w w w . r b o . o r g . b r
Original
Article
Radiographic
study
on
the
tibial
insertion
of
the
posterior
cruciate
ligament
夽
Julio
Cesar
Gali
∗,
Paulo
Esquerdo,
Marco
Antonio
Pires
Almagro,
Phelipe
Augusto
Cintra
da
Silva
FaculdadedeCiênciasMédicasedaSaúdedeSorocaba,PontifíciaUniversidadeCatólicadeSãoPaulo,Sorocaba,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5February2014 Accepted11June2014 Availableonline17April2015
Keywords:
Tibia
Posteriorcruciate ligament/radiography Cadaver
a
b
s
t
r
a
c
t
Objective:Toestablishtheradiographicdistancesfromposteriorcruciateligament(PCL) tib-ialinsertionscenterstothelateralandmedialtibialcortexintheanteroposteriorview,and fromthesecenterstothePCLfacetmostproximalpointonthelateralview,inordertoguide anatomicaltunnelsdrillinginPCLreconstructionandfortunnelpositioningpostoperative analysis.
Studydesign:Controlledlaboratorystudy.
Methods:Twentycadaverkneeswereevaluated.ThePCL’sbundlestibialinsertionswere identifiedandmarkedoutusingmetaltags,andthekneeswereradiographed.Onthese radiographs,thebundlesinsertionsitescenterlocationrelativetothetibialmediolateral measure,andthedistancesfromthemostproximalPCLfacetpointtothebundle’sinsertion weredetermined.AllmeasureswerecalculatedusingtheImageJsoftware.
Results:On the anteroposterior radiographs, the mean distancefrom the anterolateral (AL)bundle insertion center to the medial tibialedge was 40.68±4.10mm; the mean distancefromtheposteromedial(PM)bundleinsertioncentertothemedialtibialedge was38.74±4.40mm.Onthelateralradiographs,themeandistancesfromthePCLfacet mostproximalpointto ALandPM bundlesinsertioncenters were5.49±1.29mm and 10.53±2.17mmrespectively.
Conclusions:ItwaspossibletoestablisharadiographicpatternforPCLtibialbundles inser-tions,whichmaybeusefulforintraoperativetunnelslocationscontrolandforpostoperative tunnelspositionsanalysis.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedintheFaculdadedeCiênciasMédicasedaSaúdedeSorocaba,PontifíciaUniversidadeCatólicadeSãoPaulo,Sorocaba, SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](J.C.Gali). http://dx.doi.org/10.1016/j.rboe.2015.04.003
Estudo
radiográfico
da
inserc¸ão
tibial
do
ligamento
cruzado
posterior
Palavras-chave:
Tíbia
Ligamentocruzado posterior/radiografia Cadáver
r
e
s
u
m
o
Objetivo: Estabelecerasdistânciasradiográficasdoscentrosdasinserc¸õestibiaisdo liga-mentocruzadoposterior(LCP)atéascorticaismedialelateraldatíbia,nasradiografiasem anteroposterior,edessescentrosatéopontomaisproximaldafacetadoLCP,nas radio-grafiasemperfil,paraquepossamorientaracriac¸ãodetúneisanatômicosnareconstruc¸ão doLCPeparaanálisepós-operatóriadoposicionamentodostúneis.
Desenho: Estudolaboratorialcontrolado.
Métodos:Vintejoelhosdecadáveresforamavaliados.Asinserc¸õestibiaisdasbandasdoLCP foramidentificadasedemarcadascommarcadoresmetálicoseosjoelhosforam radiografa-dos.Nasradiografiasdeterminamosalocalizac¸ãodocentrodeinserc¸ãodasbandasrelativa àmedidamediolateraldatíbiaeasdistânciasdopontomaisproximaldafacetadoLCPatéo centrodeinserc¸ãodasbandas.TodasasmedidasforamcalculadascomosoftwareImageJ.
Resultados:Nasradiografiasemanteroposterioradistânciamédiaentreocentrodainserc¸ão dabandaanterolateral(AL)atéabordamedialdatíbiafoide40,68±4,10mm;adistância entreocentrodeinserc¸ãodabandaposteromedial(PM)atéabordamedialdatíbiafoi,em média,de38,74±4,40mm.Nasradiografiasemperfilasdistânciasmédiasentreoponto maisproximaldafacetadoLCPeoscentrosdeinserc¸ãodasbandasALePMforamde 5,49±1,29mme10,53±2,17mm,respectivamente.
