Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Original
article
Carcinoid
tumor
of
cecal
appendix:
one-year
incidence
at
the
Santa
Marcelina
Hospital
夽
Isaac
José
Felippe
Corrêa
Neto
a,b,∗,
Eduardo
Augusto
Lopes
c,
Rafael
Domingues
Marques
c,
Rogério
Freitas
Lino
Souza
a,
Alexander
Sá
Rolim
a,b,
Hugo
Henriques
Watté
a,b,
Laércio
Robles
aaServiceofColoproctology,HospitalSantaMarcelina(HSM),SãoPaulo,SP,Brazil
bSociedadeBrasileiradeColoproctologia(SBCP),SãoPaulo,SP,Brazil
cHospitalSantaMarcelina(HSM),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14March2014 Accepted11August2014 Availableonline23October2014
Keywords:
Acuteappendicitis
Carcinoidtumoroftheappendix Conduct
Follow-up
a
b
s
t
r
a
c
t
Introduction:Carcinoidtumorsareneuroendocrinemalignanciesthatoriginateinthe neu-roectodermalcellsoftheAmine,PeptideUptakeandDecarboxylationsystemdispersedin thegastrointestinalmucosaandrepresentingabout80–88%oftumorsofcecalappendix. Thesearetumorsusuallydiagnosedatappendectomies,anditisestimatedthatfromeach 100appendectomiesyearlyperformed,atleastonecaseisaneuroendocrinetumor.
Objectives: ToreporttheexperienceofanUniversityTeachingHospitalinhealthand refer-enceattheeastsideofSãoPauloandgreatSãoPauloincasesoftheserareappendicular tumors,withemphasisontheimportanceofthesedescriptions,asprobablyarerarethose surgeonsinparticularwhowillacquireextensivewisdominthesecases.
Method:Retrospectiveanalysisof237patientswhounderwentappendectomyfrom Septem-ber2010toSeptember2012intheHospitalSantaMarcelina-SP.Weevaluateddataonage, gender,initialclinicalpresentationandsurgicalfindingsofpatientsundergoing appendec-tomywithsubsequentanatomicandimmunopathologicaldiagnosisofcarcinoidtumorof cecalappendix.
Results:The presenceofa carcinoidtumoroftheappendix wasobservedin5patients, whichcorrespondsto2.1%ofallappendectomiesperformed.Regardinggender,4patients (80%)werefemaleandtheaverageagewas34.2years,witharangefrom17to68years. Inallpatientstheinitialhypothesisforsurgeryindicationwasacuteappendicitis,withan intraoperativefindingofnecroperforatedphaseacuteappendicitisin3patients(60%).
夽
StudyconductedattheColoproctologyMedicalResidencyProgram,DepartmentofGeneralSurgery,HospitalSantaMarcelina,São Paulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](I.J.F.CorrêaNeto).
http://dx.doi.org/10.1016/j.jcol.2014.08.009
Conclusion: The therapeutical conduct after the diagnosis of carcinoid tumors of the appendixmustbebasedonthedataprovidedbypathologicalandimmunohistochemical studies,besidesthejudiciousjudgmentoftheattendingphysician.
©2014SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Tumor
Carcinoide
de
Apêndice
Cecal:
incidência
em
um
ano
no
Hospital
Santa
Marcelina
Palavras-chave:
Apendiciteaguda
Tumorcarcinoidedeapêndice Conduta
Seguimento
r
e
s
u
m
o
Introduc¸ão: Os tumores carcinoides são neoplasias malignas neuroendócrinas que se originamemcélulasneuroectodérmicasdosistemaAPUD(Amine,PeptideUptakeand Decar-boxylation),dispersasnamucosagastrointestinalequerepresentamcercade80-88%das neoplasiasdoapêndicececal.Sãotumoresdiagnosticadosgeralmentedurante apendicec-tomiaseestima-sequedecada100apendicectomiasrealizadasporano,aomenosumcaso seráTNE.
Objetivos: Objetiva-senesseartigorelatarexperiênciadeHospitalUniversitárioedeEnsino (HUE)em saúdeereferêncianazonalestedeSãoPauloe grandeSãoPauloem casos dessesrarostumoresapendiculares,comênfasenaimportânciadessasdescric¸ões,jáque provavelmenteraroscirurgiõesemparticularirãoadquirirumaextensasapiêncianesses casos.
