jcoloproctol(rioj).2014;34(4):198–201
Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Original
article
Retrospective
analysis
of
patients
undergoing
bowel
transit
reconstruction
in
a
tertiary
referral
hospital
of
São
Paulo’s
east
side
夽
Isaac
José
Felippe
Corrêa
Neto
a,b,∗,
Otávio
Nunes
Siá
a,
Eduardo
Augusto
Lopes
a,
Rodrigo
Padilla
c,
Katiucia
Tereza
Molezin
Portugal
c,
Alexander
Sá
Rolim
a,b,
Rogério
Freitas
Lino
Souza
a,
Hugo
Henriques
Watté
a,b,
Laércio
Robles
c aColoproctologyService,HospitalSantaMarcelina(HSM),SãoPaulo,SP,BrazilbBrazilianColoproctologySociety(SBCP),SãoPaulo,SP,Brazil
cGeneralSurgeryService,HospitalSantaMarcelina,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1November2013 Accepted11August2014
Availableonline3September2014
Keywords:
Ostomy
Boweltransitreconstruction Morbidityandmortality
a
b
s
t
r
a
c
t
Introduction:Themorbidityandmortalityofpatientsundergoingboweltransit reconstruc-tionreachsignificantvalues.Perhapsthisandotherfactorscouldexplainwhy30–60%of patientsendupwithdefinitiveostomies,eventhosewithinitiallytemporaryostomies,due totheprocedurerisks.
Objective:Toanalyzeretrospectivelythemedicalrecordsofpatientsundergoingbowel tran-sitreconstructioninoneoftheSUSreferralhospitalsinSãoPaulofromOctober2008to December2011.
Results:Themeanageofourpatientswas53.9yearsand54%ofthose100patients stud-iedbetweenOctober2008andDecember2011hadsignificantcomorbidity.Theindication forcreatinganinitialostomywasmalignancyin43%,andthemeanstomaduration14.3 months.Themortalityratewas6%.
Conclusion:Although the bowel transit reconstruction is a procedure quite desired by patients,its indicationshouldbecarefullyevaluated,withanappropriateconsentfrom thepatient.
©2013SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
夽
StudyconductedbytheMedicalResidencyProgramofColoproctology,DepartmentofGeneralSurgery,HospitalSantaMarcelina,São Paulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](I.J.F.CorrêaNeto).
http://dx.doi.org/10.1016/j.jcol.2014.08.003
jcoloproctol(rioj).2 0 1 4;34(4):198–201
199
Análise
retrospectiva
dos
pacientes
submetidos
à
reconstruc¸ão
de
trânsito
intestinal
em
hospital
terciário
de
referência
da
zona
leste
de
São
Paulo
Palavras-chave:
Ostomia
Reconstruc¸ãodetrânsito intestinal
Morbi-mortalidade
r
e
s
u
m
o
Introduc¸ão:Amorbi-mortalidadedepacientessubmetidosàreconstruc¸ãodetrânsito intesti-nalalcanc¸avaloressignificativose,poresseeoutrosfatores,talvezseexpliqueofatoque de30a60%dosportadoresdeostomiaintestinalterminalpassamapossuí-lademaneira definitiva,apesarde,namaiorpartedasvezes,elaserrealizadacomoprocedimento pro-visóriocomoargumentodemaiorseguranc¸adopaciente.
Objetivo: Analisarretrospectivamenteosdadosdeprontuáriodepacientessubmetidosà reconstruc¸ãodetrânsitointestinalemumdoshospitaisdereferênciadoSUSnacidadede SãoPaulonoperíododeoutubrode2008adezembrode2011.
Resultados: Amédiadeidadedospacientesfoide53,9anose54%dos100pacientes estuda-dosnoperíododeoutubrode2008edezembrode2011padeciamdealgumacomorbidade.A indicac¸ãoparaconfecc¸ãodaostomiainicialdecorreudedoenc¸amalignaem43%eotempo médiodepermanênciacomoestomafoide14,3meses.Ataxademortalidadefoide6%.
Conclusão: Emboraareconstruc¸ãodotrânsitointestinalsejaumprocedimentobastante desejadopelospacientes,suaindicac¸ãodeveserbastantecriteriosa,comconsentimento adequadoporpartedopaciente.