Conclusões:Foipossívelestabelecerumpadrãoradiográficodasinserc¸õestibiaisdasbandas doLCPquepodeserútilparaocontroleintraoperatóriodalocalizac¸ãodostúneisepara análisepós-operatóriadaposic¸ãodostúneis.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Anatomicalpositioningofthegraftisarequisitefor achiev-ing a good result from posterior cruciate ligament (PCL) reconstructions.1–3 Success in surgical treatments for PCL
injuries is related to precise restoration of PCL anatomy.4
In a recent published paper, the anatomical location and measurements of the tibial insertions of the PCL were described.5
ImproperpositioningofthetunnelsinPCLreconstruction maycauseshorteningorlengtheningofthegraftduringknee flexionand,ultimately,failure.6
Forthefunctionofthereconstructedligamenttobe nor-mal,anatomicalreconstructionofitsanterolateral(AL)and posteromedial (PM) bands should be envisaged, giventhat biomechanicalstudieshave shownthatPCLreconstruction withadoublebandissuperiortoreconstructionwithasingle band.7–9
Correctdemarcation oftheinsertionsitesofthe ALand PMbandsofthePCLandthecorrelatedradiographicimages mightassistinprovidinggreaterprecisionforsurgical recon-structionofthisligament.10–12
Computedtomographyisapotentiallyusefultoolfor eval-uating the locations of bone tunnels, which even has the possibilityofgeneratingthree-dimensionalreconstructions,13
althoughtheiruseintheoperatingtheaterisnotpossible. Magneticresonanceislesseffectiveforevaluatingthe posi-tioningofthetunnelsincruciateligamentreconstructions, becauseinterferencescrewsorothermetalartifactsusedin graftfixationmayinterferewithimagequality.11
Theaimofourstudywastodefinetheradiographic dis-tancesfromthecentersofthetibialinsertionsofthebands oftheposteriorcruciateligamenttothemedialand lateral corticalboneofthetibia,onradiographsinanteroposterior view,andfromthesecenterstothemostproximalpointofthe facetofthePCL,onradiographsinlateralview,sothatthese mightguidethecreationofanatomicaltunnelsduring opera-tionsandsothatthesemightserveasanalyticalparameters forpositioningbonetunnelsaftertheseoperations.
Methods
TheinsertionsoftheALandPMbandsofthePCLwere eval-uated in20 anatomicalspecimensfromthe knees ofadult cadavers(11rightand9leftknees).Thespecimenswerenot pairedandtheirsexandagedatawereunknown.Alltheknees presentedintactanteriorandposteriorcruciateligamentsand noneofthemshowedanymacroscopicsignsofarthrosis.
Beforethedissection,thespecimenswerefixedin10% for-moland wereconservedinamixtureof2.5%phenol,2.5% formoland1%sodiumchloride.Followingthis,theywerekept inliquidglycerinfor60days.
PM
AL
Fig.1–Photographofthedissectedspecimenshowingthe insertionsoftheanterolateral(AL)andposteromedial(PM) bands.
Digitalradiographswereproducedinanteroposterior(AP) view,withthe kneeextended,and inabsolutelateral view, withthekneeflexedat30◦.Theradiographswereproduced
usingthefollowingtechnicalstandardization:distancefrom the tube tothe specimens of120cm; voltage of48kVand dosageof5mAs.
OntheAPradiographs,thelocationsoftheinsertionsites oftheALandPMbandswereestablished,inpercentages,from
theratioofthedistancefromtheinsertionpointofeachband tothemedialborderofthetibia,dividedbythelargest medio-lateralmeasurementofthesuperiortibialjointface(Fig.2).
Onthelateralradiographicimages,wetracedalineabove theinclinedregionofthemostproximalportionofthetibia, i.e.theinsertionsiteofthePCL,definedbyMoormanetal. asthe“facetofthePCL”.14Wemeasuredthesizeofthefacet
ofthePCLandthedistancesfromthemostproximalpoint ofthislinetotheinsertionsoftheALandPMbands(Fig.3). TheImageJsoftwarewasusedtomeasureallofthedistances describedabove.
Results
On all theradiographic imagesanalyzed,the center ofthe insertionofthePMbandwasdistalandmedialtothecenter oftheinsertionoftheALband.
