SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Review
Article
Understanding
posterior
meniscal
roots
lesions:
from
basic
science
to
treatment
夽
Raphael
Serra
Cruz
a,b,∗,
Marcio
Balbinotti
Ferrari
a,b,
Leonardo
Metsavaht
b,
Robert
F.
LaPrade
a,caSteadmanPhilipponResearchInstitute,Vail,UnitedStates bInstitutoBrasildeTecnologiasdaSaúde,RiodeJaneiro,RJ,Brazil cTheSteadmanClinic,Vail,UnitedStates
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30June2016 Accepted14July2016 Availableonline26July2017
Keywords:
Kneeinjuries
Knee/anatomy&histology Jointinstability
Surgicalprocedures,operative Menisci
a
b
s
t
r
a
c
t
Thevariabilityofsymptomsandthefactthattheyarenoteasilyrecognizedinimaging stud-iesmakethediagnosisandtreatmentofposteriormeniscalrootslesionsachallengingtask totheorthopedist.Inrecentyears,amorepreciseunderstandingoftheanatomyand biome-chanicalimpairofthekneejointinthesecaseshasenabledgreatadvancesintherapeutic approaches.Well-documentedstudieshaveshownthattherepairoftheselesionspresents superiorfunctionalandclinicalimprovementwhencomparedwithmeniscectomy. How-ever,theprogressionofdegenerativejointchangesinthelong-termstillexhibitsconflicting results.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Compreendendo
as
lesões
das
raízes
posteriores
dos
meniscos:
da
ciência
básica
ao
tratamento
Palavras-chave:
Traumatismosdojoelho Joelho/anatomia&histologia Instabilidadearticular Procedimentoscirúrgicos operatórios
Meniscos
r
e
s
u
m
o
Avariabilidadedasintomatologiaeofatodenãoseremfacilmentereconhecidasnosexames de imagemtornamodiagnóstico eotratamentodas lesõesdasraízes posteriores dos meniscos tarefasdesafiadoras paraoortopedista.Nos últimosanos,umacompreensão maisprecisadaanatomiaedocomprometimentobiomecânicodaarticulac¸ãodojoelho nessaslesõestêmpossibilitadograndesavanc¸osnasabordagensterapêuticas.Estudosbem
夽
StudyconductedinapartnershipoftheInstitutoBrasildeTecnologiasdaSaúde,RiodeJaneiro,RJ,Brazil,withtheSteadman-Philippon ResearchInstitute,Vail,UnitedStates.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](R.S.Cruz).
http://dx.doi.org/10.1016/j.rboe.2017.07.005
documentadosdemonstramqueoreparodessaslesõesofereceumamelhoriaclínicae funcionalsuperioràmeniscectomia.Entretanto,osresultadosdaprogressãodasalterac¸ões degenerativasarticularesemlongoprazoaindasãoconflitantes.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Inthepast,lesionsofthemeniscalrootswereunderdiagnosed andoftenunrecognized,butnowtheyarebetterunderstood and have been biomechanically proven to be a source of overloadinthekneejoint.1–6Theyarepossiblyrelatedto early-onset osteoarthritis.1,7–9 Thefirst descriptionofameniscal rootlesionintheliteraturewasmadebyPagnanietal.,10who in1991describedtheprocessofextrusionofthemedial menis-cusinafootballplayer.Historically,thistypeoflesionwas treatedbypartialor totalmeniscectomy,which,despiteits goodshort-termsubjectiveresults,presentedahigherriskof long-termjointdegeneration.11
Themenisciplayimportantrolesintheknee;theirintegrity isessential forthe properfunctioning ofthe joint.1,12,13 In addition to sharing the loads and reducing the joint con-tactpressurebyincreasingthecontactsurfacebetweenthe femurand tibia,12 other functionsassigned tothe menisci areproprioception,14stabilization,15lubrication,16and nutri-tionofthejointcartilage.17Themeniscalrootsareessential formaintaining the meniscal abilitytoconvert axial loads intocircumferentialtension.1,5 Biomechanicalstudiesshow thatlesionsinthesestructuresarecomparabletoacomplete meniscectomy.1
Aslesionsoftheposteriorrootofthemeniscusarethemost frequently reported in the literature,18,19 this study aimed toprovidethesurgeonwithacomprehensivereviewofthis importantconditioninordertofacilitateitsunderstanding, diagnosis,andtreatment.
Anatomy
and
composition
Knowledgeoftheanatomyofmeniscalrootsisimportantnot onlytoallowapreciserepairincasesofinjury, butalsoto preventiatrogenicdamageduringproceduresclosetotheir location,suchasreconstructionoftheanteriorcruciate lig-ament(ACL)orintramedullarytibialnailing.Meniscalroots aredefinedastheinsertionofthemeniscalhorns intothe tibialplateau,andextendtoadistanceof0.9mmfromthe attachmentsite.20Respectingsomecharacteristics,theroots ofthe meniscusarebasicallyformedbyadensefibercore, surroundedbyadditionalfibers.1,21,22Histologically,meniscal rootshaveastructuresimilartoatypicalenthesis,comprised offour zones: meniscus fibers, non-calcified fibrocartilage, fibrocartilage,andcalcifiedbone.23
Inadditiontothequalitativeanatomy,itisimportantthat thesurgeonisfamiliarwiththequantitativedescriptionsof relevantsurgical landmarks when performing arthroscopic procedures.
