www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
REVIEW
ARTICLE
Prevalence
of
Y-chromosome
sequences
and
gonadoblastoma
in
Turner
syndrome
Alessandra
Bernadete
Trovó
de
Marqui
∗,
Roseane
Lopes
da
Silva-Grecco,
Marly
Aparecida
Spadotto
Balarin
UniversidadeFederaldoTriânguloMineiro(UFTM),Uberaba,MG,Brazil
Received5March2015;accepted4June2015 Availableonline25December2015
KEYWORDS Turnersyndrome; Ychromosome; Gonadoblastoma; Prevalence; Polymerasechain reaction;
Gonadaldysgenesis
Abstract
Objective: To assess the prevalence of Y-chromosome sequences and gonadoblastoma in patientswithTurnersyndrome(TS)usingmoleculartechniques.
Datasource: A literature search was performed inPubmed, limiting theperiod oftime to the years2005---2014 andusing the descriptors:TS and Y sequences (n=26), andTS and Y-chromosomematerial(n=27).Theinclusioncriteriawere:articlesdirectlyrelatedtothesubject andpublishedinEnglishorPortuguese.Articleswhichdidnotmeetthesecriteriaandreview articleswereexcluded.Afterapplyingthesecriteria,14paperswereleft.
Datasynthesis: ThemainresultsregardingtheprevalenceofY-chromosomesequencesinTS were:(1)about60%ofthestudieswereconductedbyBrazilianresearchers;(2)theprevalence variedfrom4.6to60%;(3)themostfrequentlyinvestigatedgeneswereSRY,DYZ3andTSPY; (4)seven studiesusedonlypolymerase chainreaction, whileinthe remainingseven itwas associatedwithFISH.Nineofthe14studiesreportedgonadectomyandgonadoblastoma.The highestprevalenceofgonadoblastoma(33%)wasfoundintwostudies.Infiveoutofthenine papersevaluatedtheprevalenceofgonadoblastomawas10---25%;intwoofthemitwaszero.
Conclusions: Accordingtothesedata,molecularanalysistodetectY-chromosomesequences inTSpatientsisindicated,regardlessoftheirkaryotype.Inpatientswhotestpositiveforthese sequences,gonadoblastomaneedstobeinvestigated.
©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(https://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](A.B.T.Marqui).
http://dx.doi.org/10.1016/j.rppede.2015.12.004
PALAVRAS-CHAVE SíndromedeTurner; CromossomoY; Gonadoblastoma; Prevalência;
Reac¸ãoemcadeiada polimerase;
Disgenesiagonadal
PrevalênciadesequênciasdoYedegonadoblastomaemsíndromedeTurner
Resumo
Objetivo: ApresentaraprevalênciadesequênciasdocromossomoYportécnicasmoleculares edegonadoblastomaempacientescomsíndromedeTurner.
Fontesdedados: FoifeitaumapesquisabibliográficanoPubmed,comlimitedeperíodoentre 2005e2014,comosdescritoresTurnersyndromeandYsequences(n=26)eTurnersyndrome
andYchromosomematerial(n=27).Oscritériosdeinclusãoforamartigosquetivessemrelac¸ão diretacomotemaepublicadosnoidiomainglêsouportuguês.Foramexcluídosaquelesque nãocumpriramessescritérioseeramdotiporevisão.Apósaplicac¸ãodessescritérios,14foram selecionados.
Síntesedosdados: Osprincipaisresultadosquantoàprevalênciadesequênciasdocromossomo YemsíndromedeTurnerforam:1---cercade60%dosestudosforamfeitosporpesquisadores brasileiros;2---afrequênciavarioude4,6a60%;3---osgenesSRY,DYZ3eTSPYforamosmais investigados;4---atécnicadePCRfoiempregadaexclusivamenteemseteestudosenossete restantes,associadaàFISH.Novedos14 estudosapresentaraminformac¸õessobre gonadecto-miaegonadoblastoma.Doisestudosrelataramamaiorprevalênciaparagonadoblastoma(33%). Cincodosnoveestudosreferiramprevalênciade10a25%eemdoisessevalorfoinulo.
Conclusões: De acordo com os dados apresentados, é indicada a pesquisa molecular para sequênciasdocromossomoYempacientescomST,independentementedocariótipo.Naquelas compositividadeparaessassequências,énecessáriaainvestigac¸ãodegonadoblastoma. ©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Turner syndrome (TS) is a chromosomal disorder with an incidence of 1:2500 girls; its etiology is associated with totalor partial X-chromosome monosomy andthe diagno-sisismadebykaryotypetesting.1,2Aretrospectivestudyof 260patientswithTSshowedthattheimprovementin chro-mosomal analysis provided a change in the proportionof observedkaryotypetypes.3
PatientswithTSexhibithaveshortstatureandgonadal dysgenesisasmain clinical signs.They alsomay havelow hairlineat thenapeof theneck,strabismus,ptosis, high-arched palate, micrognathia, short and/or webbed neck, lymphedema of hands and/or feet, metacarpal and/or metatarsal shortening, Madelung deformity, cubitus
val-gus,genu valgum,scoliosis and multiple pigmented nevi,
cardiovascularandrenaldisorders,thyroiddisorders, hear-ingimpairment,hypertension,osteoporosis,andobesity.1,2 However, this syndrome is characterized by wide pheno-typicvariability, frompatientswiththe classicphenotype tothosealmostindistinguishablefromthegeneral popula-tion.