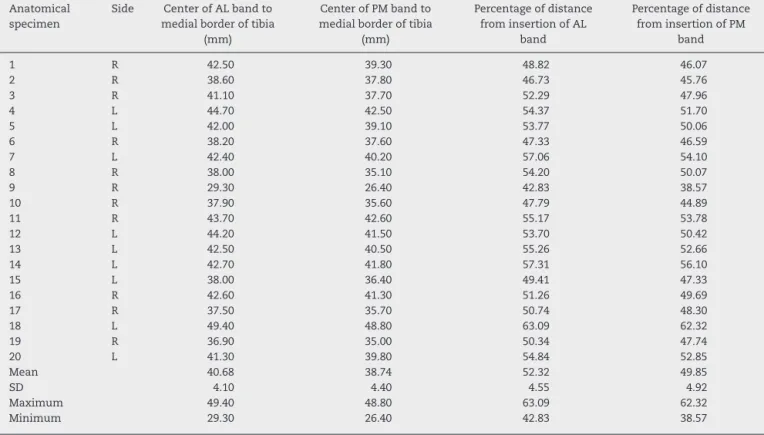
Themeandistancefromthecenteroftheinsertionofthe ALbandtothemedialborderofthetibiawas40.68±4.10mm, whichcorrespondedto52.32±4.55%ofthemediolateral mea-surementofthesuperiortibialjointface.
InrelationtothePMband,themeandistancebetweenthe centerofitsinsertionandthemedialborderofthetibiawas 38.74±4.40mm,equivalentto49.85±4.92%ofthe measure-mentofthedistancebetweenthemedialandlateralborders ofthesuperiortibialjointface.Thedatarelatingtothe tib-ialinsertionsofthePCLonAPradiographsarepresentedin Table1.
Table1–DistanceinmmfromthecentersoftheinsertionsoftheALandPMbandstothemedialborderofthetibiaand thisdistanceasapercentageofthegreatestmediolateraldistancefromthesuperiortibialjointface,onradiographsin APview.
Anatomical specimen
Side Facetofthe PCL(mm)
Distancefromthemostproximalpointofthefacet ofthePCLtotheinsertionoftheband
AL(mm) PM(mm)
1 R 15.87 5.34 9.58
2 L 15.77 6.62 11.99
3 R 12.29 4.16 7.9
4 L 13.47 4.33 9.61
5 L 13.46 3.99 9.75
6 R 13.2 4.27 8.7
7 R 13.13 5.18 9.29
8 R 14.32 4.15 9.51
9 L 12.66 5.47 7.75
10 R 18.42 6.07 12.24
11 L 22.03 8.74 15.29
12 L 15.04 5.79 11.82
13 R 15.77 6.1 11.33
14 R 17.8 5.81 9.43
15 L 15.72 6.26 8.92
16 R 19.2 7.85 15.03
17 R 14.67 4.15 8.12
18 R 17.08 6.32 12.68
19 L 13.71 4.66 9.76
20 L 15.1 4.59 11.91
Mean 15.436 5.493 10.531
SD 2.472 1.291 2.176
Maximum 22.030 8.740 15.290
y
AL
PM
x
Fig.2–RadiographinAPviewshowingtheinsertionsof theanterolateral(AL)andposteromedial(PM)bands;
x=distancefromtheinsertionpointofthebandtothe
medialborderofthetibia;y=greatestmediolateraldistance
fromthesuperiortibialjointface.
Inevaluatingthelateral-viewradiographs,themeanlength ofthefacetofthePCLwas15.43±2.47mm.Themean dis-tancesbetweenthemostproximalpointofthefacetofthe PCLandthecentersofinsertionoftheALandPMbandswere 5.49±1.29mmand10.53±2.17mm,respectively(Table2).
Discussion
Thegeneral orthopedicprecept that surgery should repro-duce anatomy suggests that grafts placed far from their trueanatomicalinsertionmaypresent impairedfunction.14
Thus,radiographicguidelinesforplacingtunnelsinsurgical treatmentsforPCLinjuriesare essential foraccomplishing anatomicalreconstructions.15
TheradiographiclocationsofthebandsofthePCLare ref-erencepointsthatareindependentofthesizeoftheknee. Intraoperativefluoroscopymaythereforebeahelpfultoolfor correctplacementofthetunnels.12
Biomechanicalstudieshaveshownthatreconstructionof thePCLusingadoublebandissuperiortoreconstructionwith asingleband.7–9However,themostimportantfactorforgood
resultsisperfectanatomicalplacementofthebands.9Some
studiesonthePCLhavenotdescribedthelocationsoftheAL andPMbandsseparately.10,12,16
WeobservedthatthecenterofinsertionofthePMbandwas alwaysmedialanddistaltothecenterofinsertionoftheAL band.OnAPradiographs,themeandistancesfromthecenters ofinsertionoftheALandPMbandstothemedialborderofthe tibiawere40.68±4.10mmand38.74±4.40mm,respectively. ThecenterofinsertionoftheALbandwasatalocationthat correspondedto52.32±4.55%ofthemediolateral
measure-PM
AL
Fig.3–Radiographinlateralviewshowingthelineabove the“facetofthePCL”andtheinsertionsoftheanterolateral (AL)andposteromedial(PM)bands.
mentofthesuperiortibialjointface.Forthecenterofinsertion ofthePMband,thislocationrepresented49.85±4.92%ofthe measurementofthesuperiortibialjointface.