Medialmeniscusposteriorroot(MMPR)
The additional fibers of the MMPR were first described by Anderson et al.24 asshiny white fibers (SWF). These fibers increase the attachment area of the medial meniscus to theposteriorportionoftheplateau.Inaquantitativestudy, Johannsenetal.22demonstratedthattheareaofthedenser MMPRfiberinsertionwasonaverage30.4mm2,corresponding
to a6-mm diametertunnel toreproduceits native attach-mentarea.WhenSWFswereincludedinthemeasurement, theinsertionareaincreasedto77.7mm2.Inthesamestudy,
the authors determined the distances from the center of theMMPRtothemainarthroscopicframes.TheMMPRwas located9.6mmposteriorand 0.7mmlateral totheapexof themedialtibialeminence(themostreproduciblelandmark); 3.5mm lateral to the inflection point of the medial tibial plateauarticularcartilage;and 8.2mmanteriortothemost superiortibialattachmentoftheposteriorcruciateligament (PCL;Fig.1).
Lateralmeniscusposteriorroot(LMPR)
TheattachmentareaofthemainfibersoftheLMPRmeasures 39.2mm2,correspondingtoa7-mmdiametertunnelto
repro-duceitsoriginalattachmentarea.22Thisareadoesnotinclude theadditionalfibers,whichextendtothelateraledgeofthe medialtibialeminence.SomeauthorshavereportedanLMPR areaof115mm2.25Thisdiscrepancyinmeasurementmaybe relatedtotheinclusionoftheadditionalfibersaspartofthe root.Johannsenetal.22demonstratedthatthecenterofLMPR islocated4.2mmmedialand1.5mmposteriortothelateral tibialeminence;4.3mmmedialtoarticularcartilagemargin ofthelateraltibialplateau;12.7mmanteriortothesuperior aspect ofthePCL tibialinsertion; 10.1mmposterior tothe posteromedialcorneroftheanteriorrootattachmentofthe lateralmeniscus;and10.8mmposteriortotheposteromedial ACLband.22
AnimportantconsiderationregardingtheLMPRanatomyis thepresenceofthemeniscofemoralligaments(MFLs),which attach the LMPR to the medial femoral condyle.26 These ligaments play an important role in stabilizing the lateral meniscus and preventingorreducing extrusionin casesof injurytothisroot.26
Biomechanics
Anterior
A
B
ACL
MTE apex
LTE apex
Medial meniscus Medial inflexion point
MMPR ACL LMPR
Lateral meniscus Border of the lateral
cartilage
SWF
PCL
9.6mm
MMPR
SWF PCL Lateralmeniscus
Posterior
Medial meniscus
LMPR 4.2mm
8.2 mm
1.5mm 0.7mm
10.1mm
Fig.1–Superior(A)andposterior(B)viewsoftheposteriormeniscalroots,evidencingtheirinsertionsandanatomical relationships.
LTE,lateraltibialeminence;MTE,medialtibialeminence;SWF,shinywhitefiberslocatedintheposteriorhornofthe medialmeniscus;ACL,anteriorcruciateligamentinsertion;PCL,posteriorcruciateligamentinsertion;LMPR,lateral meniscusposteriorrootinsertion;MMPR,medialmeniscusposteriorrootinsertion.Reprintedwiththepermissionof Johannsenetal.22
distributiontothejoint,increasingthecontactsurfaceand reducing the peak pressure in the compartment.1 This is possiblebecause themeniscusrootsactasanchorsforthe meniscalhorns,allowingthemtoresistthetendencytoward extrusiongeneratedbytheaxialforce.1,5
Damagetothiscomplexmaycompromiseitsfunction.1–6 Biomechanically,ithasbeenshownthatMMPRlesionsreduce thecontactsurfaceand increasesthepeak pressureofthe ipsilateralkneecompartment,duetolossofcircumferential (hoop)stresscausedbythetearofthefibers.The biomechan-icaleffectofthisinjuryissimilartothatofakneeundergoing totalmeniscectomy.1 Therefore,the integrityofthe menis-calrootsisofparamountimportancetopreservethe knee kinematicsofthejointandpreventdegenerativechanges.1,7–9 Themenisci alsoplayaroleinknee stability, especially inthecontextofaligamenttear,wheretheyhaveincreased importanceasasecondaryrestraint.27Allaireetal.1 demon-strated that MMPR injury resulted in increased external rotationandlateraltranslationofthetibia.LMPRinjurieshave lessrepercussiononjointstability,possiblybecausethelateral meniscushastwicethemobilityofthemedialmeniscus.2,5,25 Theposteriorhornsofbothmenisciaremoresusceptible toinjurythantheanteriorhorns.Thiscanbeexplainedbythe factthattheybearmoreloadandarelessmobilethantheir anteriorcounterparts.4,28Thesamereasonsexplainwhythe MMPRismoresusceptibletodamagewhencomparedwith theLMPR.2,5,25,28
Lesions of the meniscal roots correlate with menis-cal extrusion, defined as a displacement of the meniscus beyond the margin of the tibial plateau.29 Hein et al.13 demonstrated that MMPR lesions lead to medial meniscal displacement and the formation of a gap at the insertion
site, whichbecomessignificantlyhigher whencompressive loadsareappliedtotheknee.Thisimpairsthetransmission ofcircumferential(hoop)stress,leadingtofunctionalshock absorption failure and, consequently, to accelerated joint wear.13,25,29
