w w w . r b o . o r g . b r
Original
Article
Importance
of
anatomically
locating
the
infrapatellar
branch
of
the
saphenous
nerve
in
reconstructing
the
anterior
cruciate
ligament
using
flexor
tendons
夽
,
夽夽
Julio
Cesar
Gali
∗,
André
Franc¸a
Resina,
Gabriel
Pedro,
Ildefonso
Angelo
Mora
Neto,
Marco
Antonio
Pires
Almagro,
Phelipe
Augusto
Cintra
da
Silva,
Edie
Benedito
Caetano
OrthopedicsandTraumatologyService,SchoolofMedicalSciencesandHealthofSorocaba,PontificalCatholicUniversityofSãoPaulo
(PUC-SP),Sorocaba,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8October2013 Accepted11October2013 Availableonline27October2014
Keywords:
Knee
Anteriorcruciate Ligament/innervation Anteriorcruciate Ligament/surgery
a
b
s
t
r
a
c
t
Objective:Todescribethepathoftheinfrapatellarbranchofthesaphenousnerve(IBSN)
usingthemedialjointline,anteriortibialtuberosity(ATT),tibialcollateralligamentanda horizontallineparalleltothemedialjointlinethatpassesovertheATT,asreferencepoints, inordertohelpsurgeonstodiminishthelikelihoodofinjuringthisnervebranchduring reconstructionoftheanteriorcruciateligament(ACL)usingflexortendons.
Methods:Ten frozen knees thatoriginated from amputations wereexamined. Through
anatomicaldissectionperformedwiththespecimensflexed,wesoughttofindtheIBSN, fromitsmostmedialandproximalportiontoitsmostlateralanddistalportion. Follow-ingthis,theanatomicalspecimenswerephotographedand,usingtheImageJsoftware,we determinedthedistancefromtheIBSNtothemedialjointlineandtoalowerhorizontal linegoingthroughtheATTandparalleltothefirstline.Wealsomeasuredtheangleofthe directionofthepathofthenervebranchinrelationtothislowerline.
Results:Themeanangleofthepathofthenervebranchinrelationtothelower
horizon-tallinewas17.50±6.17◦.ThemeandistancefromtheIBSNtothemedialjointlinewas
2.61±0.59cmandfromtheIBSNtothelowerhorizontalline,1.44±0.51cm.
Conclusion: TheIBSNwasfoundinallthekneesstudied.Inthreeknees,wefoundasecond
branchproximaltothefirstone.Thedirectionofitspathwasalwaysfromproximaland medialtodistalandlateral.TheIBSNwasalwaysproximalandmedialtotheATTanddistal tothemedialjointline.Themedialanglebetweenitsdirectionandahorizontallinegoing throughtheATTwas17.50±6.17◦.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:GaliJC,ResinaAF,PedroG,NetoIAM,AlmagroMAP,daSilvaPAC,CaetanoEB.Importânciadalocalizac¸ão anatômicadoramoinfrapatelardonervosafenonareconstruc¸ãodoligamentocruzadoanteriorcomtendõesflexores.RevBrasOrtop. 2014;49:625–629.
夽夽
WorkdevelopedintheSchoolofMedicalSciencesandHealthofSorocaba,PUC-SP,Sorocaba,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](J.C.Gali).
http://dx.doi.org/10.1016/j.rboe.2013.10.004
Importância
da
localizac¸ão
anatômica
do
ramo
infrapatelar
do
nervo
safeno
na
reconstruc¸ão
do
ligamento
cruzado
anterior
com
tendões
flexores
Palavras-chave:
Joelho
Ligamentocruzado anterior/inervacão Ligamentocruzado anterior/cirurgiar
r
e
s
u
m
o
Objetivo:Descreverotrajetodoramoinfrapatelardonervosafeno(RIPNS)comousodalinha
articularmedial,datuberosidadeanteriordatíbia(TAT),doligamentocolateraltibialede umalinhahorizontal,paralelaàlinhaarticularmedialequepassasobreaTAT,comopontos dereferência,afimdepoderauxiliaroscirurgiõesadiminuiraprobabilidadedelesãodesse ramonervosonareconstruc¸ãodoligamentocruzadoanterior(LCA)comtendõesflexores.