Women with TS who have Y chromosome material are at increased risk of developing gonadal tumors, such as gonadoblastoma and dysgerminoma. Gonadoblastoma is a benigngonadaltumorwithahighpotentialformalignancy; it can differentiate into invasive dysgerminomain 60% of casesandalsoinotherformsofmalignanttumors.About90% ofpatientswithgonadoblastomahaveY-chromosome mate-rialintheirgeneticmakeup.Therefore,sequencedetection of Y-chromosome by cytogenetic and/or molecular tech-niques in patients with TS is critical. In positive cases, prophylactic removal of gonads has been indicated.4 Two
recentlypublishedretrospectivestudiesshowedY chromo-somematerialfrequenciesinTSbyclassicalcytogeneticsof 6.6%(4/61)5and7.6%(12/158).6Inonesuchstudy,33%of patients(4/12)hadgonadoblastomaandintwopatientsit progressedtodisgerminonaorteratoma.6Inanotherstudy with 11 patients with sexual differentiation disorders, 7 hadTurnerphenotypeandmosaickaryotypeYinperipheral blood.7 Allpatients withTS underwentgonadectomy, and histopathologicalfindingsrevealedthatfourofthem(57.1%) hadgonadoblastoma,andintwocasesitwasassociatedwith dysgerminoma.7 Regardingtheclassicalcytogenetic analy-sisby GTGbanding,peripheral bloodlymphocytesarethe material of choice because it is easy to harvest this tis-sue,andtheanalysisisusuallyperformedin30metaphases, whichallowsdetectionof10%ofmosaicism.8Theadvantage ofmolecularmethodsisthatitrequirenocellcultureand onlyasmallsamplefor analysisandaremoresensitive to detectlowmosacismo,frequentinTS.8
Thus,theaimofthisreviewistopresenttheprevalence ofY chromosomesequences by moleculartechniques and gonadoblastomainpatientswithTS.
Method
A literature search was performed on Pubmed, on 10/24/2014,withtimelimitbetween2005and2014.Fig.1
showstheflowchartofthiselectronicsearch.
Results
Eletronic search (Pubmed)
Descriptors:
Turner syndrome and Y sequences n=26 (“search 1”)
Descriptors:
Turner syndrome and Y chromosome material n=27 (“search 2”)
Total: 53 articles
7 articles: Searches 1 and 2 5 articles: Search 1 2 articles: Search 2
Articles included from the review n=14
Articles excluded from the review n=39
• Unrelated to the subject • Publication in another language • Review articles
• Directly related to the subject (selection by title and/or abstract analysis)
• Publication in English or Portuguese
Inclusion reasons Exclusion reasons
Figure1 Representationofthemethodandelectronicsearchresults.
studies.Table2showsthekaryotypeofthesepatients.The frequency of gonadoblastomain TS patients withpositive amplificationfor Y-chromosomeis summarized in Table3, withinformationongonadectomyandgonadoblastomainTS
in9of14studies.Theresultsoffivestudies3,14,15,17,21arenot includedinTable3forthefollowingreasons:(1)two stud-ieshadnoinformationongonadectomyandgonadoblastoma in thetext3,21;(2)in twostudies patientswerescheduled