Inabiomechanicalstudy,Ellmanetal.21definedthe struc-turalpropertiesofmeniscalroots,comparingintactrootswith rootsdissectedfromtheiradditionalfibers.Theyconcluded that, exceptforthelateral meniscusanteriorroot,the sup-plementaryfibersoftheanteriormedialmeniscusroot,the MMPR,andtheLMPRareresponsibleforasignificantincrease inthemeanmaximumtensilestrengthresistedbyitsroots. Theseauthorssuggestedthatcurrentfixationtechniquesare notcapableofbiomechanicallyreproducetheadditionalfibers ofnativemeniscalroots.Intheirstudy,themaximumforce resistedbytheposteriormeniscalrootswas513.8N(MMPR) and509N(LMPR).25
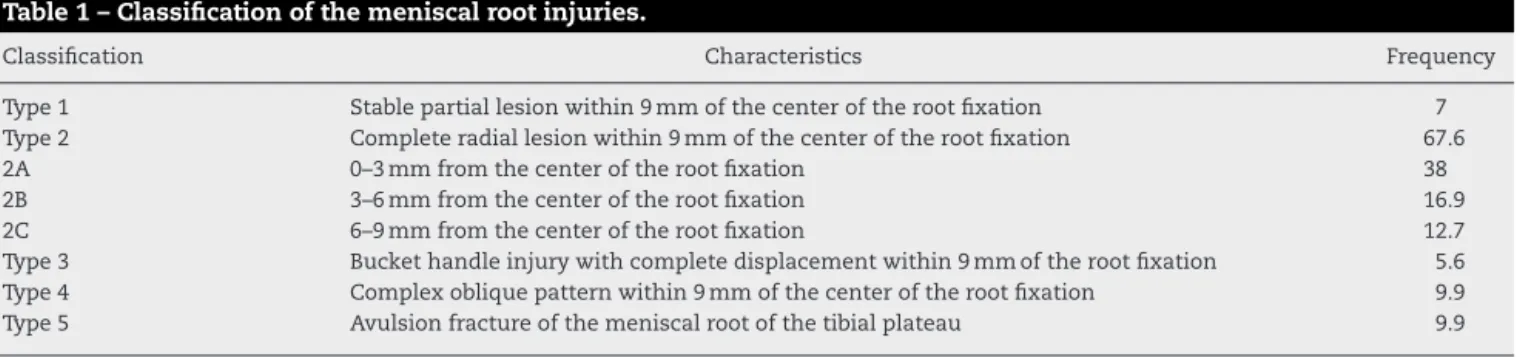
Table1–Classificationofthemeniscalrootinjuries.
Classification Characteristics Frequency
Type1 Stablepartiallesionwithin9mmofthecenteroftherootfixation 7 Type2 Completeradiallesionwithin9mmofthecenteroftherootfixation 67.6 2A 0–3mmfromthecenteroftherootfixation 38 2B 3–6mmfromthecenteroftherootfixation 16.9 2C 6–9mmfromthecenteroftherootfixation 12.7 Type3 Buckethandleinjurywithcompletedisplacementwithin9mmoftherootfixation 5.6 Type4 Complexobliquepatternwithin9mmofthecenteroftherootfixation 9.9 Type5 Avulsionfractureofthemeniscalrootofthetibialplateau 9.9
increaseat90◦ offlexion (126%)and thelowestincreaseat
totalextension(79%).34
On the lateral side, Schillhammer et al.6 assessed the contactareasandpeakcontactpressureinthetibiofemoral compartmentduringsimulatedgaitcyclesaftertheposterior hornofthelateral meniscuswassectioned.They observed thatthisdamagegeneratesasignificantincreaseinpeak pres-sureinthelateralcompartment,from2.8MPato4.2MPa(50%), aswellasasignificantdecrease(32.6%)ofthemaximum con-tactarea(from451mm2intheintactstateto304mm2after
theposteriorhorn ofthe lateralmeniscus wassectioned).6 LaPradeetal.5reportedtheirfindingsforfivetestedflexion angles(0◦,30◦,45◦,60◦,and90◦)andfoundthatanLMPR avul-siondecreasedcontactareaby34% onaverage;the largest reporteddecreasewasat90◦(40%)andthelowestreduction reportedwasintotalextension(23%).Rootavulsionwas asso-ciatedwithameanincreaseincontactpressureof56%,with thehighestincreaseat90◦ (83%)andthelowestincreaseat totalextension(29%).5
TheLMPR hasabiomechanicalparticularity: the conse-quencesofthelesionofthisrootcanvaryaccordingtothe stateofthe MFLs,sincetheyplayanimportantroleinthe transmissionofloadinthelateraltibiofemoralcompartment andinmeniscalextrusionprevention.32 Forkeletal.,33 ina porcinemodelstudy,concludedthatasignificantincreasein thelateraltibiofemoralcontactpressureisonlyexpectedin combinedLMPRandMFLslesions.Brodyetal.,26inastudy usingmagneticresonanceimaging(MRI),reporteda preva-lence of 14% lateral meniscus extrusion in casesof LMPR injurywithintactMFLs,andof60%inthecaseofcombined injuries.
Classification
LaPradeetal.developedaclassificationsystem20thatcanbe usedforbothlesionsoftheposteriorroots(Table1),which facilitatesthedocumentationofresultsandpatientoutcomes. Thissystemcanalsobeusedtoestablishamoreappropriate prognosisandtherapeuticapproach.Fig.2showsthe classi-ficationsystemforlesionsofposteriormeniscalroots.Itis interestingtonotethat,inthatstudy,theauthorsreporteda variantinwhichtheMFLsremainedintactdespiterootinjury, possiblyaddingacertaindegreeofstabilityandpreventing excessiveextrusionofthelateralmeniscus.Allcasesinwhich
thisvariantwasobservedwerereportedintype2(complete) lesions.20
Epidemiology
and
risk
factors
Knowledgeoftheepidemiologicalcharacteristics,suchasthe chronologyoflesionsorassociatedpathologies,mayhelpin thediagnosisofameniscalrootlesion.Allfourmeniscalroots aresubjecttolesions,buttheposteriorrootsaremost com-monlyaffected.4,18,28
MMPRlesionsarethemostfrequent,withaprevalenceof 10–21%amongallmeniscalsurgeries.28Thepercentageofall medialmeniscuslesionsthatarelocatedintheposteriorroot canreach 21.5%.19 Theyare morecommonlyobservedina chronic setting,usuallyinmiddle-agedwomen, withmore subtle symptoms, degenerative pattern, and often without a definite history of trauma.19,35 As observed in the acute setting, MMPR tears are usually related to multi-ligament lesions andcartilage damageclassifiedas Outerbridge2or higher.18OtherfactorsrelatedtoMMPRinjuriesincludebody massindex(BMI), mechanicalaxisinvarus,and lowlevels ofphysicalactivity.19Anincreasedriskofspontaneousknee osteonecrosiswasalsodescribedincombinationwithMMPR lesions.36
LMPRlesionsaremorecommonlyobservedinacute con-ditions,inassociationwithACLlesions,especiallyinyoung malepatients.32,37 Upto8%ofACLinjurieshavean associ-atedLMPRtear,whileinjuryoccursonlyin0.8%ofpatients withintactACL.38
In aretrospectivestudy,Mello et al.39 analyzedthe epi-demiologyofmeniscallesionsassociatedwithACLtear.The authorsconcludedthatlateralmeniscalinjurywasmore fre-quentinthe firstfour monthsafterACL tear,andthat the laterthereconstructionsurgery,thegreatertheincidenceof meniscalinjury,especiallythoseinthemedialmeniscus.