Lorenzetal.12studiedtheinsertionofthePCLin16knees
fromcadavers.Theyfoundthatthecommonpointofthe inser-tion of the PCLwas locatedat49±2%of the mediolateral diameter ofthe tibia,inrelationtothemedialborder.Ina study on10kneesfrom cadaversusingcomputed tomogra-phy,Greineretal.13 foundthatthemean distancebetween
thetibialinsertionofthePCLandthemedialborderofthe tib-ialplateauwas36.6mm,equivalentto49%ofthetotalwidth ofthetibialplateau.
Inastudyon39kneesfromcadavers,Edwardsetal.17found
thattherewasastrongcorrelationbetweenthepositionsof thecentersoftheALandPMbandsandthewidthofthe tib-ialplateau,whichwas48±4%fortheALband(p<0.001)and 48±5%forthePMband(p<0.002).
According toOsti etal.,18 who evaluated15 kneesfrom
humancadavers,thecentersofinsertionoftheALandPM bandswerefoundat47.88%and50.93%ofthetotal medio-lateraltibialdiameter,respectively.Takahashietal.19studied
33tibiasfromcadaversandfoundthatthedistancesfromthe medialborderofthejointcartilageofthetibialplateautothe centersofthetibialinsertionsoftheALandPMbands,in rela-tiontothewidthofthetibialplateau,were51.0%and50.0%, respectively.
Inoursample,thedistancefromthemostproximalpoint ofthelinetracedabovethefacetofthePCLtotheinsertion oftheALbandwas5.49±1.29mmanditwas10.53±2.17mm forthePMband.AccordingtoOstietal.,18themeasurements
Table2–LengthofthefacetofthePCLanddistancefromthemostproximalpointofthefacettothecentersofthe insertionsoftheALandPMbandsofthePCL,onradiographsinlateralview.
Anatomical specimen
Side CenterofALbandto medialborderoftibia
(mm)
CenterofPMbandto medialborderoftibia
(mm)
Percentageofdistance frominsertionofAL
band
Percentageofdistance frominsertionofPM
band
1 R 42.50 39.30 48.82 46.07
2 R 38.60 37.80 46.73 45.76
3 R 41.10 37.70 52.29 47.96
4 L 44.70 42.50 54.37 51.70
5 L 42.00 39.10 53.77 50.06
6 R 38.20 37.60 47.33 46.59
7 L 42.40 40.20 57.06 54.10
8 R 38.00 35.10 54.20 50.07
9 R 29.30 26.40 42.83 38.57
10 R 37.90 35.60 47.79 44.89
11 R 43.70 42.60 55.17 53.78
12 L 44.20 41.50 53.70 50.42
13 L 42.50 40.50 55.26 52.66
14 L 42.70 41.80 57.31 56.10
15 L 38.00 36.40 49.41 47.33
16 R 42.60 41.30 51.26 49.69
17 R 37.50 35.70 50.74 48.30
18 L 49.40 48.80 63.09 62.32
19 R 36.90 35.00 50.34 47.74
20 L 41.30 39.80 54.84 52.85
Mean 40.68 38.74 52.32 49.85
SD 4.10 4.40 4.55 4.92
Maximum 49.40 48.80 63.09 62.32
Minimum 29.30 26.40 42.83 38.57
otherhand,accordingtoRacanelliandDrez,10inastudyon12
kneesfromhumancadavers,thedistancefromthecommon insertionofthePCLtothetibialjointfacewas8mm.
WefullyagreewiththestatementbyJohannsenetal.15that
themostimportantfindingsrelatetothelateralradiographic view,whichismorefrequentlyusedduringoperations.
Thedifferentevaluationmeasurementsthatweusedhere canbeappliedtosurgicalreconstructionsofthePCL,bothas anaidforcreatinganatomicaltunnelsandforpostoperative verification.
Conclusions
Ourstudyestablishedaradiographicmodelforidentifyingthe sitesofthe tibialinsertionsofthe bands ofthePCLbased onthedistancesfromthe centersoftheirinsertionstothe medialandlateralcorticalbonesofthetibiaandfromthese centerstothemostproximalpointofthefacetofthePCL.The resultsfromourinvestigationmaycontributetoward anatom-icalreconstruction of the PCL, sincecorrect positioning of the tunnels can bechecked using fluoroscopy, before they aredrilled.Thedataobtainedmayalsoaidinanalyzingthe locationsofthetunnels,aftertheoperation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.PetersenW,LenschowS,WeimannA,StrobelMJ,RaschkeMJ, ZantopT.Importanceoffemoraltunnelplacementin double-bundleposteriorcruciateligamentreconstruction: biomechanicalanalysisusingarobotic/universal
force-momentsensortestingsystem.AmJSportsMed. 2006;34(3):456–63.