Métodos: Foram examinados 10 joelhos congelados, originados de amputac¸ões. Na
dissecac¸ãoanatômica,feitacomaspec¸asflexionadas,procuramosencontraroRIPNS,desde asuaporc¸ãomaismedialeproximalatésuaporc¸ãomaislateraledistal.Emseguida,as pec¸asanatômicasforamfotografadase,comoprogramaImageJ,determinamosadistância doRIPNSatéalinhaarticularmedialeatéumalinhahorizontalinferior,quepassapelaTAT eéparalelaàprimeira.Medimos,também,oângulodadirec¸ãodotrajetodoramonervoso emrelac¸ãoaessalinhahorizontalinferior.
Resultados: Oângulomédiodotrajetodoramonervoso,emrelac¸ãoàlinhahorizontal
infe-rior,foide17,50◦±6,17◦.AdistânciamédiadoRIPNSatéalinhaarticularmedialfoide
2,61±0,59cmeatéalinhahorizontalinferior,de1,44±0,51cm.
Conclusão: ORIPNSfoiencontradoemtodososjoelhosestudados;emtrês,encontramos
umsegundoramo,proximalaoprimeiro.Adirec¸ãodeseutrajetofoisempredeproximale medialparadistalelateral.ORIPNSestevesempreproximalemedialàTATedistalàlinha articularmedial.Aangulac¸ãomédiadesuadirec¸ão,emrelac¸ãoaumalinhahorizontalque passapelaTAT,foide17,50◦±6,17◦.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Surgicalreconstructionoftheanteriorcruciateligament(ACL) isaveryfrequently performedprocedure. Ithasbeen esti-matedthat100,000oftheseproceduresareperformedinthe UnitedStateseveryyearandthatthisisthesixthcommonest orthopedicsurgicalprocedureinthatcountry.1
Useofgraftsfrom thetendonsofthegracilisand semi-tendinosusmusclesforsurgicalreconstructionoftheACLis increasingly common,becausethese grafts withstandhigh loadsbeforefailure;theircross-sectionalarea islarge; they passeasilythoughthetunnels;theyonlyneedasmall inci-sion;theypresentlowpostoperativemorbidity;andgiverise tolowermorbidityatthedonorsite.2
However,becauseoftheiranatomicallocation,thereisa potentialriskofinjurytotheinfrapatellarbranchofthe saphe-nousnerve(IPBSN)duringharvestingofautologoustendons fromthegracilisandsemitendinosusmuscles.3–6
Intheliterature,thepercentageoccurrenceofiatrogenic lesionsoftheIPBSNduringreconstructionoftheACLusing flexortendonsrangesfrom14.9%to77%.5–10
Theorientationofthesurgicalincisionforharvestingthe tendons may, theoretically, influence the risk of injury to the IPBSN.11 Tifford et al.12 reported that verticalincisions
are perpendiculartothe nervetrunkand putthe IPBSNat risk.AccordingtoSabatandKumar,13verticalincisionshave
greater incidence of injuries to the IPBSN, with persistent
hyperesthesia,extensiveareasofsensorylossandworse sub-jectiveresults.Severalauthorshaverecommendedthatthis incisionshouldpreferentiallybeoblique.3,4,6,8,9,11,13
TheaimofourstudywastodescribethepathoftheIPBSN intheregionofflexortendonharvesting,inordertoprovide informationonwherethisbranchiscommonlyencountered andthustodiminishthechancesofiatrogenicinjuries.
Materials
and
methods
Tenfrozenkneesoriginatingfromamputationswere dissec-ted.Sixwerefrommenandfourfromwomen.Sixwereright kneesandfourwereleftknees.Thepatients’agesrangedfrom 28to72years,withameanof41.
Weremovedtheskinfromtheproximalandmedialthirds ofthelowerlegandfromthedistalandmedialthirdsofthe thigh.WethencarefullysearchedfortheIPBSNfromitsmost medial and proximalportion to its mostlateral and distal portion.Thedissectionwasperformedwiththespecimens flexed.
AfterisolatingtheIPBSN,wephotographedeachspecimen usingaNikonD3100digitalcamera.Theimagesobtainedwere evaluatedusingtheImageJsoftware.
A
B
1
α
2 3
4
x
y
Fig.1–Photographofadissectedrightknee(A)andanillustrationfromthis(B)showing:1=anteriortibialtuberosity; 2=insertionoftheflexortendons;3=IPBSN;4=tibialcollateralligament;x=distancetothemedialjointline;and y=distancetothelowerhorizontalline.
thatwentthroughthecenteroftheanteriortibialtuberosity (ATT);andalowerhorizontallinethatalsowentthroughthe ATT,perpendiculartothetwoverticallinesandparalleltothe upperhorizontalline.