Método:Análiseretrospectivade237pacientessubmetidosàapendicectomianoperíodode setembrode2010asetembrode2012noHospitalSantaMarcelina-SP.Foramavaliadosos dadosreferentesaidade,sexo,quadroclínicoinicial,achadosoperatóriosdospacientes sub-metidosàapendicectomiacomposteriordiagnósticoanatomopatológicoeimunopatológico detumorcarcinoidedeapêndice.
Resultados: Verificou-seapresenc¸adetumorcarcinoidedeapêndiceem5pacientes,oque correspondea2,1%dasapendicectomiasrealizadas.Comrelac¸ãoaogênero,4pacientes (80%)erammulhereseamédiadeidadefoide34,2anos,comvariac¸ãode17a68anos.Em todosospacientesahipóteseinicialparaindicac¸ãodecirurgiaforadeapendiciteaguda, comachadointra-operatóriodeapendiciteagudaemfasenecroperfuradaem3pacientes (60%).
Conclusão: Acondutaapósodiagnósticodetumorescarcinoidesdeapêndicececaldeve seralicerc¸adanosdadosfornecidosporexamesanatomopatológicoseimunoistoquímicos, alémdojulgamentocriteriosodomédicoassistente.
©2014SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Recognizedsincethelatenineteenthcenturyandreceiving thedesignation“karzinoid”onlyin1917byOberndorfer,1,2
car-cinoidtumorsareneuroendocrinemalignanciesthatoriginate inneuroectodermalcellsoftheAPUD(Amine,PeptideUptake andDecarboxylation)system,dispersedinthe gastrointesti-nalmucosaandrepresentingabout80–88%oftumorsofthe appendix.3,4
Theappendixisthesecond mostfrequentsiteofonset of neuroendocrine tumors (NET) throughout the digestive tract, with a frequency of 25–30%,5 after tumors of the
smallintestine.6,7Usuallythesetumorsarediagnosedduring
appendectomies,anditisestimatedthatateach100 appen-dectomiesperformedyearly,atleastonecaseisNET.8Others,
likeFernandoetal.,demonstrateanincidenceof0.3–0.7%of thehistopathologicalfindingsinappendectomies.9
Theapproximateincidenceofthisneoplasmis2–3cases permillion,withapreferenceforfemalesof2–4:1,10butwith
noracepredilection.Thepeakincidenceisbetween15and19 yearsinwomenand20–24yearsinmen.10
Thepreoperativediagnosisofamalignantneoplasmofthe appendixisrarelyperformedbecauseofitsnonspecific clini-calpicture,oftencompatiblewithanacuteappendicitis.11
Asfortreatment,consideringthatthediagnosisisusually establishedbythepathologistduringthepostoperativeperiod, itisuptothesurgeonthetask,sometimeshard,todetermine, throughthepathologyreport(basicallyanalyzingtumorsize anditslocationintheappendix,thepatient’sageandpresence ofmetastases), ifthepatient willbetreated withasecond surgicalintervention,thistimeofamoreaggressivetype,in theformofrighthemicolectomy.
sideofSãoPauloandgreater SãoPaulointhoserare cases ofappendiculartumors,withemphasisontheimportanceof thesedescriptions,consideringthatprobablyfewsurgeonsin particularwillacquireanextensiveexperienceinthesecases.
Patients
and
methods
Thisisaretrospectiveanalysisof237patientswhounderwent appendectomyfromSeptember2010toSeptember2012inthe HospitalSantaMarcelina-SP.
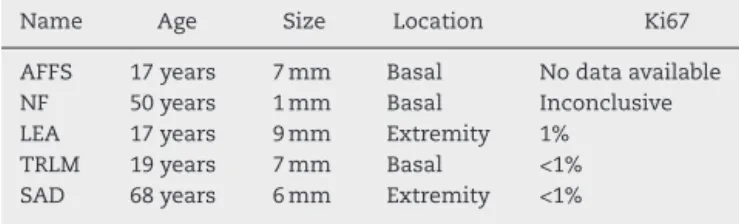
Dataforage,gender,baselineclinicalpicture,surgical find-ingsofpatientsundergoingappendectomy,withsubsequent anatomicaland immunopathologicaldiagnosisofcarcinoid tumoroftheappendixwereevaluated.Inthissearch,we stud-ieddataonmacroscopiclocationofthetumoranditssize, aswell asits histopathologic features.Regarding immuno-histochemistry,weanalyzedpositivetumormarkersandKi67 index.