2.YasudaK,KitamuraN,KondoE,HayashiR,InoueM. One-stageanatomicdouble-bundleanteriorandposterior cruciateligamentreconstructionusingtheautogenous hamstringtendons.KneeSurgSportsTraumatolArthrosc. 2009;17(7):800–5.
3.McGuireDA,HendricksSD.Comparisonofanatomicversus non-anatomicplacementoffemoraltunnelsinAchilles double-bundleposteriorcruciateligamentreconstruction. Arthroscopy.2010;26(5):658–66.
4.HarnerCD,XerogeanesJW,LivesayGA,CarlinGJ,SmithBA, KusayamaT,etal.Thehumanposteriorcruciateligament complex:aninterdisciplinarystudy.Ligamentmorphology andbiomechanicalevaluation.AmJSportsMed.
1995;23(6):736–45.
5.GaliJC,OliveiraHC,LisboaBCB,DiasBD,CasimiroFG, CaetanoEB.Inserc¸õestibiaisdoligamentocruzadoposterior: anatomiatopográficaeestudomorfométrico.RevBrasOrtop. 2013;48(3):263–7.
6.SaddlerSC,NoyesFR,GroodES,KnochenmussDR,HefzyMS. Posteriorcruciateligamentanatomyandlength-tension behaviorofPCLsurfacefibers.AmJKneeSurg.
1996;9(4):194–9.
8. HarnerCD,JanaushekMA,KanamoriA,YagiM,VogrinTM, WooSL.Biomechanicalanalysisofadouble-bundleposterior cruciateligamentreconstruction.AmJSportsMed.
2000;28(2):144–51.
9. MannorDA,ShearnJT,GroodES,NoyesFR,LevyMS. Two-bundleposteriorcruciateligamentreconstruction.An invitroanalysisofgraftplacementandtension.AmJSports Med.2000;28(6):833–45.
10.RacanelliJA,DrezDJr.Posteriorcruciateligamenttibial attachmentanatomyandradiographiclandmarksfortibial tunnelplacementinPCLreconstruction.Arthroscopy. 1994;10(5):546–9.
11.BrandJCJr,ColeJ,SumidaK,CabornDN,JohnsonDL. Radiographicanalysisoffemoraltunnelpositionin postoperativeposteriorcruciateligamentreconstruction. Arthroscopy.2002;18(7):688–94.
12.LorenzS,ElserF,BruckerPU,ObstT,ImhoffAB.Radiological evaluationoftheanterolateralandposteromedialbundle insertionsitesoftheposteriorcruciateligament.KneeSurg SportsTraumatolArthrosc.2009;17(6):683–90.
13.GreinerP,MagnussenRA,LustigS,DemeyG,NeyretP,Servien E.Computedtomographyevaluationofthefemoralandtibial attachmentsoftheposteriorcruciateligamentinvitro.Knee SurgSportsTraumatolArthrosc.2011;19(11):1876–83.
14.MoormanCT3rd,ZaneMS,BansaiS,CinaSJ,WickiewiczTL, WarrenRF,KasetaMK.Tibialinsertionoftheposterior cruciateligament:asagittalplaneanalysisusinggross, histologic,andradiographicmethods.Arthroscopy. 2008;24(3):269–75.
15.JohannsenAM,AndersonCJ,WijdicksCA,EngebretsenL, LaPradeRF.Radiographiclandmarksfortunnelpositioningin posteriorcruciateligamentreconstructions.AmJSportsMed. 2013;41(1):35–42.
16.LeeYS,RaHJ,AhnJH,HaJK,KimJG.Posteriorcruciate ligamenttibialinsertionanatomyandimplicationsfortibial tunnelplacement.Arthroscopy.2011;27(2):182–7.
17.EdwardsA,BullAM,AmisAA.Theattachmentsofthefiber bundlesoftheposteriorcruciateligament:ananatomic study.Arthroscopy.2007;23(3):284–90.
18.OstiM,TschannP,KünzelKH,BenedettoKP.Anatomic characteristicsandradiographicreferencesofthe anterolateralandposteromedialbundlesoftheposterior cruciateligament.AmJSportsMed.2012;40(7):1558–63. 19.TakahashiM,MatsubaraT,DoiM,SuzukiD,NaganoA.