Anterior rootlesions may alsooccur ina traumatic sit-uation, but most studies describe them as a result of an iatrogenicinjury,duringtheperforationofatunnelforACL reconstruction orfortheintroduction ofanintramedullary tibialnail.28,40
Type 1
Type 4
Type 5
Type 2
Type 3
FC
FC FC
FC FC
Partial
root lesion Complete
root lesion
Oblique root lesion
Bucket-handle injury
Avulsion fracture
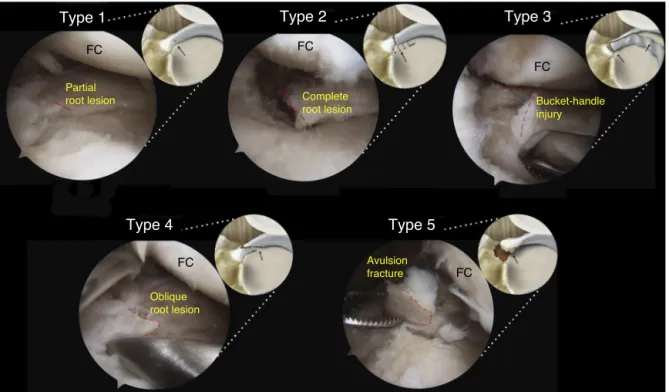
Fig.2–Arthroscopicsimulationandillustrationofthedifferenttypesofmeniscalrootlesionsclassifiedbasedon
morphology:stablepartialrootlesion(type1);completeradiallesionwithin9mmfromtheposteriorfixationintheplateau (type2);bucket-handleinjurywithcompleterootdetachment(type3);longitudinalorcomplexobliquelesionwithtotalroot detachment(type4);andavulsionfractureofthemeniscalroot(type5).
FC,femoralcondyle.
Originalphotographandpartialreproductionofimage,withthepermissionofLaPradeetal.20
BehavioralcharacteristicsrelatedtoEasterncultures,such askneelingandsquatting,mayalsobeassociatedwith pos-teriorrootlesions41butthisaspectisnotwelldefinedinthe literature.28
Diagnosis
Asthesymptomatologyofmeniscalrootlesionsishighly vari-able,diagnosiscanbechallenging,requiringahighdegreeof suspicionaswellasknowledgeoftheassociatedriskfactors andcommonlyrelatedlesions.
Clinical
evaluation
MMPRinjuriesarenotnecessarilyassociatedwithatraumatic event.Approximately70%ofpatientsreportaroutineevent (suchassquatting),whileothersdonotreportany specific event.25,42Themostcommonsymptomsofposteriormeniscal roottearsareposteriorkneepainandpaininthearticularline, whicharenonspecific.32Mechanicalsymptoms,suchas block-ing,arelesscommon.Jointeffusionisobservedinonly14.3% ofthecases,andMcMurraytestispositiveinonly57.1%of patients.43Seiletal.44describedatesttodetectMMPRlesions basedonmeniscalextrusion.Themaneuverconsistsin apply-ingastressin varus,withthe kneeinfullextension,while
palpatingtheanteromedialjointline.Itisconsideredpositive whenthemeniscusextrusioncanbepalpatedanddisappears whenthekneeisbroughtbackintonormalalignment.
Imaging
Magneticresonanceimagingisthemostindicated noninva-siveexamination.4,25,38Nonetheless,someauthorspostulate thattheonlywaytoconfirmaposteriormeniscalrootinjury isthrougharthroscopy.32 Uptoone-thirdofadjacentradial MMPRlesionscannotbeobservedonMRI.9,25 Theabilityof MRItodetectaposteriormeniscalrootteardependsonthe imagequalityandtheabilityoftheradiologist.25 Generally, T2-weightedsequencesaremoresuitabletoassessmeniscal rootinjury.25However,arecently-releasedprotocolusingfat suppression(FS3DVISTA)hasshownbetterperformancein thediagnosisoftheselesions.28
Normally, posterior meniscal roots can be visualized in twoconsecutivecoronalimagesasafibrocartilagebandthat anchors the posterior horn of the meniscus to the tibial plateau.25Ideally,coronal,sagittal,andaxialimagesshould beassessed.38
Fig.3–T2-weightedmagneticresonanceimagingofaleftkneewithlesionofthemedialmeniscusposteriorroot. Evidencing:(A)sagittalcut,showingtheghostsign(yellowarrow);(B)coronalcut,inwhichitispossibletoobservethe medialmeniscusextrusion(yellowarrow),and(C)axialcutshowinganincreaseinthesignintheposteriorinsertionarea ofthemedialmeniscus,indicatingaradiallesionofthisroot.