©2013SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
SincethefirstdescriptionofcolostomybytheFrench physi-cian Littré, the use of ostomy and their indications were modifiedthroughtheages.However,themorbidityand mor-talityassociatedwithboweltransitrestorationarestillcause for concern. In this regard, it is known that overall mor-bidityratescanreach 50%,andmortalityratesvaryfrom 0 and 4.5%.1–3 However,when specifically analyzingpatients
whounderwentboweltransitreconstructionwithaprevious Hartmann-typeostomy,thevaluesofmortalitycanreachupto 28%.4,5
Theoperationinitially described in1921byHenri Hart-mann Albert is of fundamental importance in cases of emergency colorectal surgery and, in addition, it must be emphasized that this typeof procedure is commonly per-formedonpatientswithsevereconditions,6 suchthatonly
about 30–60%ofthesepatients are referred tobowel tran-sitreconstruction.4,5 However,onemustkeepinmindthat,
according to Vaid et al., 32.3% of patients undergoing ini-tialsurgerywithHartmann-typeterminalcolostomyfailedin theirboweltransitreconstruction.7
Thesepercentagesdemonstratetheimportanceof deter-mining the factors that influence the clinical outcome of patients undergoing surgical bowel transit reconstruction. Amongthesefactors,thereistheprocedureperformedatthe initialoperationand the complications ofthis procedure,8
the surgical technique used in the restoration of bowel continuity and the experience of the surgeon, the type (terminal- or loop-) of ostomy9 and the conscious use
of antibiotics and the pre- and postoperative care,10 in
addition to the risk factors associated with the patient itself.
Objectives
To analyze retrospectively data obtained from electronic medical records of patients who underwent bowel transit reconstruction inoneofSUS referralTeachingHospitalsin SãoPaulo.
Patients
and
methods
ThisisaretrospectivestudyconductedbetweenOctober2008 andDecember2011involving100patientstreated,monitored andoperatedbytheMedicalResidencyServiceof Coloproctol-ogy,HospitalSantaMarcelina,SãoPaulo.
Wesoughttoanalyzedataobtainedfromelectronic medi-calrecordsinrelationtogender,age,comorbidities(including smoking),anestheticriskclassification(ASA),meanostomy duration primaryindication (benignor malignant disease), typeofanesthesiausedforboweltransitreconstruction, mor-talityandmeanin-hospitallengthofstay.
Thestudy wasconductedattheColoproctology Service, HospitalSantaMarcelina,SãoPaulo,andapprovedbythe Eth-icalCommitteeunderNo.27/13.
Results
Inthestudyperiod,betweenOctober2008andDecember2011, the Medical Residency Service of Coloproctology, Hospital Santa Marcelina,SãoPaulo,performed264elective colorec-taloperations,comprising100boweltransitreconstructions (37.8%).
200
jcoloproctol(rioj).2 0 1 4;34(4):198–201Gender
Female 43%
Male 57%
Fig.1–Genderdistribution.
presentin54patients,mainlyhypertension,diabetes melli-tus,smokingandChagasdisease.Amongthosepatientswith comorbidity,23(42.6%)hadanassociationoftwoormore med-icalconditions.
Theindicationfortheinitialostomycreationwas malig-nantdiseasein43%(Fig.2)andthemeanstomadurationwas 14.3months.Fifty-twopatientshadterminalostomy,notably ofHartmanntype.Regardingtheclassificationofanesthetic risk(ASA),30%were ASAI, 56%wereASAIIand14%were ASAIII(Fig.3).Ontheotherhand,whenstratifyingtheinitial indicationforstomaconstruction,15%ofthesesurgeriescan beconsideredasscheduledprocedures,particularlydiverting colorectalanastomosis.
Generalanesthesiawasusedin40%ofpatients,peripheral blockin34%andanassociationbetweenbothtypesin26%of patients.
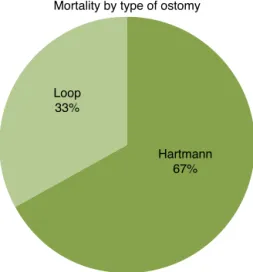
Complicationsinthesurgicalprocedureoccurredin3%of patients,andnoneoftheseprogressedtodeath.Sixpercent ofthepatientsundergoingboweltransitreconstructiondied, and66.7%ofthesedeceasedpatientshadbeentreatedwitha Hartmann-typeterminalcolostomy(Fig.4)and75%ofthem
57%
43%
Malignant disease Benign disease
Fig.2–Initialindicationofstomaconstruction.
