BrazJOtorhinolaryngol.2017;83(1):98---104
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Obstructive
sleep
apnea
and
oral
language
disorders
夽
Camila
de
Castro
Corrêa
a,∗,
Maria
Gabriela
Cavalheiro
b,
Luciana
Paula
Maximino
b,
Silke
Anna
Theresa
Weber
aaUniversidadeEstadualPaulista‘‘JúliodeMesquitaFilho’’(FM---UNESP),FaculdadedeMedicinadeBotucatu,Departamentode
OftalmologiaeOtorrinolaringologia,Botucatu,SP,Brazil
bUniversidadedeSãoPaulo(FOB---USP),FaculdadedeOdontologiadeBauru,DepartamentodeFonoaudiologia,Bauru,SP,Brazil
Received14June2015;accepted10January2016 Availableonline28April2016
KEYWORDS Childlanguage; Languagedisorders; Speech,languageand hearingsciences; Obstructivesleep apnea
Abstract
Introduction:Childrenandadolescentswithobstructivesleepapnea(OSA) mayhave conse-quences,suchasdaytimesleepinessandlearning,memory,andattentiondisorders,thatmay interfereinorallanguage.
Objective:Toverify,basedontheliterature,whetherOSAinchildrenwascorrelatedtooral languagedisorders.
Methods:AliteraturereviewwascarriedoutintheLilacs,PubMed,Scopus,andWebofScience databasesusingthedescriptors‘‘ChildLanguage’’AND‘‘ObstructiveSleepApnea’’.Articles thatdidnotdiscussthetopicandincludedchildrenwithothercomorbiditiesratherthanOSA wereexcluded.
Results:Intotal,noarticleswerefoundatLilacs,37atPubMed,47atScopus,and38atWeb ofSciencedatabases.Basedontheinclusionandexclusioncriteria,sixstudieswereselected, allpublishedfrom2004to2014.Four articlesdemonstratedanassociationbetweenprimary snoring/OSAandreceptivelanguageandfourarticlesshowed anassociationwithexpressive language.Itisnoteworthythatthearticlesuseddifferenttoolsandconsidereddifferentlevels oflanguage.
Conclusion:Thelatediagnosisandtreatmentofobstructivesleepapneaisassociatedwitha delayinverbalskillacquisition.Theprofessionalswhoworkwithchildrenshouldbealert,as mostofthephoneticsoundsareacquiredduringages3---7years,whichisalsothepeakagefor hypertrophyofthetonsilsandchildhoodOSA.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽
Pleasecitethisarticleas:CorrêaCC,CavalheiroMG,MaximinoLP,WeberSA.Obstructivesleepapneaandorallanguagedisorders.Braz JOtorhinolaryngol.2017;83:98---104.
∗Correspondingauthor.
E-mail:[email protected](C.C.Corrêa).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.01.017
1808-8694/©2016Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen
Obstructivesleepapneaandorallanguagedisorders 99
PALAVRAS-CHAVE Linguageminfantil; Transtornosda linguagem; Fonoaudiologia; Apneiadosonotipo obstrutiva
Apneiaobstrutivadosonoealterac¸õesdalinguagemoral
Resumo
Introduc¸ão: Crianc¸aseadolescentescomApneiaObstrutivadoSono(AOS)podemapresentar sonolênciadiurna,alterac¸ões deaprendizado, memóriaeatenc¸ão,quepodem interferirna linguagemoral.
Objetivo: Verificar,combasenaliteratura,seaAOSapresentacorrelac¸ãocomalterac¸õesda linguagemoral.
Método: FoirealizadarevisãobibliográficanasbasesdedadosLilacs,Pubmed,ScopuseWebof Science,apartirdaspalavras-chaves‘‘LinguagemInfantil’’AND‘‘ApneiadoSonoTipo Obstru-tiva’’.Osartigosquenãoserelacionavamaotemaforamexcluídos,bemcomoestudoscom crianc¸asqueapresentassemoutrascomorbidades,alémdaAOS.
Resultados: Foramlocalizados0artigosnabaseLilacs,37naPubmed,47naScopuse38na WebofScience.Apartirdoscritériosdeinclusãoeexclusão,foramselecionadosseisestudos, publicados em 2004 a2014. Dosartigosincluídos, observou-seem quatro artigosarelac¸ão dogrupocomroncoprimário/SAOScomaLinguagemReceptivaeemquatroartigosarelac¸ão dessapopulac¸ãocomaLinguagemExpressiva.Ressalta-sequeosartigosutilizaraminstrumentos diferenteseconsideraramníveisdiversificadosdaLinguagem.