Meniscalextrusion, definedasameniscaldislocationin relationtothemarginofthetibialplateau,29hasbeenhighly correlatedwiththepresenceofameniscalrootlesion. Extru-sionslargerthan3mmhavebeenassociatedwithmeniscal andarticularcartilagedegeneration.29,45
Theghostsignisdefinedastheabsenceofanidentifiable meniscusinthesagittalplaneorasahighsignalreplacing thelowsignalofthenormalmeniscus,followed by menis-calimageswithanormalsignalintheimmediatelyadjacent sequences.4,29
Treatment
indications
and
options
Treatmentofposteriormeniscalroottearsrequiresacareful evaluation of each patient. Factors that should be con-sidered when choosing a treatment option include – but are not limited to – the condition of articular cartilage and meniscal tissue, mechanical alignment, BMI, patient expectations,andwillingnesstoadheretotherehabilitation protocol.
Non-surgical treatment may be a reasonable option for older patients,46 those with clinical contraindication to surgery,andthosewithadvancedjointdamageinthe ipsi-lateral compartment(Outerbridge 3or 4).These should be managedwithsymptomaticreliefthrough theuseof anal-gesicsand/orbraces.
Surgicaloptionsincludepartialmeniscectomyand menis-cal root repair. Osteotomies may be indicated alone or in combinationwithanotherprocedureinselectedcases,totreat misalignmentofthemechanicalaxis.31
Priortotheknowledgeofthebiomechanicaland degener-ativeconsequencesforthejointandtheadventofmeniscal preservation techniques, meniscectomy was widely per-formedasatreatmentoptionfortheselesions.1,7 Currently, selectedpatients maybenefitfrom this procedure, suchas
thosewithosteoarthritisrefractorytoconservativetreatment and who persist with complaints of pain and mechanical symptoms.Patientswithpartiallesions(type1)mayachieve goodresultswithpartialmeniscectomy.47
Indicationsformeniscal repairincludepatientswithan acute history whose cartilage has a normal or near nor-malappearance,aswellaspatientswithchronicsymptoms without preexisting significant osteoarthrosis.25,35,42 Con-traindicationsincludediffusechondralinjuriesgrades3and4, uncorrectedmisalignment,rootlesionswithdefinitive menis-caldegeneration,andobesity(BMI>30).25,35,48
Thetechniquesformeniscalrootsrepaircanvaryin rela-tionshiptothesurgicalapproach,typeofsuture,deviceused, andfixationtechnique.
Somesurgeonsprefertoapproachtheselesionsthrough aposteromedialportalandoccasionallyassociatea postero-lateral portal to facilitate sutures.42,48,49 Different ligatures havebeenreportedintheliterature,includingpolydioxanone (PDS)No.1(Ethicon,Somerville,NJ);EthibondNo.2(Ethicon, Somerville,NJ);andFiberWireNo.0andNo.2(Arthrex,Naples, FL).48Moststudiesdescribetheuse oftwospecifictypesof devices: acurved suturehook35,42,43,49 and an arthroscopic suturingforcepsloadedwithaneedletopiercethemeniscal tissueanddeploythesuture.50,51
Suturetechniquesreportedintheliteratureincludesingle suture,doublesuture,simplerunningsuture,lockedrunning suture,modifiedKessler,andmodifiedMason-Allen.52–54
The most commonly reported fixation techniques are transtibial pull-outandanchors.2,5,34,54 Thetranstibial pull-out canbeattachedtotheanteriorsurfaceoftheproximal tibiausingapost-tie(screwandwasher),corticaldevice,or bonebridge(whenusingatwo-tunneltechnique).43,49
Radial lesion 3 mm from the root
Meniscal root remnant tissue
Suture tunnels
Cortical fixation device
Fig.4–Techniqueforfixationoflesionoftheposterior meniscalrootthroughatranstibialsuturefixatedtoa buttonontheanteromedialaspectofthetibia.An anatomicalpositioningofthefixationisnecessaryto restorethecircumferentialhoopstressofthemeniscus. ReprintedwiththepermissionofPadaleckietal.2
intheproximaltibia.Attachmenttotheanteriortibialsurface ismadewithacorticaldevice(Fig.4).
Postoperative
rehabilitation
Therehabilitationprotocolused bytheseniorauthor (RFL) takes into account the anatomy, biomechanics, outcomes, and clinical judgment; it is divided into different phases and its progression isassessed according to the following criteria.
Phase1
Basedonsurgicalrepairandrangeofmotion(ROM).Weight bearingisnotallowedduringthefirstsixweeks,inorderto avoidstressinthemeniscus.Passivemovementis immedi-atelyperformed,limitedto90◦flexionfortwoweeks,followed by complete recovery of passive ROM. The patellofemoral joint,thequadriceps,andthepatellartendonarealso immedi-atelymobilized,topreventscartissueadhesions.Toprogress tophase2,afullROM(whencomparedwiththecontralateral limb)shouldbeachieved,aswellasminimaljointeffusion, andnormalkneetemperature.
Level2
Fromtheseventhweekonwards,pre-gaitactivitiesare initi-ated.Weightbearingof25%oftotalbodyweightisallowed,
andlargerloadsareinitiatedaccordingtopatienttolerance. Thepatientshouldfeelcomfortablewalkingforatleast25min toprogresstophase3.
Phase3
Exercisesbasedonagreaternumberofrepetitionsandshort restperiodsareconductedtopromotemuscularendurance. Exerciseswithbothlegsprogresstosinglelegexercises.Squats areprogressedupto70◦,accordingtotolerance.Atweek12, stationarybike,freestyleswimming,andtreadmillwalkingare allowed.
Phase4
Thequadricepsisstrengthenedtoachieveatleast80%ofthe forceoftheunaffectedlimb.Multiplanarexercisesare initi-atedtoallowneuromuscularcontrol.