Wemeasuredtheangleofthedirectionofthepathofthe nervebranchinrelationtothelowersideoftherectangle.We drewastraight-linesegmentwithitsendsatthemidpoints ofthehorizontalsidesoftherectangle.Onthissegment,we measuredthedistancesfromthenervebranchtotheupper horizontalbranchandtothelowerhorizontalbranch(Fig.1).
Results
Inalltheanatomicalspecimens,theIPBSNwasfoundtobe distaltothe medialjoint lineand proximal and medialin relationtotheATT,anditpresentedapaththatheadedfrom proximalandmedialtodistalandlateral.
Inthreeknees,wefoundasecondbranchlocated proxi-mallytothefirstanddistallytothemedialjointline(Fig.2).
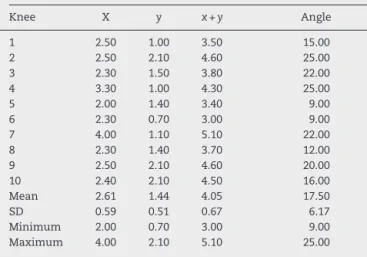
Themeanangleofthepathofthenervebranchinrelation tothelowersideoftherectanglewas17.50±6.17◦.Themean distancefromtheIPBSNatthestraight-linesegmenttothe medialjointlinewas2.61±0.59cmandtothelowersideofthe rectangle(paralleltothemedialjointline)was1.44±0.51cm. AllthesemeasurementsareshowninTable1.
Discussion
Afterleavingthe adductorcanal, thesaphenous nerve fol-lowsaposteromedialcoursetowardsthemediallineofthe knee,whereit emergesbetweenthe tendonsofthe gracilis andsemitendinosusmuscles.TheIPBSNemergesproximally tothepointwherethesaphenousnervecrossesthetendon ofthegracilisandcurvesunderthepatellatosupplytheskin overtheanteriorfaceoftheproximaltibia.3
Inharvestingtheflexortendonsofthegracilisand semi-tendinosusforACLreconstruction,thereisimminentdanger ofinjuringtheIPBSN.3–6
Ebraheim and Mekhail14 reported that injuries to this
branchcouldbecausedbytheincisionthatismadetoharvest thetendons.Figueroaetal.5believedthattheinjuryoccurred
duringtheremovalofthetendons,ratherthanduringtheskin incision.Ontheotherhand,Kartusetal.15believedthatthis
inadvertentinjurycouldoccurduringtheproceduresofskin incision,initialexposureofthetendonsordrillingthetibial tunnel.
Fig.2–Photographofadissectedrightkneethatshowsthe
mainIPBSN(widearrow)andanotherproximalbranch
Table1–DistancesfromtheIPBSNtothemedialjoint line(x)andtothelowersideoftherectangle(y),incm;
lengthofthestraight-linesegment(x+y)incmand
meanangleofthedirectionofthepathofthenerve branch(indegrees).
Distributionofthemeasurementsandangles
Knee X y x+y Angle
1 2.50 1.00 3.50 15.00
2 2.50 2.10 4.60 25.00
3 2.30 1.50 3.80 22.00
4 3.30 1.00 4.30 25.00
5 2.00 1.40 3.40 9.00
6 2.30 0.70 3.00 9.00
7 4.00 1.10 5.10 22.00
8 2.30 1.40 3.70 12.00
9 2.50 2.10 4.60 20.00
10 2.40 2.10 4.50 16.00 Mean 2.61 1.44 4.05 17.50
SD 0.59 0.51 0.67 6.17
Minimum 2.00 0.70 3.00 9.00 Maximum 4.00 2.10 5.10 25.00
TheincidenceofiatrogenicinjuriestotheIPBSN during
ACLreconstructionusingflexortendonsmayreachasmuch
as77%.5
InjurytotheIPBSNmaycausehypoesthesiainthe antero-lateral regionofthe proximal thirdofthe lower leg,3,7,11,16
painful neuroma,12 sympathetic reflex dystrophy17 or pain
on kneeling7,12,18,19 or whenpressure is applieddirectly to
thesite.20 However,thesesymptomsonlycauselimitations
todailyactivitiesinasmallpercentageofthepatientswith injuriestotheIPBSN.4,7,10,13
Explorationofthebranchesofthesaphenousnervecauses anenormouseffectontherateofsensorydeficits.6Changes
tosensitivityattheupperextremitiesareconsidered tobe ofextremeimportance.Sensoryprotectionofthelowerlimbs perhapsalsodeservesgreateffort,especiallyforthesensory areaofthekneethatisusedforkneeling.19Therefore, itis
importanttolocatethesesensorybranches,inordertoavoid injurytothem.