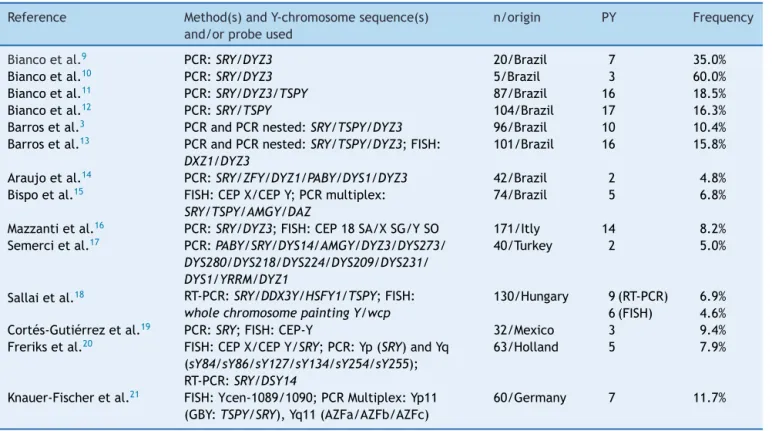
Table1 FrequencyofY-chromosomesequencesidentifiedbymoleculartechniquesinpatientswithTurnersyndrome. Reference Method(s)andY-chromosomesequence(s)
and/orprobeused
n/origin PY Frequency
Biancoetal.9 PCR:SRY/DYZ3 20/Brazil 7 35.0%
Biancoetal.10 PCR:SRY/DYZ3 5/Brazil 3 60.0%
Biancoetal.11 PCR:SRY/DYZ3/TSPY 87/Brazil 16 18.5%
Biancoetal.12 PCR:SRY/TSPY 104/Brazil 17 16.3%
Barrosetal.3 PCRandPCRnested:SRY/TSPY/DYZ3 96/Brazil 10 10.4%
Barrosetal.13 PCRandPCRnested:SRY/TSPY/DYZ3;FISH: DXZ1/DYZ3
101/Brazil 16 15.8%
Araujoetal.14 PCR:SRY/ZFY/DYZ1/PABY/DYS1/DYZ3 42/Brazil 2 4.8%
Bispoetal.15 FISH:CEPX/CEPY;PCRmultiplex: SRY/TSPY/AMGY/DAZ
74/Brazil 5 6.8%
Mazzantietal.16 PCR:SRY/DYZ3;FISH:CEP18SA/XSG/YSO 171/Itly 14 8.2% Semercietal.17 PCR:PABY/SRY/DYS14/AMGY/DYZ3/DYS273/
DYS280/DYS218/DYS224/DYS209/DYS231/ DYS1/YRRM/DYZ1
40/Turkey 2 5.0%
Sallaietal.18 RT-PCR:SRY/DDX3Y/HSFY1/TSPY;FISH: wholechromosomepaintingY/wcp
130/Hungary 9(RT-PCR) 6.9% 6(FISH) 4.6%
Cortés-Gutiérrezetal.19 PCR:SRY;FISH:CEP-Y 32/Mexico 3 9.4%
Freriksetal.20 FISH:CEPX/CEPY/SRY;PCR:Yp(SRY)andYq (sY84/sY86/sY127/sY134/sY254/sY255); RT-PCR:SRY/DSY14
63/Holland 5 7.9%
Knauer-Fischeretal.21 FISH:Ycen-1089/1090;PCRMultiplex:Yp11 (GBY:TSPY/SRY),Yq11(AZFa/AZFb/AZFc)
60/Germany 7 11.7%
Table2 Karyotypesdeterminedbyconventionalcytogenetics(GTG)inpatientswithY-chromosomesequencesidentifiedby moleculartechniques.
Reference Karyotypes Biancoetal.9 45,X:n=7
Biancoetal.10 45,X/46,X,+mar:n=2;45,X/45,X,add(15)(p11):n=1
Biancoetal.11 45,X:n=12;45,X/46,X,+mar:n=2;45,X/45,X,add(15)(p11):n=1;45,X/46,X,r(?):n=1 Biancoetal.12 45,X:n=12;45,X/46,X,+mar:n=2;45,X/45,X,add(15)(p11):n=1;45,X/46,X,r(?):n=1;
45,X/47,XXX:n=1
Barrosetal.3 45,X/46,X,+mar:n=5;45,X:n=3;45,X/46,X,r(?):n=2
Barrosetal.13 45,X:n=3;45,X/46,XY:n=5;45,X/46,X,+mar:n=5;45,X/46,X,r(?):n=2;45,X/47,XYY:n=1 Araujoetal.14 45,X:n=2
Bispoetal.15 45,X/46,XY:n=2;45,X:n=1;45,X/46,XY:n=1;46,X,i(Xq):n=1
Mazzantietal.16 45,X/46,XY:n=6;45,X:n=2;45,X/46,X,idic(Y):n=3;45,X/46,X,+mar:n=2; 45,X/46,XY/46,X,idic(Y):n=1
Semercietal.17 45,X:n=2
Sallaietal.18 45,X:n=3;45,X/46,XY:n=3;45,X/46,X,+mar:n=2;45,X/46,X,del(Xq):n=1 Cortés-Gutiérrezetal.19 45,X/46,X,+mar:n=1;45,X/46,XY:n=1;45,X:n=1
Freriksetal.20 45,X:n=5
Knauer-Fischeretal.21 45,X:n=2;45,X/46,X,idicY(q11.2):n=2;46,X,i(X)(q10):n=1;46,X,del(X)(q12ouq13.1):n=1; 46,X,der(X)t(X;Y)(p22.3;q11.21):n=1
forclinicalfollow-up17ormonitoringbyamultidisciplinary team of biologist, psychologist, geneticist, endocrinolo-gist,and gynecologist14;and (3)inonestudy prophylactic gonadectomywasofferedtoallpatientswithYsequences, however,thesamepatientsoptedforregularmonitoringby ultrasoundandCT.15
Discussion
The present literature review study showed the preva-lenceofY-chromosomesequencesandtheriskofdeveloping gonadoblastomainTSpatients.