Phase5
Thisphasevariesaccordingtopatientdemand.Atweek22, patients are encouraged to return to running, agility, and changeofdirectionactivities.Totalreturntosportsis autho-rizedonacase-by-casestatus,basedonthepatient’sability.55
Assessment
of
outcomes
Thecomparisonofclinicaloutcomes betweenthedifferent techniquesusedtotreatmeniscalrootlesionshasconflicting results,asmostpublications presentsmall samples, differ-entinclusioncriteria,lackofcontrolgroup,andalowlevelof evidence.
Partialmeniscectomy
Widelyusedinthepastastheprimaryformoftreatmentof theselesions,theresultsofmeniscectomyintheliterature are conflicting. Ozkocet al.9 analyzed70 partial meniscec-tomiesinasampleinwhichapproximately80%ofpatients wereagedover50yearsandwereobese.TheLysholmscore56 improved from 53 to 67 points. However, despite patient satisfaction, the control radiographs evidenced arthrosis progression.9
Intheevaluationof46casesofpartialmeniscectomywith aminimumfollow-upoffiveyears,Hanetal.8found radio-graphicsignsofdegenerativealterationsin16patients,and only56%reportedimprovementinpain,despitethefactthat theLysholmscorehadimprovedsignificantly.
Repair
revision was made, complete healing of the lesion was observed.43
Regarding the curerates ofthe pull-out technique,Cho etal.49foundfourcompletelyhealedlesionsandeight par-tiallyhealed injuriesin13 kneessubmittedtoarthroscopic revision.TheLysholmscoreincreasedfrom34.7to75.6,and theHSSscoreimprovedfrom33.5to82.2.49
Chunget al.30 conducteda meta-analysisto assess the clinicaloutcomesofMMPRinjuryrepairandobserveda signif-icantimprovementontheLysholmscale;however,meniscal extrusiondidnotimprove,andosteoarthrosisprogressionwas inevitable.
Inarecentsystematicreview,allsevenstudies–including 172 patients treated with transtibial pull-out – demon-stratedfunctionalimprovementaftertheprocedure.Among thosewhounderwentanarthroscopicreview,48%presented complete healing, 42% partial healing, and 10% treatment failure.Radiologicalaggravationofatleastonestageinthe Kellgren–Lawrenceclassificationwasobservedin16%ofthe 76patientsevaluatedforosteoarthrosisprogression.48
When comparing the fixation ofmeniscal rootthrough anchorsvs.thepull-outtechnique,Kimetal.42foundno sig-nificantdifferencesintheIKDC,57,58Lysholm,andHSSscores, aswellasinthedegreeofarticulardegenerationbetweenthe twogroups.
Comparisonbetweenpartialmeniscectomyandrepair techniques
ThehighestLysholmandIKDCscoresandlowerratesof pro-gressionofdegenerativechangeswereobservedinpatients withMMPRlesionstreatedwithtranstibialpull-outtypewhen comparedwiththosewhounderwentpartialmeniscectomy.35 Similar resultswere demonstrated byChunget al.31: of20 patientswhounderwentmeniscectomy,sevenrequiredtotal kneearthroplasty,whichwasnotrequiredinthe37patients treatedwithrootfixation.
Final
considerations
Studiessuggestthatpatientsundergoingposteriormeniscal rootrepair,whetherusinganchorsorthetranstibialpull-out technique,presentfunctionalandclinicalbenefitswhen com-paredwith those who underwent meniscectomy. However, morestudieswithahighlevelofevidenceareneededto estab-lishtherelationshipbetweentheuseofthesetechniquesand therateofprogressiontoosteoarthritisinthelongterm.
Conflicts
of
interest
Dr.Robert F. LaPrade isa technicalconsultant forArthrex, Össur,andSmith & Nephew.Theother authors declareno conflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.AllaireR,MuriukiM,GilbertsonL,HarnerCD.
Biomechanicalconsequencesofatearoftheposterior
rootofthemedialmeniscus.Similartototal
meniscectomy.JBoneJtSurgAm.2008;90(9):1922–31.
2.PadaleckiJR,JanssonKS,SmithSD,DornanGJ,PierceCM, WijdicksCA,etal.Biomechanicalconsequencesofa completeradialtearadjacenttothemedialmeniscus posteriorrootattachmentsite:insitupull-outrepair restoresderangementofjointmechanics.AmJSports Med.2014;42(3):699–707.
3.MarzoJM,Gurske-DePerioJ.Effectsofmedialmeniscus posteriorhornavulsionandrepairontibiofemoral contactareaandpeakcontactpressurewithclinical implications.AmJSportsMed.2009;37(1):124–9.
4.PapaliaR,VastaS,FranceschiF,D’AdamioS,MaffulliN, DenaroV.Meniscalroottears:frombasicscienceto ultimatesurgery.BrMedBull.2013;106:91–115.
5.LaPradeCM,JanssonKS,DornanG,SmithSD,Wijdicks CA,LaPradeRF.Alteredtibiofemoralcontactmechanics duetolateralmeniscusposteriorhornrootavulsionsand radialtearscanberestoredwithinsitupull-outsuture repairs.JBoneJtSurgAm.2014;96(6):471–9.
6.SchillhammerCK,WernerFW,ScuderiMG,CannizzaroJP. Repairoflateralmeniscusposteriorhorndetachment lesions:abiomechanicalevaluation.AmJSportsMed. 2012;40(11):2604–9.
7.McDermottID,AmisAA.Theconsequencesof meniscectomy.JBoneJtSurgBr.2006;88(12):1549–56.
8.HanSB,ShettyGM,LeeDH,ChaeDJ,SeoSS,WangKH, etal.Unfavorableresultsofpartialmeniscectomyfor completeposteriormedialmeniscusroottearwithearly osteoarthritis:a5-to8-yearfollow-upstudy.Arthroscopy. 2010;26(10):1326–32.