30%
56%
14%
ASA I ASA II ASA III
Fig.3–Classificationofanestheticrisk.
hadbeenreoperated,duetoanastomoticdehiscencefollowed byfecalperitonitis.
Themeanin-hospitallengthofstaytimewas7.66days, witharangeof4–36days.However,whenonelooks specif-ically atthe hospitalizationtime amongpatientsin whom clinicalorsurgicalcomplicationsoccurredbutnotprogressed todeath,thismeantimewas27.25days.
Discussion
Inthepresentstudy,themeanagestandsinthe5thdecade. Thisfindingislikelytoreflectthepercentageofmalignant dis-easesasacauseforstomaindication(43%).However,when oneanalyzesstudieswhosemaincauseforostomycreation was some traumaticinjury (i.e., a gunshot), alower mean age4,11wasfound,whichmayinfluencethefinalresultsfor
morbidityandmortality.
Melottietal.12–16studied273ostomizedpatientsbetween
2000and2010andfoundameanageof64.5yearswith53.1% ofpatientsbeingfemale.Ithasbeenshown,asinourstudy, thatthemainindicationforostomycreationwascolorectal cancer,accountingfor45.8%ofcases.
Loop 33%
Hartmann 67% Mortality by type of ostomy
jcoloproctol(rioj).2 0 1 4;34(4):198–201
201
Themean ostomy duration inour study was similar to otherresultsfoundinnationalliterature.6Silvaetal.13noted
ameanostomydurationof15.7months(3–284months). How-ever, this duration undergoes variation, mainly dueto the initialindicationfortheintestinaldiversion,forexample, neo-plasticdisease,theneedforadjuvantchemotherapy6andalso
toanoverloadofthehealthservicesystemcapacity.4
Wefoundsimilarhospitallengthofstaytothosedescribed in the literature. In addition, studies show a longer in-hospital period in caseswith surgical times over 300min, intra-operativeadhesions,bowellesionsduringsurgery, ana-stomoticfistulae,abdominalwallinfectionsandtheneedfor IntensiveCareUnituse.6Inourstudy,allpatientsthathad
spentmorethan 10daysofin-hospital lengthofstaywere thoseundergoingreoperation.
Asregardstomortalityanalysis,ouroverallratewas6%, with 4.1%for casesof loop ostomy and 7.7% for terminal ostomy. When reviewing the literature, it appears that a greaternumberofoveralldeathsoccurredinourstudy com-paringtootherpublishedstudies.However,itshouldbeborne inmindthatourpatientswereolderthanthoseinthe stud-ies reviewedand, inaddition, ourpatients who died were also older (67.5 years). Furthermore, it should be empha-sizedthatoneofthepatientswhodiedafterterminalostomy reconstructionhadactinicdisease,andperhapsinthiscase thesurgical indicationcould berevised, asoccurs incases describedintheliterature.6
Bocicetal.14observedamortalityrateof1.7%.InBrazil,
Habr-Gama15 hadanoverallrateof3.6%.Bahtenetal.4had
onedeathafterboweltransitreconstructionamongatotalof 42patients(2.3%).However,whenthemortalityforsurgical reconstructionofboweltransitafteraninitialHartmann pro-cedureisanalyzed,ourdataareconsistentwiththeliterature, withratesupto28%.5,6
Whenstratifyingthepatientswhodied,themeanagewas 67.5years,rangingbetween52and79years.Thegender dis-tributionwasequivalent,and4of6patients(66.7%)exhibited terminalostomy.Inthisgroupofpatients,wefoundthatonly onehadnocomorbidities(16.7%),includingcasesofsmoking. Thesereportedpercentagesshowtheimportanceof deter-mining the factors that influence the clinical outcome of patientsundergoingsurgicalreconstructionofboweltransit. Amongthesefactors,standouttheprocedureperformedat theinitialoperationandthecomplicationsofthisprocedure, thesurgicaltechniqueusedintherestorationofbowel con-tinuity and the surgeon’s experience, the conscious use of antibioticsandpre-andpostoperativecare,aswellasthose riskfactorsassociatedwiththepatient.11,16
Conclusion
Boweltransitreconstruction,althoughgenerallyaprocedure quitedesiredbythepatient,isnotfreefromcomplications. Therefore,onemustalwaysclarifythepatientaboutthemain complications,includingthepossibilityofalethaloutcome. Inaddition, thededicatedteammusttakeinto accountthe contraindicationsoftheprocedure.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.PittmanDM,SmithLE.Complicationsofcolostomyclosure. DisColonRectum.1985;28:836–43.