Y-chromosomesequences
Of the 14 studies included in this review, 60% were per-formed by Brazilian investigators.3,9---15 Four have been published by the same group and the two studies repor-ting a higher prevalence of Y-chromosome sequences9---12 analyzedsamplesfromdifferenttissues(peripheralblood, oral mucosacells, andhair root).9,10 Onestudy evaluated 20 patients withTS and karyotype 45,X9 and the other 5 patientswithchromosomalabnormalities,suchas chromo-some marker, additional material, or ring chromosome.10 Threestudies9---11 showedthatallinvestigatedpatientshad
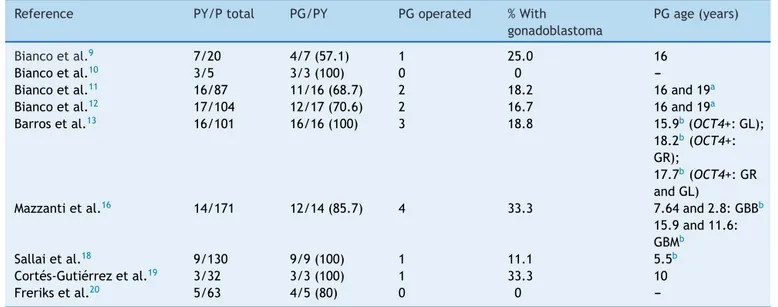
Table3 FrequencyofgonadoblastomainpatientswithTurnersyndromeandY-chromosomesequences. Reference PY/Ptotal PG/PY PGoperated %With
gonadoblastoma
PGage(years)
Biancoetal.9 7/20 4/7(57.1) 1 25.0 16
Biancoetal.10 3/5 3/3(100) 0 0
---Biancoetal.11 16/87 11/16(68.7) 2 18.2 16and19a
Biancoetal.12 17/104 12/17(70.6) 2 16.7 16and19a
Barrosetal.13 16/101 16/16(100) 3 18.8 15.9b(OCT4+:GL);
18.2b(OCT4+: GR);
17.7b(OCT4+:GR andGL)
Mazzantietal.16 14/171 12/14(85.7) 4 33.3 7.64and2.8:GBBb
15.9and11.6: GBMb
Sallaietal.18 9/130 9/9(100) 1 11.1 5.5b
Cortés-Gutiérrezetal.19 3/32 3/3(100) 1 33.3 10
Freriksetal.20 5/63 4/5(80) 0 0
---PY/Ptotal,patientswithYsequenceinrelationtothetotalnumberofpatients;PG/PY,gonadoblastomapatientscomparedtopatients withYsequence;PGoperated,gonadoblastomapatientsundergoingsurgery;OCT4,octamer-bindingtranscriptionfactor4;G,gonad; R,right;E,left;GBB,bilateralgonadoblastoma;GBM,gonadoblastomamonolateral.
amplification for SRY gene and only a few for DYZ3 and
TSPY.ThisdatashowsthattheSRYgeneshouldbeespecially investigatedinpatientswithTS.9---11Inastudypublishedin 2010,Biancoetal.12 alsoevaluatedgeneexpression(SRY,
TSPY,SF1,WT1,DAX1,OCT4,GATA4,FOG2,STRA8)inright
and left gonads of six patients undergoing gonadectomy andfound no differencein theexpression of thesegenes inthistissue bothin patients andcontrols, exceptinone case with high expression of genes SRY, TSPY, and OCT4 inboth gonads [karyotype:45,X/45,X,add(15)(p11)].These nineinvestigatedgenesareinvolvedinsexdetermination, differentiation,andgonadaltumorigenesis.12Inthisstudy,12 allpatientsshowedSRYgeneamplification,whichhighlight the findings previously publicados.9---11 The studies pre-sentedaboveusedexclusivelythepolymerasechainreaction (PCR) technique for the investigation of Y-chromosome sequencesinTS9---12 andreportedfrequencies rangingfrom 16.3to60%.
Two studies performed by another group of investiga-torsalsousedPCRandPCRinit.3,13 Oneofthemassessed Y-chromosome sequences in 96 TS patients a total of 260.3 This research was indicated only in cases of: (a) 45,X karyotype and negative X-chromatin; (b) presence of marker chromosomes in karyotype, i.e., chromosome fragmentsofunknownorigin;and(c)impossibilityof cyto-geneticidentification ofring chromosomeorigin.Thus,96 patients metthese criteria and of these10 showed posi-tiveamplificationfor theinvestigatedgenes. Inthissame study, six cases of intact Y-chromosome had previously been identifiedby classicalcytogenetics (45,X/46,XY: n=5 and45,X/47,XYY:n=1).In asubsequentstudy,thesesame authors evaluated 101 of 260 TS patients by PCR and, whenpositive,theyusedthefluorescenceinsitu hybridiza-tion(FISH)technique.13 The101casesanalyzedbyPCRfor Y-chromosomesequencesshowed45,Xkaryotypeand nega-tiveBarrcorpuscle(n=73),markerchromosome(n=25),and ringchromosome(n=3).