Ourobjectivewas todeterminethecourseoftheIPBSN intheregionofflexortendonharvesting,inordertoprovide references regardingwhere this branch is mostfrequently encounteredandthus withthepurposeofdiminishingthe likelihoodofinjurywhentheautologoustendonsofthe gra-cilisandsemitendinosusareusedinACLreconstruction.
Theanatomicalstudythatweconductedwasdonewith thespecimensflexed,inthesamewayinwhichharvesting oftheflexortendonsismostcommonlydoneinACL recon-struction.Ontheotherhand,intheliterature,someauthors havereportedthattheyconductedtheirstudieswiththeknee extended.14,20
Tifford et al.12 evaluated the effect that dynamic knee
mobilitymighthaveinrelationtothepositionofthenerve,in 20kneesfromrecentcadavers.Theyconcludedthatthenerve moveddistallywithflexionandrecommendedthatincisions intheanteriorfaceofthekneeshouldbeperformedwiththe kneeflexed,soastoavoidnerveinjuries.
Inallthekneesstudies,theIPBSNpresentedaconsistent anatomicalpattern:thedirectionofitspathwasalwaysfrom
proximalandmedialtodistalandlateral,anditwasalways locateddistallytothe medialjointlineandproximally and mediallyinrelationtotheATT.Asecondbranch,proximalto thefirstanddistaltothemedialjointline,wasfoundinthree knees.
Inastudyconductedon129kneesfromcadavers,Mochida and Kikuchi20described twopatternsfortheIPBSN: typeI,
presentin68.2%,inwhichthebranchcrossesthemedialedge ofthetibia;andtypeII,presentin31.8%,inwhichthebranch
passesproximallytothemedialjointline.
Tifford etal.12 foundtwomaintrunksofthe nervethat
penetratedthe kneegoing frommedialtolateraland from proximaltodistalinallthekneesevaluated.
Inourstudy,thepathoftheIPBSNpresentedameanangle of17.50±6.17◦inrelationtoahorizontallinepassingthrough theATT.
ItisimportanttodeterminethisangleoftheIPBSNinorder tobeabletoplananincisionforharvestingtheflexortendons thatdiminishesthepossibilityofinjuringthisbranch.Ifthe directionoftheincisionissimilartothatofthepathofthe IPBSN,itbecomeseasiertoidentifyandretractthisnerve.19
Several authors have recommended using oblique and horizontalincisionstoexposethetibialinsertionsofthe ham-stringtendonsandharvestthem,sincethereislesschance ofcausingdamagetothenervebranch,incomparisonwith verticalincisions.3,4,6,8,9,11,13
Wecanconfirmthat,inourhands,itwasnoteasyto iden-tifytheIPBSNintheanatomicalspecimensevaluatedhere, evenwithcarefuldissection.
MirzatolooeiandPisoodeh6performedmeticulous
dissec-tion in ordertofind and sparethe superficial and sensory branchesofthesaphenousnervein98patients,duringACL reconstructionusingquadrupletendonsfromthehamstrings. Despite using a relatively constant type of incision, they onlyfoundthesensory branchesin44.8%ofthecasesand attributedthistoanatomicalvariations.
Infact,the tourniquetthatisappliedduringACL recon-struction surgery may cause difficulty in differentiating betweenvesselsandnerves,andanatomicalvariationsmay bepresent.6,12,14,19–21
Asapracticalconsequenceofourstudy,wehavestarted toperformanobliqueincisionthattendstowardshorizontal, mediallytotheATT,intheregionofthehamstringinsertions, inperformingACLreconstructionusingflexortendons.Weare seekingtopushawaythesofttissuesproximally,towardsthe periosteum,inordertodrillthetunnels.Webelievethatin thisway,wemaydiminishthechanceofinjurytothesensory branchofthesaphenousnerve.
Conclusion
relationto a horizontal line passingthrough the ATTwas 17.50±6.17degrees.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BrownCHJr,CarsonEW.Revisionanteriorcruciateligament
surgery.ClinSportsMed.1999;18(1):109–71.
2. BartlettRJ,ClatworthyMG,NguyenTN.Graftselectionin
reconstructionoftheanteriorcruciateligament.JBoneJoint
SurgBr.2001;83(5):625–34.
3. PagnaniMJ,WarnerJJ,O’BrienSJ,WarrenRF.Anatomic
considerationsinharvestingthesemitendinosusandgracilis
tendonsandatechniqueofharvest.AmJSportsMed.