Next,additionaltestswereperformedinordertoachievea bettertumorstagingandfortheapproachtobeadopted,with subsequentfollow-upandclinicaloutcomeanalysis.
Results
During the study period between September 2010 and September2012,237appendectomieswereperformedatthe departmentofgeneralsurgery,HospitalSantaMarcelina,São Paulo. Of this total, carcinoid tumor of the appendix was diagnosed in 5 patients, which corresponds to 2.1% of all appendectomiesperformed(Fig.1).
Itisworthnotingthatallpatientswerereferredtothe colo-proctologyoutpatientclinic,andoneofthesepatientscame fromanexternalservice.
Astothe gender, 4patients (80%)were female and the averageagewas34.2years,witharangeof17–68years.In all patients the initialhypothesis for indicationof surgery hadbeenacuteappendicitis,withanintraoperativefindingof necroperforated-stageacuteappendicitisin3patients(60%)
Pathological result Carcinoid
tumor 2%
Appendicitis 98%
Fig.1–Percentageofcarcinoidtumorsbypathological diagnosisafterappendectomy.
Table1–Age,localizationdata,tumorsizeand
immunohistochemistryofthecarcinoidtumorandcecal appendixoperations.
Name Age Size Location Ki67
AFFS 17years 7mm Basal Nodataavailable
NF 50years 1mm Basal Inconclusive
LEA 17years 9mm Extremity 1%
TRLM 19years 7mm Basal <1%
SAD 68years 6mm Extremity <1%
and phlegmonous-stage acute appendicitis intwo patients (40%).
Table1showsdataregardingpathologicaland immunohis-tochemistryexaminations.
A conduct of right hemicolectomy was adopted in two patientsandwatchfulwaitingfortheotherthree;thesurgical choiceswereduetothefactthat,inthefirstpatient,a mas-sivemesoappendixinvasionwasobserved;andinthesecond patient,theimmunohistochemistryreportwasinconclusive fordefiningtumorhistogenesis.
Discussion
Carcinoid tumors are neoplasms of the diffuse neuroen-docrinecellsystemwithgeneticinvolvementinitsetiology, with possible deletion of the gene PLC3 and consequent uncontrolledgrowthofneuroendocrinecells,distortionofthe apoptosisprocessanddevelopmentofneoplasms.12,13
Thefivecasesofcarcinoidtumoroftheappendixdescribed in this study present an incidence of 2.1% of the total of 237appendectomiesperformedintheperiodoftwoyearsat theHospitalSantaMarcelina,coincidentwiththeincidence describedintheliterature.11
Importantly,malignantneoplasmsoftheappendix, regard-less of histological type, are presented most of the time withaclinicalpicturehighlysuggestiveofacuteappendicitis (about 68%),probablydue totheobstruction ofthe appen-diceallumenbytheneoplasticinjury,causinganoverlapping infection.14,15 Innoneofthecasesherereporteda
preoper-atory suspicion ofcancer ofthe appendix was raised; and inall reportsthe initialhypothesis wasacuteappendicitis, althoughinonepatient(NF)themedicalhistorywithits evolu-tiontimeoffivedaysdidnotmatchthephysicalexamination. Thedefinitivediagnosis ofneoplasiaanditshistologictype areconfirmedonlybyhistologicalandimmunopathological studiesofthesurgicalspecimen.
Consistent with the literature,4 in the present study a
higher incidence of neuroendocrine tumor (NET) of the appendixwasfoundinfemales,with80%ofcases(4/5),and withahigherprevalenceinyoungpatients,withameanage of43.2years.Largeseriesintheliteratureindicatethatthe meanagerangedfrom27to40years.10
Withrespecttocarcinoidtumorsoftheappendix,themost frequentlocationisatitsextremityin62–78%ofcases;and generallybetween70and95%ofthetumorsmeasurelessthan 1cm.16,17 Morespecifically,Roggoetal.14reportthat80%of
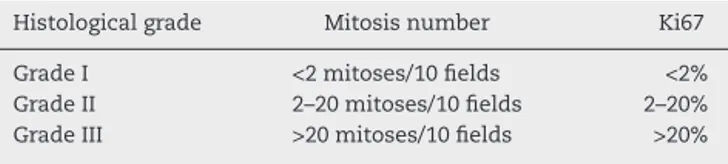
Table2–Histologicalgradebasedonthemitosis numberandKi67percentage.