TwootherstudiesreportedthelowerY-chromosome fre-quencyvaluesamongstudiesperformedinBrazil.14,15Infour TSpatients,thedetectionofY-chromosomesequenceswas identifiedonlybyPCR[karyotypes:45,Xand46,X,i(Xq)].14,15 Thus,theinclusionofPCRtechniqueinTSroutine investiga-tionwouldbeindicated.14ItisnoteworthythatsixBrazilian studies have used only the PCR technique for the inves-tigation of Y-chromosome sequences. Advantages of this technique include: (1) quick execution; (2) low cost; (3) simultaneousprocessingofmultiplesamples;(4) applicabil-ityinscreeningofalargenumberofpatients;and(5)high sensitivityfor detectionof mosaicism. The use of PCR to investigate14Y-chromosomesequencesidentifieda preva-lence of 5%,17 value similar to that reported by a study analyzingonlysixsequences.14
FISH and PCR techniques were concurrently used in severalstudies.15,16,18---21Onestudy publishedin2005 iden-tified a frequency of about 6% by classical cytogenetics (10/171)and8%bymolecularanalysis(14/171).16Inanother study,19 GTG banding revealed threepositive cases: kary-otypes45,X/46,X,mar;45,X/46,XY,and45,X. FISHanalysis of lymphocytes revealed: (1) that the marker chromo-some was Y; (2) confirmed the Y-chromosome previously identifiedby classical cytogenetics; and (3) did not iden-tifyY-chromosomematerial, respectively. FISH analysisof
gonadaltissueshowedthatY-chromosomewaspresentin57, 46and26%ofcells,respectively.InvestigationbyPCR/SRY inlymphocytesandgonadswaspositiveinallthreecases. ThecaseconsideredY-negativeinlymphocytesbyGTGand FISH(45,X)waspositiveforSRYbyPCR/lymphocytes. There-fore,theauthorssuggested:(1)theuseofPCR,inaddition toconventional cytogenetic analysis, toruleout the pos-sibility of hidden Y-chromosome mosaicism; and (2) the use of FISHtechnique onlyafter a positiveresultfor PCR becauseitisexpensiveandlaborious.19 InadditiontoFISH, real-timePCR(RT-PCR)wasalsoused.18,20 Thefirststudy18 identified Y-chromosome mosaicism by conventional cyto-genetic analysisin three of the 130 patients investigated (karyotypes:45,X/46,XYn=3).Twopatientshavemosaicism aroundtheY-chromosome,whiletheotherpatienthadonly part ofthe Y-chromosome.By RT-PCR,ninepatients were positive for Y. Of the four Y-chromosome specific probes used in the RT-PCR technique, two (SRY and TSPY1) are onthe Y-chromosomeshortarm (Yp)and two(DDX3Yand
HSFY1) on the long arm (Yq). Six patients had
amplifica-tiontothe foursequences,threetotwo(SRYand TSPY1) orthree(SRY,TSPY1,andDDX3Y)sequences;thatis,three patientshadnocomplicationsof HSFY1geneandonehad
loss of DDX3Y region, which suggests Yq deletion. FISH
analysis confirmed positive for Y in six cases. Thus, the frequency of Y-chromosome sequences was 2.3, 4.6, and 6.9%by GTGbands,RT-PCR,andFISH techniques, respec-tively. In the 2013 study,20 with 162 TS patients, 75 had a 45,Xkaryotype andofthese63 have agreedtoundergo additionalmolecularinvestigations.Ysequenceswere iden-tified by FISH in five patients on oral cell samples but notin peripheralblood lymphocytesby PCR.RT-PCR anal-ysis revealed the presence of SRY and DYS14 in two of them.20 In another study, the combined use of PCR and FISH allowedthe identificationof afrequency of approxi-mately12%ofY-chromosomesequencesinTS.Oftheseven patientswithY-sequences,21fourdidnotshowitinthe kary-otype.
In short, in the present study the frequency of Y-chromosome sequencesin TS patients rangedfrom 4.6to 60%.Accordingtotheliterature,theprevalenceis0---61%.19 This difference may be due to the following factors: selection criteria of patients, sample size, methodology, andY-chromosomemarkersused.Whentheanalyzedtissue wasperipheralbloodalone,theprevalenceofYsequences ranged from4.6 to 18.5%.11,21 However, in studies where more than one tissue evaluated, the prevalence was greater.9,10 SRY, DYZ3, and TSPY genes were the most widely investigated.SRY gene is locatedin the shortarm of Y-chromosome (Yp11.3) and DYZ3 gene in the pericen-tromeric region at Yp12. Both genes play a role in sex determination and chromosomal stability, respectively.22
contradicts those published in the literature that recom-mendtheuseofPCRintheinvestigationofY-chromosome sequencesinTS.The authorsattributethislow sensitivity to the difficulty in detecting mosaicism below 10%.20 Chromosomal mosaicism is defined as the presence of twoor more distinctcell lineswithin thesame individual resultingfrompost-zygoticnondisjunction.Whenitoccurs inalreadydifferentiatedcells,mosaicismmaybeconfined tooneor afew tissues.26 Inthis context,investigationof Y-chromosomesequencesintissuesofdifferentembryonic originsisadvised, suchascells ofthe oralmucosa,which caneasilybeharvestedbynon-invasiveprocedures.
