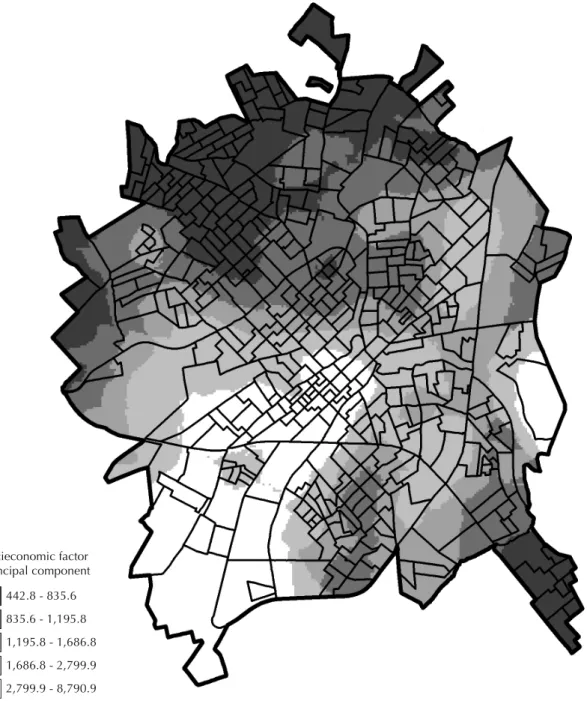
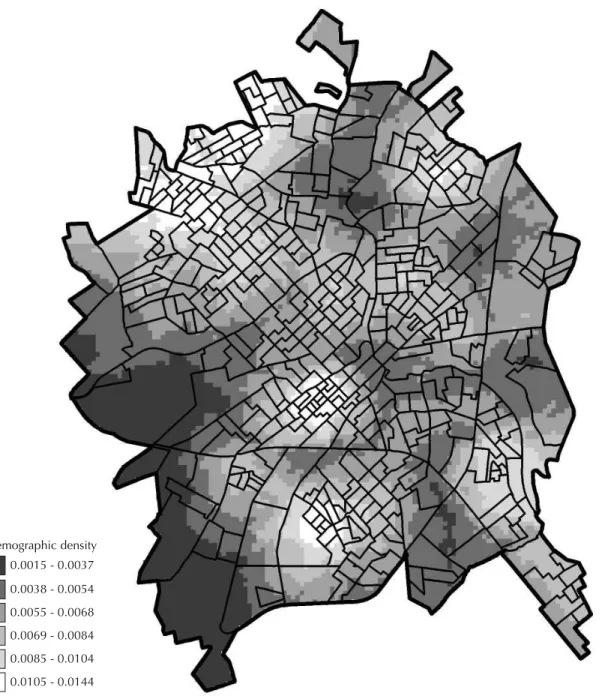
The ACCS with high relative risk and with excess risk in the northern part of the city are also areas with precarious urban infrastructure and located next to the municipality
pessoas julgam que, se tomarem pais dessa maneira, poderá infiltrar-se nelas algo de mau que receiam: por exemplo um traço dos pais, uma deficiência ou uma
Anopheles were observed in two areas with different levels of human settlement in the Cantá city, Roraima State, Northern Brazil.. The influence of the dry and rainy seasons
Efeito da temperatura (260C e 360C) e da dexametasona na diferenciação sexual A experiência decorreu nas condições experimentais descritas anteriormente. Os ovos provinham de
The composition of dichloromethane, ethanol and water extractives of the heat treated pine wood samples that were analysed corresponded to treatments at 190ºC during 2, 6 and 12 h
Distribuição Reservatório Captação Estação de Tratamento de Água Adutora de água tratada Adutora de água bruta Estação elevatória de água bruta Curso de água
We hypothesized that this depth would provide a minimum temperature range with almost constant temperatures, conducive to the development of the symbiotic fungus and the brood yet
Em um movimento de revisionismo histórico, alguns autores consideram o programa de anemia falciforme estadunidense como um passo no aprendizado ético para programas de