9.OzkocG,CirciE,GoncU,IrgitK,PourbagherA,Tandogan RN.Radialtearsintherootoftheposteriorhornofthe medialmeniscus.KneeSurgSportsTraumatolArthrosc. 2008;16(9):849–54.
10.PagnaniMJ,CooperDE,WarrenRF.Extrusionofthe medialmeniscus.Arthroscopy.1991;7(3):297–300.
11.HedeA,LarsenE,SandbergH.Thelongtermoutcomeof opentotalandpartialmeniscectomyrelatedtothe quantityandsiteofthemeniscusremoved.IntOrthop. 1992;16(2):122–5.
12.SeedhomBB,DowsonD,ProceedingsWrightV.Functions ofthemenisci.Apreliminarystudy.AnnRheumDis. 1974;33(1):111.
13.HeinCN,DeperioJG,EhrensbergerMT,MarzoJM.Effects ofmedialmeniscalposteriorhornavulsionandrepairon meniscaldisplacement.Knee.2011;18(3):189–92.
14.ZimnyML,AlbrightDJ,DabeziesE.Mechanoreceptorsin thehumanmedialmeniscus.ActaAnat.
1988;133(1):35–40.
15.MarkolfKL,MenschJS,AmstutzHC.Stiffnessandlaxity oftheknee–thecontributionsofthesupporting structures.Aquantitativeinvitrostudy.JBoneJtSurg Am.1976;58(5):583–94.
16.MacCM.Themovementsofbonesandjoints;the synovialfluidanditsassistants.JBoneJtSurgBr. 1950;32-b(2):244–52.
17.RenstromP,JohnsonRJ.Anatomyandbiomechanicsof themenisci.ClinSportsMed.1990;9(3):523–38.
18.MathenyLM,OckulyAC,SteadmanJR,LaPradeRF. Posteriormeniscusroottears:associatedpathologiesto assistasdiagnostictools.KneeSurgSportsTraumatol Arthrosc.2015;23(10):3127–31.
19.HwangBY,KimSJ,LeeSW,LeeHE,LeeCK,HunterDJ, etal.Riskfactorsformedialmeniscusposteriorroottear. AmJSportsMed.2012;40(7):1606–10.
basedontearmorphology.AmJSportsMed. 2015;43(2):363–9.
21.EllmanMB,LaPradeCM,SmithSD,RasmussenMT, EngebretsenL,WijdicksCA,etal.Structuralpropertiesof themeniscalroots.AmJSportsMed.2014;42(8):1881–7.
22.JohannsenAM,CivitareseDM,PadaleckiJR,Goldsmith MT,WijdicksCA,LaPradeRF.Qualitativeandquantitative anatomicanalysisoftheposteriorrootattachmentsof themedialandlateralmenisci.AmJSportsMed. 2012;40(10):2342–7.
23.MessnerK,GaoJ.Themenisciofthekneejoint. Anatomicalandfunctionalcharacteristics,anda rationaleforclinicaltreatment.JAnat.1998;193Pt 2:161–78.
24.AndersonCJ,ZieglerCG,WijdicksCA,EngebretsenL, LaPradeRF.Arthroscopicallypertinentanatomyofthe anterolateralandposteromedialbundlesoftheposterior cruciateligament.JBoneJtSurgAm.2012;94(21): 1936–45.
25.BhatiaS,LaPradeCM,EllmanMB,LaPradeRF.Meniscal roottears:significance,diagnosis,andtreatment.AmJ SportsMed.2014;42(12):3016–30.
26.BrodyJM,LinHM,HulstynMJ,TungGA.Lateralmeniscus roottearandmeniscusextrusionwithanteriorcruciate ligamenttear.Radiology.2006;239(3):805–10.
27.ShybutTB,VegaCE,HaddadJ,AlexanderJW,GoldJE, NoblePC,etal.Effectoflateralmeniscalroottearonthe stabilityoftheanteriorcruciateligament-deficientknee. AmJSportsMed.2015;43(4):905–11.
28.BonasiaDE,PellegrinoP,D’AmelioA,CottinoU,RossiR. Meniscalroottearrepair:why,whenandhow?Orthop Rev.2015;7(2):5792.
29.LererDB,UmansHR,HuMX,JonesMH.Theroleof meniscalrootpathologyandradialmeniscaltearin medialmeniscalextrusion.SkeletRadiol.
2004;33(10):569–74.
30.ChungKS,HaJK,RaHJ,KimJG.Ameta-analysisof clinicalandradiographicoutcomesofposteriorhorn medialmeniscusrootrepairs.KneeSurgSports TraumatolArthrosc.2016;24(5):1455–68.
31.ChungKS,HaJK,YeomCH,RaHJ,JangHS,ChoiSH,etal. Comparisonofclinicalandradiologicresultsbetween partialmeniscectomyandrefixationofmedialmeniscus posteriorroottears:aminimum5-yearfollow-up. Arthroscopy.2015;31(10):1941–50.
32.FeuchtMJ,SalzmannGM,BodeG,PestkaJM,KuhleJ, SudkampNP,etal.Posteriorroottearsofthelateral meniscus.KneeSurgSportsTraumatolArthrosc. 2015;23(1):119–25.
33.ForkelP,HerbortM,SchulzeM,RosenbaumD,KirsteinL, RaschkeM,etal.Biomechanicalconsequencesofa posteriorroottearofthelateralmeniscus:stabilizing effectofthemeniscofemoralligament.ArchOrthop TraumaSurg.2013;133(5):621–6.