To our knowledge,thereis only one systematicreview focusing on clinical and genetic characteristics of TS, mosaicism,Y-chromosome,andriskofgonadaltumor.8Data presented inthis study show:(1) thatthe detectionof Y-chromosomesequencesinTS,regardlessofthekaryotype, isnecessarytopreventthedevelopmentofgonadoblastoma; and(2)PCRtechniqueshouldbeemployedduetoitshigh sensitivity,lowcost,andeasytoperform.
After TS confirmationby cytogenetics,the inclusionof thePCRtechniqueissuggestedasacomplementfor detec-tion of Y-chromosome sequences in these patients. This moleculartechnique is moresensitive andcan detect the presenceofY-chromosomematerial.
Gonadoblastoma
Gonadoblastoma, oftenobserved in thesecond decade of life, is a benign gonadal tumor with a high potential for malignant transformation.4 It has a good prognosis and maydifferentiate into a germ celltumor, such as dysger-minomas, and less frequently into teratomas, embryonal carcinoma, yolk sac tumor, and choriocarcinoma.13 This tumorispresentmainlyinwomenwithgonadaldysgenesis, andapproximately95%ofthemhaveY-chromosome mate-rial in their genomes. Therefore, the detection of these sequencesbycytogeneticand/ormoleculartechniqueshas been encouraged to guidethe prophylactic indication for surgicalremovalofgonadsinthisgroupofpatients,as gen-erally they are not metastatic tumors, and there is the possibility of cure with their removal.4 Women with TS havegonadaldysgenesisandthereforethedetectionofthe Y-chromosome sequences in these patients is of extreme clinicalimportance.
Thehighestprevalenceforgonadoblastomainthisreview was33%16,19andisinlinewithotherstudies.6,27This percent-agewasidentifiedinarecentsurvey,andfourpatientswith SThadthekaryotype45,X/46,XY.6Twoofthemhada dys-germinoma(ageatsurgery:11.25years)andateratoma(15 years).Inthetwopatientswithgonadoblastomaalone,age atsurgerywas1.5and11.7years.6Anotherstudypublished recently reported 35.3% incidence of gonadoblastoma.28 TwentypatientswithTShadY-chromosomesequencesfrom atotalof217and17ofthemunderwentgonadectomy.28An evenhigherfrequencywasreportedbyAlvarez-Navaetal.29 who investigated 52 patients and detected four with Y-chromosomesequences(7.7%),allunderwentgonadectomy andtwohad gonadoblastoma(50%).Fivestudies reported incidenceof10---25%.9,11---13,18Previousstudieshavereported frequenciesof7---10%30and16.7%.31Thesefindingsshowthat
thefrequencyofgonadoblastomaisvariableandmayreflect anearlyinvestigation.
InstudiesperformedbyBiancoetal.,9---12resultsobtained were: (1) one 45,X patient with bilateral gonadoblas-tomapositiveSRYgeneamplificationfor thethreetissues analyzed9; (2) two patients with bilateral gonadoblas-toma[45,X:SRY+and45,X/46,X,r(?):SRY+DYZ3+]11;(3)two patients with bilateral gonadoblastoma [45,X: SRY+ and 45,X/46,X,r(?):SRY+].12Althoughtherewasnopatient iden-tifiedwithgonadoblastoma,histopathologicalstudyofthe gonadsofonepatientrevealedstromalcellhyperplasiaand luteoma.10 Subsequent studies also showed patients with thesehistopathologicalfindings.11,12
Another geneassociated withgonadoblastoma is OCT4
(octamer-bindingtranscriptionfactor4),12,13 alsoknownas
OCT3 or POU5FI. This gene is considered to be a tumor
marker of germ cells, such as gonadoblastoma, dysger-minoma, seminoma, and others, and its expression was detected by immunohistochemistry in 100% of cases of gonadoblastoma.32 The study published in 2010 showed highexpressionof theSRY,TSPY,andOCT4genes inboth gonadsofapatientwithpositivePCR (SRY+andTSPY+).12 Another study showed that immunohistochemical analy-sisfor OCT4 was positive in three cases (karyotypes: 45, X/46,XY:n=2and45,X/46,X,+mar:n=1),asuggestingresult ofgermcelltumor(gonadoblastomaorcarcinomainsitu).13 Inthisstudy,the16casesofYsequencesunderwent bilat-eral gonadectomy, and the left and right gonads were assessed by conventional staining with hematoxylin and eosin (H&E) and immunohistochemical staining for OCT4. Gonadal neoplasia was not detected in any of 32 gonads evaluated by H&E; however, four gonads (12%) of three patients(19%)werepositiveforOCT4,suggestingthe exis-tenceof germ celltumors.13 Forthis reason,the authors recommend a specific histopathological study in gonads, suchasOCT4immunohistochemistry,toassesstherealrisk of gonadal tumorsin patients withTS and Y-chromosome sequences.12,13