Histologicalgrade Mitosisnumber Ki67
GradeI <2mitoses/10fields <2%
GradeII 2–20mitoses/10fields 2–20%
GradeIII >20mitoses/10fields >20%
Table3–TNMstagingofcarcinoidtumorofthe appendix.
T-primarytumor
Tx Aprimarytumorcannotbeassessed
T0 Noevidenceofprimarytumor
T1 Tumor≤1cminvadingsubmucosaand
muscularispropria
T2 Tumor≤2cminvadingsubmucosa,
muscularispropriaand/orminimalserosalor mesoappendicealinvasion(upto3mm)
T3 Tumor>2cmand/ormassiveserosalor
mesoappendicealinvasion(>3mm)
T4 Tumorinvadingperitoneum/otherorgans
N-regionallymphnodes
Nx Regionallymphnodescannotbeassessed
N0 Noregionallymphnodemetastasis
N1 Presenceofregionallymphnodemetastasis
M-Metastasis
Mx Adistantmetastasiscannotbeassessed
M0 Nodistantmetastasis
M1 Presenceofdistantmetastasis
Table4–Clinicalstaging.
Clinical stage
T-primary tumor
N-lymph nodes
M-metastasis
I T1 N0 M0
IIA T2 N0 M0
IIB T3 N0 M0
IIIA T4 N0 M0
IIIB AnyT N1 M0
IV AnyT AnyN M1
carcinoidtumorsmeasuredlessthan1cm,and40%ofthem werelocatedattheextremityoftheappendix.
Recentconsensusestablishedbythe European Neuroen-docrine Tumor Society (ENETS)proposes a grading system forNETsofthestomach,duodenumandpancreas,basedon mitotic count and/or immunohistochemical assessment of Ki67,aproliferationmarker(Table2).18
Another model widely used for carcinoid tumor of the appendixstagingisthatalsoproposedbyENETSin2007and presentedinTables3and4.19
Surgical resection is the most widely established treat-mentforpatientswithcarcinoidtumoroftheappendix.Itis knownthat,forlesionssmallerthan1cm,theappendectomy achieveshigh curerates(near 100%). Intumorsmeasuring between1and 2cm andwithoutlymphnode involvement, theappendectomyisalsoindicated. Ifthereislymphnode involvement,itbecomesnecessaryaprocedureofright hemi-colectomy, although presenting metastases around 3%. In patientswithtumorslargerthan3cm,righthemicolectomy
alsoisthe best therapeuticoption,but withahigh rateof metastases(about80%).20,21Totheseindications,wemustalso
addthecaseswithmesoappendixinvasion.22
Furthermore,someindicationsforamoreaggressive inter-vention,besidesthediameterofthemass,aretheextentof themesoappendixtumor,itslocationatthebaseofappendix, subserosallymphaticinvasion,andageofthepatient.These criteriaforabroadersurgeryhavegreatersignificancewhen decidingbetweenanappendectomyorarighthemicolectomy inpatientswithtumorswith1–2cm.23
Alsowithrespecttoprognosis,Itisknownthattheriskof metastasisintumorsmeasuringlessthan1cmindiameteris zero;fortumorsof1–2cm,thisriskis0–11%;andintumors largerthan2cm,theriskofmetastasisisconsiderablyhigher, 30–60%.11
StudyconductedbytheAbdominal-PelvicSurgeryService at INCA5 evaluated 13 patients operated at, or referenced
to,thatinstitutionbetween1996and2008.Apredominance of female patients (5.5:1) was noted, with a mean age of 44.7 years.Thetumorsizerangedfrom 0.3to6cm, witha medianof2.3cm;andintwocasesthepatientshavestarted thediseasewithadistantlesion.Furthermore,itwasshown that,afterameanfollow-upof32months,10patientswere alive(77%),one(7.7%)waslosttofollow-up,andtwo(15.3%) died.