1993;21(4):565–71.
4. BoonJM,VanWykMJ,JordaanD.Asafeareaandanglefor
harvestingautogenoustendonsforanteriorcruciateligament
reconstruction.SurgRadiolAnat.2004;26(3):167–71.
5. FigueroaD,CalvoR,VaismanA,CamperoM,MoragaC.Injury
totheinfrapatellarbranchofthesaphenousnerveinACL
reconstructionwiththehamstringstechnique:clinicaland
electrophysiologicalstudy.Knee.2008;15(5):360–3.
6. MirzatolooeiF,PisoodehK.Impactofexplorationofsensory
branchesofsaphenousnerveinanteriorcruciateligament
reconstructivesurgery.ArchIranMed.2012;15(4):219–22.
7. SpicerDD,BlaggSE,UnwinAJ,AllumRL.Anteriorknee
symptomsafterfour-strandhamstringtendonanterior
cruciateligamentreconstruction.KneeSurgSports
TraumatolArthrosc.2000;8(5):286–9.
8. MochizukiT,MunetaT,YagishitaK,ShinomiyaK,SekiyaI.
Skinsensorychangeafterarthroscopically-assistedanterior
cruciateligamentreconstructionusingmedialhamstring
tendonswithaverticalincision.KneeSurgSportsTraumatol
Arthrosc.2004;12(3):198–202.
9. PapastergiouSG,VoulgaropoulosH,MikalefP,ZiogasE,
PappisG,GiannakopoulosI.Injuriestotheinfrapatellar
branch(es)ofthesaphenousnerveinanteriorcruciate
ligamentreconstructionwithfour-strandhamstringtendon
autograft:verticalversushorizontalincisionforharvest.
KneeSurgSportsTraumatolArthrosc.2006;14(8):789–93.
10.SandersB,RolfR,McClellandW,XerogeanesJ.Prevalenceof
saphenousnerveinjuryafterautogenoushamstringharvest:
ananatomicandclinicalstudyofsartorialbranchinjury.
Arthroscopy.2007;23(9):956–63.
11.KjaergaardJ,FaunøLZ,FaunøP.SensibilitylossafterACL
reconstructionwithhamstringgraft.IntJSportsMed.
2008;29(6):507–11.
12.TiffordCD,SperoL,LukeT,PlancherKD.Therelationshipof
theinfrapatellarbranchesofthesaphenousnerveto
arthroscopyportalsandincisionsforanteriorcruciate
ligamentsurgery.Ananatomicstudy.AmJSportsMed.
2000;28(4):562–7.
13.SabatD,KumarV.Nerveinjuryduringhamstringgraft
harvest:aprospectivecomparativestudyofthreedifferent
incisions.KneeSurgSportsTraumatolArthrosc.
2013;21(9):2089–95.
14.EbraheimNA,MekhailAO.Theinfrapatellarbranchofthe
saphenousnerve:ananatomicstudy.JOrthopTrauma.
1997;11(3):195–9.
15.KartusJ,MovinT,KarlssonJ.Donor-sitemorbidityand
anteriorkneeproblemsafteranteriorcruciateligament
reconstructionusingautografts.Arthroscopy.
2001;17(9):971–80.
16.KartusJ,MagnussonL,StenerS,BrandssonS,ErikssonBI,
KarlssonJ.Complicationsfollowingarthroscopicanterior
cruciateligamentreconstruction.A2–5-yearfollow-upof604
patientswithspecialemphasisonanteriorkneepain.Knee
SurgSportsTraumatolArthrosc.1999;7(1):
2–8.
17.PoehlingGG,PollockFEJr,KomanLA.Reflexsympathetic
dystrophyofthekneeaftersensorynerveinjury.Arthroscopy.
1988;4(1):31–5.
18.CorryIS,WebbJM,ClingelefferAJ,PinczewskiLA.
Arthroscopicreconstructionoftheanteriorcruciateligament.
Acomparisonofpatellartendonautograftandfour-strand
hamstringtendonautograft.AmJSportsMed.
1999;27(4):444–54.
19.HunterLY,LouisDS,RicciardiJR,O’ConnorGA.The
saphenousnerve:itscourseandimportanceinmedial
arthrotomy.AmJSportsMed.1979;7(4):
227–30.
20.MochidaH,KikuchiS.Injurytoinfrapatellarbranchof
saphenousnerveinarthroscopickneesurgery.ClinOrthop
RelatRes.1995;320:88–94.
21.ArthornthurasookA,Gaew-ImK.Studyoftheinfrapatellar