Regardingthestudiesthatreportedahigherprevalence of gonadoblastoma, one of them reported two patients with monolateral gonadoblastoma (karyotype: 45,X and 45,X/46,X,+mar) and two with bilateral gonadoblastoma (karyotype:45,X/46,XY)16andtheotherreportedapatient 45,X/46,XYwithgonadoblastoma.19 Inthestudypublished in 2010, prophylactic surgery was performed in all nine patientswithY-chromosomematerialbeforeageof20and one of them, a girl of 5-year old, the youngest patient in the study, had bilateral gonadoblastoma without clini-calsigns.18Thispatienthada45,X/46,XYkaryotype(GTG), wcpY+93(FISH),andwaspositiveforallY-specificsequences
(SRY,TSPY1, DDX3Y,and HSFY1).Ovarian tissuehistology
revealednogonadoblastomainfourofthepatients under-goinggonadectomy.20
46,X,+der(15)/46,XYand ages:11yearsand6monthsand 15yearsand4months,respectively).Theyoungestpatient withTSsubmittedtogonadectomywas2yearsold.7
According to data presented, it can be concluded thatmolecularinvestigationisindicatedforY-chromosome sequencesin TS patients, regardless of the karyotype, as a complement to the cytogenetic diagnosis. PCR is the technique suggested because it is inexpensive, sensitive, rapid,and enablethe tracking of varioussequencesof Y-chromosomesimultaneously.Itwouldalsobeappropriatefor analysisofasecondtissue,inadditiontoperipheralblood. InthosepatientswithY-positivesequences,gonadoblastoma investigationisrequired.
Funding
Thestudyreceivednofunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Sybert VP, McCauley E. Turner’s syndrome. N Engl J Med. 2004;351:1227---38.
2.SantosV,Marc¸alM,AmaralD,PinaR,LopesL,FonsecaG.Turner syndrome.Fromchildtoadult...Amultidisciplinaryapproach.
ActaMedPort.2010;23:873---82.
3.BarrosBA,Maciel-GuerraAT,DeMelloMP,CoeliFB,CarvalhoAB, Viguetti-CamposN,etal.Ainclusãodenovastécnicasdeanálise citogenética aperfeic¸oou o diagnósticocromossômico da sín-dromedeTurner.ArqBrasEndocrinolMetab.2009;53:1137---42. 4.LipayMV,BiancoB,VerreschiIT.Gonadaldysgenesisandtumors: genetic and clinical features. Arq Bras Endocrinol Metab. 2005;49:60---70.
5.MohamedS,RocheEF,HoeyHM.Modeofinitialpresentationand chromosomalabnormalities inIrishpatientswithTurner syn-drome:asingle-centreexperience.JPediatrEndocrinolMetab. 2014[Epub2014].
6.Kanakatti Shankar R, Inge TH, Gutmark-LittleI, Backeljauw PF. Oophorectomy versus salpingo-oophorectomy in Turner syndromepatientswithY-chromosomematerial:clinical expe-rienceandcurrentpracticepatternsassessment.JPediatrSurg. 2014;49:1585---8.
7.MatsumotoF,ShimadaK,IdaS.Tumorsofbilateralstreakgonads inpatientswithdisordersofsexdevelopmentcontainingy chro-mosomematerial.ClinPediatrEndocrinol.2014;23:93---7. 8.OliveiraRM,VerreschiIT,LipayMV,Ec¸aLP,GuedesAD,Bianco
B.YchromosomeinTurnersyndrome:reviewoftheliterature. SaoPauloMedJ.2009;127:373---8.
9.Bianco B, Lipay MV, MelaragnoMI, Guedes AD,Verreschi IT. DetectionofhiddenYmosaicisminTurner’ssyndrome: impor-tanceinthepreventionofgonadoblastoma.JPediatrEndocrinol Metab.2006;19:1113---7.
10.Bianco B, Lipay MV, Guedes AD, Verreschi IT. Clinical implications of the detection of Y-chromosome mosaicism in Turner’s syndrome: report of 3 cases. Fertil Steril. 2008;90(1197):e17---20.
11.BiancoB,LipayM,GuedesA,OliveiraK,VerreschiIT.SRYgene increasestheriskofdevelopinggonadoblastomaand/or nontu-moralgonadallesionsinTurnersyndrome.IntJGynecolPathol. 2009;28:197---202.