Conclusion
Themedicalconductafterthediagnosisofacarcinoidtumor oftheappendixmustbebasedindataprovidedby patholog-icalandimmunohistochemicalstudies,besidesthejudicious judgment of the treating physician. In addition (and also because this tumor mainly affects relatively young indi-viduals), we must proceedwith the oncological follow-up, despiteadoptingaconservativeapproach,sincethesepatients present anincreasedriskofsynchronousormetachronous malignancies in percentages that can reach 29%, par-ticularly in the gastrointestinal tract, breast, cervix and endometrium.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.RizoliSB,MantovaniM,TrentiniJLB,CaponeNetoA. Carcinóidedoapêndice-achadoincidental.RevBras Coloproct.1990;10:24–6.
2.OberndorferS.UberdiekleinenDunndarmCarcinome.Verh DtschGesPathol.1907;11:113–6.
3.GuptaSC,GuptaAK,KeswaniNK,SinghiPA,TripathiAK, KrishnaVl.Pathologyoftropicalappendicitis.JClinPathol. 1989;42:1169–72.
5. SilvaRL,LinharesE,Gonc¸alvesR,RamosC.Tumores NeuroendócrinosdoApêndiceCecal:ExperiênciadoInstituto NacionaldeCâncer.RevBrasilCancerol.2010;56:463–70.
6. AraújoJS,JúniorRAC,SalibasGAM,PisolerLT,DiasACM, RibeiroRG.Tumorcarcinoidedeintestinodelgado.RevMéd MinasGerais.2010;20:469–72.
7. FernandesLC,PuccaL,MatosD.Diagnósticoetratamentode tumorescarcinoidesdotratodigestivo.RevAssocMedBras. 2002;48:87–92.
8. StinnerB,RothmundM.Neuroendocrinetumours (carcinoids)oftheappendix.BestPractResClin Gastroenterol.2005;19:729–38.
9. FernandoUherekP,ClaudiaBarríaA,CristóbalLarraínT, EstefaníaBirrerG.Carcinoideapendicular.Comunicaciónde 6casosyactualizacióndeltema.CuadCir.2004;18:52–6.
10.BrombergSH,ReisPMJr,WaisbergJ,Franc¸aLCM,GodoiAC. Tumorescarcinóidesdoapendicececal.RevBrasColoproct. 2000;20:9–13.
11.MercioAAP,WeindorferM,WeberAL,ManoAC.Neoplasias malignasprimáriasdeapêndicececal.MedicinaRibeirão Preto.1999;32:193–8.
12.O’DowdG,GosneyJR.Absenceofoverexpressionofp53 proteinbyintestinalcarcinoidtumors.JPathol. 1995;175:403–4.
13.ÖbergK.Biologicalaspectsofneuroendocrine
gastro-enteropancreatictumours.Digestion.1996;57Suppl. 1:42–4.
14.RoggoA,WoodWC,OttingerLW.Carcinoidtumorsofthe appendix.AnnSurg.1993;217:385–90.
15.DeansGT,SpenceRAJ.Neoplasticlesionsoftheappendix. BritJSurg.1995;82:299–306.
16.GoedeAC,CaplinME,WinsletMC.Carcinoidtumourofthe appendix.BrJSurg.2003;90:1317–22.
17.PickhardtPJ,LevyAD,RohrmannCAJr,KendeAI.Primary neoplasmsoftheappendix:radiologicspectrumofdisease withpathologiccorrelation.Radiographics.2003;23:645–62.
18.RindiG,KloppelG,AlhmanH,CaplinM,CouvelardA,Herder WW,etal.TNMstagingofforegut(neuro)endocrinetumors:a consensusproposalincludingagradingsystem.Virchows Arch.2006;449:395.
19.RindiG,KlöppelG,CouvelardA,KomminothP,KörnerM, LopesJM,etal.TNMstagingofmidgutandhindgut(neuro) endocrinetumors:aconsensusproposalincludingagrading system.VirchowsArch.2007;451:757–62.
20.AndradeLC,SoaresJD,BarbosaMVJ,CassisFM,SouzaAM. Revisãodeliteratura:tumorcarcinóidedeapêndice.RUn Alfenas.1999;5:247–9.
21.LopesAGJr,SaquetiEE,CardosoLTQ.Tumordoapêndice vermiforme.RevColBrasCirur.2000;28:228–9.
22.MoertelCG,WeilandLH,NagorneyDM,DockertyMB. Carcinoidtumoroftheappendix:treatmentandprognosis.N EnglJMed.1987;317:1699–701.