2.KnoxAJ,BirkettFDH,CollinsCD.Closureofcolostomy.BrJ Surg.1971;58:559–72.
3.BahtenLCV,NicoluzziJEL,SilveiraF,NicollelliGM,Kumagai LY,DeLimaVZ.MorbimortalidadedaReconstruc¸ãode TrânsitoIntestinalColônicaemHospitalUniversitário– Análisede42Casos.RevBrasColoproctol.2006;26:123– 7.
4.DeschampsC,TirnaksizBM,DarbandiR,TrastekVF,AllenMS, MillerDL,etal.Earlyandlong-termresultsofprosthetic chestwallreconstruction.JThoracCardiovascSurg. 1999;117:588–91[discussion591-2].
5.ChangRR,MehraraBJ,HuQY,DisaJJ,CordeiroPG. Reconstructionofcomplexoncologicchestwalldefects:a 10-yearexperience.AnnPlastSurg.2004;52:471–9.
6.SilvaRG,CastroJúniorGR,FerreiraCLM,LuzMMP,Conceic¸ão AS,Lacerda-FilhoA.Reconstruc¸ãodetrânsitointestinalapós confecc¸ãodecolostomiaàHartmann.RevColBrasCir. 2010;37:17–22.
7.VaidS,WalletJ,LittJ,BellT,GrimR,AhuaiV.Applicationofa tertiaryreferralscoringsystemtopredictnonreversalof Hartmann’sprocedurefordiverticulitisinacommunity hospital.AmSurg.2011;77:814–9.
8.Biondo-SimöesMLP,BrennerS,LemosR,DuckD,ReySD. Análisedasconsequênciaspós-operatóriasemcolostomias. ActaCirBras.2000;15Suppl.3:53–7.
9.DemetriadesD,PezikisA,MelissasJ,ParekhD,PicklesG. Factorsinfluencingthemorbidityofcolostomyclosure.AmJ Surg.1988;155:594–6.
10.CuriA,MascarenhasJCS,MoreiraJuniorH,AlmeidaAC, MoreiraJPT,MoreiraH,etal.Morbimortalidadeassociadaà consequênciadotrânsitointestinal:análisede67casos.Rev BrasColoproctol.2002;22:88–97.
11.MarqueseSilvaS,MeloCCL,AlmeidaSB,QueirozHF,Soares AF.Complicac¸õesdasOperac¸õesdeReconstruc¸ãodoTrânsito Intestinal.RevBrasColoproctol.2006;26:24–7.
12.MelottiLF,BuenoIM,SilveiraGV,SilvaMEN,FedosseE. Characterizationofpatientswithostomytreatedatapublic municipalandregionalreferencecenter.JColoproctol. 2013;33:70–4.
13.SilvaJB,CostaDR,MenezesFJC,TavaresJM,MarquesAG, EscalanteRD.Perfilepidemiológicoemorbimortalidadedos pacientessubmetidosàreconstruc¸ãodetrânsitointestinal: experiênciadeumcentrosecundáriodoNordestebrasileiro. ArqBrasCirDig.2010;23:150–3.
14.BocicGA,JensenCB,AbedrapoMM,GarridoRC,PérezGO, CúeneoAZ.ColostomíaseIleostomías:8A ˜nosde consequênciaclínica.RevHospClinUnivChile. 1999;10:195–200.
15.Habr-GamaA,TeixeiraMG,VieiraMJF,MiléuLF,LaurinoNeto R,PinottiHW.Operac¸ãodeHartmannesuasconsequências. RevBrasColoproctol.1997;17:5–10.