12.BiancoB,OliveiraKC,GuedesAD,BarbosaCP,LipayMV, Ver-reschiIT.OCT4gonadalgeneexpressionrelatedtothepresence ofY-chromosomesequencesinTurnersyndrome.FertilSteril. 2010;94:2347---9.
13.BarrosBA,MoraesSG, CoeliFB,Assumpc¸ãoJG,DeMello MP, Maciel-GuerraAT, etal.OCT4 immunohistochemistrymay be necessarytoidentifytherealriskofgonadaltumorsinpatients with Turner syndrome and Y chromosome sequences. Hum Reprod.2011;26:3450---5.
14.Araujo C, Galera MF, Galera BB, Silvestre FG, Medeiros SF. Molecular identification of chromosome Y sequences in BrazilianpatientswithTurnersyndrome.GynecolEndocrinol. 2008;24:713---7.
15.Bispo AV, Burégio-Frota P, Oliveira dos Santos L, Leal GF, Duarte AR, Araújo J, et al. Y chromosome in Turner syn-drome: detection of hidden mosaicism and the report of a rare X;Y translocation case. Reprod Fertil Dev. 2014;26: 1176---82.
16.MazzantiL, CicognaniA, Baldazzi L,BergamaschiR, Scarano E, Strocchi S, et al. Gonadoblastoma in Turner syndrome and Y-chromosome-derived material. Am J Med Genet A. 2005;135:150---4.
17.SemerciCN, Satiroglu-Tufan NL, Turan S, BereketA, Tuysuz B, Yilmaz E,et al. Detectionof Y chromosomal material in patientswitha45,XkaryotypebyPCRmethod.TohokuJExp Med.2007;211:243---9.
18.SallaiA,SólyomJ,DobosM,SzabóJ,HalászZ,SágodiL,etal. Y-chromosomemarkersinTurner syndrome:screeningof130 patients.JEndocrinolInvest.2010;33:222---7.
19.Cortés-Gutiérrez EI, Herrera-Bartolo R, Dávila-Rodríguez MI, Palacios-Saucedo GC, Vargas-Villarreal J, Romero-Villarreal JB. Molecular detection of cryptic Y-chromosomal mate-rial in patients with Turner syndrome. Oncol Rep. 2012;28: 1205---10.
20.FreriksK,TimmersHJ,Netea-MaierRT,BeerendonkCC,Otten BJ,vanAlfen-vanderVeldenJAEM,etal.BuccalcellFISHand bloodPCR-YdetecthighratesofXchromosomalmosaicismand YchromosomalderivativesinpatientswithTurnersyndrome. EurJMedGenet.2013;56:497---501.
21.Knauer-FischerS,BesikogluB,IntaI,KneppoC,VogtPH, Bet-tendorfM.AnalysesofgonadoblastomaY(GBY)-locusandofY centromereinTurnersyndrome patients.ExpClinEndocrinol Diabetes.2015;123:61---5.
22.Harley VR, Clarkson MJ, Argentaro A. The molecular action and regulationof the testis-determining factors, SRY (sex-determining region on the Y chromosome) and SOX9 [SRY-related high-mobility group (HMG) box 9]. Endocr Rev. 2003;24:466---87.
23.SaloP,KääriäinenH, PetrovicV,PeltomäkiP,PageDC,dela Chapelle A. Molecular mapping of the putative gonadoblas-tomalocusontheYchromosome.GenesChromosomesCancer. 1995;14:210---4.
24.TsuchiyaK,ReijoR,PageDC,DistecheCM.Gonadoblastoma: moleculardefinitionofthesusceptibilityregionontheY chro-mosome.AmJHumGenet.1995;57:1400---7.
25.HildenbrandR,SchröderW,BrudeE,ScheplerA,KönigR,Stutte HJ,etal.DetectionofTSPYproteininaunilateralmicroscopic gonadoblastomaofa Turner mosaicpatientwitha Y-derived markerchromosome.JPathol.1999;189:623---6.
26.Maciel-Guerra AT, Paulo JD, Santos AP, Guaragna-Filho G, AndradeJG,Siviero-MiachonAA,etal.Theuseoffluorescence insituhybridizationinthediagnosisofhiddenmosaicism: apro-pos of three cases of sex chromosome anomalies. Arq Bras EndocrinolMetabol.2012;56:545---51.
28.ZelayaG,LópezMartiJM,MarinoR,GarcíadeDávilaMT,Gallego MS.GonadoblastomainpatientswithUllrich-turnersyndrome. PediatrDevPathol.2014;18:117---21.
29.Alvarez-Nava F, Soto M, Sánchez MA, Fernández E, Lanes R. Molecular analysis in Turner’s syndrome. J Pediatr. 2003;142:336---40.
30.Gravholt CH, Fedder J, Naeraa RW, Müller J. Occurrence of gonadoblastoma in females with Turner syndrome and Y
chromosome material:a population study.J Clin Endocrinol Metab.2000;85:3199---202.