34.LaPradeCM,FoadA,SmithSD,TurnbullTL,DornanGJ, EngebretsenL,etal.Biomechanicalconsequencesofa nonanatomicposteriormedialmeniscalrootrepair.AmJ SportsMed.2015;43(4):912–20.
35.KimSB,HaJK,LeeSW,KimDW,ShimJC,KimJG,etal. Medialmeniscusroottearrefixation:comparisonof clinical,radiologic,andarthroscopicfindingswithmedial meniscectomy.Arthroscopy.2011;27(3):346–54.
36.RobertsonDD,ArmfieldDR,TowersJD,IrrgangJJ,Maloney WJ,HarnerCD.Meniscalrootinjuryandspontaneous osteonecrosisoftheknee:anobservation.JBoneJtSurg Br.2009;91(2):190–5.
37.AndersonL,WattsM,ShapterO,LoganM,RiseburyM, DuffyD,etal.Repairofradialtearsandposteriorhorn
detachmentsofthelateralmeniscus:minimum2-year follow-up.Arthroscopy.2010;26(12):1625–32.
38.DeSmetAA,BlankenbakerDG,KijowskiR,GrafBK, ShinkiK.MRdiagnosisofposteriorroottearsofthe lateralmeniscususingarthroscopyasthereference standard.AmJRoentgenol.2009;192(2):480–6.
39.MelloWAJ,PenteadoPCF,MarchettoA,FatarelliIFC, RodriguesRL,CerqueiraPH.Históriadaslesõesmeniscais nareconstruc¸ãodoligamentocruzadoanterior.RevBras Ortop.1999;34(11):569–74.
40.EllmanMB,JamesEW,LaPradeCM,LaPradeRF.Anterior meniscusrootavulsionfollowingintramedullarynailing foratibialshaftfracture.KneeSurgSportsTraumatol Arthrosc.2015;23(4):1188–91.
41.BinSI,KimJM,ShinSJ.Radialtearsoftheposteriorhorn ofthemedialmeniscus.Arthroscopy.2004;20(4):373–8.
42.KimJH,ChungJH,LeeDH,LeeYS,KimJR,RyuKJ. Arthroscopicsutureanchorrepairversuspulloutsuture repairinposteriorroottearofthemedialmeniscus:a prospectivecomparisonstudy.Arthroscopy.
2011;27(12):1644–53.
43.LeeJH,LimYJ,KimKB,KimKH,SongJH.Arthroscopic pulloutsuturerepairofposteriorroottearofthemedial meniscus:radiographicandclinicalresultswitha2-year follow-up.Arthroscopy.2009;25(9):951–8.
44.SeilR,DuckK,PapeD.Aclinicalsigntodetectroot avulsionsoftheposteriorhornofthemedialmeniscus. KneeSurgSportsTraumatolArthrosc.2011;19(12): 2072–5.
45.CostaCR,MorrisonWB,CarrinoJA.Medialmeniscus extrusiononkneeMRI:isextentassociatedwithseverity ofdegenerationortypeoftear?AmJRoentgenol. 2004;183(1):17–23.
46.CamanhoGL.Doragudanojoelhodopacienteidoso.Rev BrasOrtop.2008;43(9):361–6.
47.MordecaiSC,Al-HadithyN,WareHE,GupteCM. Treatmentofmeniscaltears:anevidencebased approach.WorldJOrthop.2014;5(3):233–41.
48.FeuchtMJ,KuhleJ,BodeG,MehlJ,SchmalH,Sudkamp NP,etal.Arthroscopictranstibialpulloutrepairfor posteriormedialmeniscusroottears:asystematicreview ofclinical,radiographic,andsecond-lookarthroscopic results.Arthroscopy.2015;31(9):1808–16.
49.ChoJH,SongJG.Second-lookarthroscopicassessment andclinicalresultsofmodifiedpull-outsuturefor posteriorroottearofthemedialmeniscus.KneeSurg RelatRes.2014;26(2):106–13.
50.AnzAW,BranchEA,SalimanJD.Biomechanical
comparisonofarthroscopicrepairconstructsformeniscal roottears.AmJSportsMed.2014;42(11):2699–706.
51.BlackmanAJ,StuartMJ,LevyBA,McCarthyMA,KrychAJ. Arthroscopicmeniscalrootrepairusingaceterix novostitchsuturepasser.ArthroscTech.2014;3(5):e643–6.
52.MitchellR,PittsR,KimYM,MatavaMJ.Medialmeniscal rootavulsion:abiomechanicalcomparisonof4different repairconstructs.Arthroscopy.2016;32(1):111–9.
53.KopfS,ColvinAC,MuriukiM,ZhangX,HarnerCD. Meniscalrootsuturingtechniques:implicationsforroot fixation.AmJSportsMed.2011;39(10):2141–6.
54.FeuchtMJ,GrandeE,BrunhuberJ,BurgkartR,ImhoffAB, BraunS.Biomechanicalevaluationofdifferentsuture techniquesforarthroscopictranstibialpull-outrepairof posteriormedialmeniscusroottears.AmJSportsMed. 2013;41(12):2784–90.
55.MuellerBT,MoultonSG,O’BrienL,LaPradeRF.
Rehabilitationfollowingmeniscalrootrepair:aclinical commentary.JOrthopSportsPhysTher.
56.PeccinMS,CiconelliR,CohenM.Questionárioespecífico parasintomasdojoelhoLysholmKneeScoringScale– Traduc¸ãoevalidac¸ãoparaalínguaportuguesa.Acta OrtopBras.2006;14(5):268–72.
57.MetsavahtL,LeporaceG,RibertoM,SpositoMM,Del CastilloLN,OliveiraLP,etal.Translationand cross-culturaladaptationofthelowerextremity functionalscaleintoaBrazilianPortugueseversionand
validationonpatientswithkneeinjuries.JOrthopSports PhysTher.2012;42(11):932–9.