Conclusão:OdiagnósticoetratamentotardiodeAOSresultamemalterac¸õessignificantesna qualidadedaaquisic¸ãoverbal.Torna-seimprescindívelaatenc¸ãodosprofissionaisqueatuam comoapopulac¸ãoinfantilparaesteaspecto,umavezquegrandepartedossonsdafalasão adquiridosentre3---7anos,quecorrespondeao períododepicodeocorrênciadehipertrofia adenoamigdalianaeAOSnainfância.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
ObstructiveSleepApnea (OSA) is characterized by partial and/or complete upper airway obstruction during sleep, associated with increased respiratory effort, fragmented sleep, and/or gas exchange abnormalities.1,2 There are differences in what is observed in adults versus chil-drenwithrespecttopathophysiology,clinicalfeaturesand treatment.2 The pathophysiology of OSA in children is associatedwithapredominantpatternofpartial and per-sistent upperairwayobstruction, resultingin hypercapnia and intermittenthypoxia.3 Snoring, the main symptom of OSA, is present in the clinical picture of almost all chil-dren with the alteration. Other signs and symptoms such asforced mouth breathingwith costalretractions, sleep-walking,enuresisandnightsweats,coughing,gagging,and agitation during sleep are also part of the clinical pic-ture,andit iscommonfor thesechildren tomove around in search of positions that facilitate the passage of air.4 Treatment differsfromthatof adults:adenotonsillectomy isconsidered thegoldstandard treatment and,when per-formed for the proper indications, it benefits the child withrespect toneuropsychological,behavioral, and qual-ity of life issues; obese children exhibit a lower rate of success.5,6
ItisestimatedthattheprevalenceofOSAinhealthy chil-dren without other associatedclinical picture varies from 0.7% to 3%.7---10 The incidence is higher in the preschool range,anagewhenthereisagreaterdisproportionbetween thehypertrophyofthepalatineandpharyngealtonsilsand upperairwaydimensions.5Thisperiodisalsorecognizedas
privilegedfortheacquisitionanddevelopmentoflanguage andintenseneuroplasticityof thecentralnervoussystem, whichfavorslearning.11---14
AmongtheconsequencesofOSAinchildren,the associa-tionwithattentionandmemorydeficitsmustbeconsidered; that could impair information processing and recording, decreasing the learning capacity.15---17 The condition also affects the mood, expressive language skills, school per-formance, cognitive skills, and visual perception of this population.18---20
Because the reported frequency of OSA in the litera-tureoccurs duringan importantphase of developmentin preschoolchildrenandOSA’seffectonskillsinvolvedinthe languageacquisition process,learning, andschool perfor-mance, it is relevant to assess the development of oral languageinthesechildren.ThereisstrongevidenceofOSA association with neurocognitive deficits,6,17,19 but studies thatspecifically focused onthe developmentof language werenotretrievedfromtheliterature.
100 CorrêaCCetal.
The observation and measurement of allthese linguis-ticlevelscanonlybeachievedthroughtheapplication of protocolsspecificallydevelopedforthepatient’snative lan-guage that have comparative scores with normative data foreachagegroup.The onlystudydetailingthisaspectis a systematic review of the following tests usedto assess receptive oral language: the Peabody Picture Vocabulary Test, Peabody Picture Vocabulary Test-Revised (PPVT-R), Swedish Communication Screening at 18 months of act (SCS18),TestforReceptionofGrammar-2(TROG-2),Reynell Test, Reynell Language Development Scales, and Reynell DevelopmentalLanguageScales-II.Italsoemphasizedthat there are few tools and not all of them have validity studies.24
Therefore,thisstudyaimedtoverifywhetherthe pres-ence of OSA is associated with possible oral language alterations.
Methods
A literature search was carried out with no temporal limitation, using the keywords ‘‘Child Language’’ AND ‘‘Obstructive Sleep Apnea’’, as well as their counter-partsinPortuguese,‘‘LinguagemInfantil’’AND‘‘Apneiado SonoTipo Obstrutiva’’.Thesearch wasperformed infour databases:Lilacs,PubMed,Scopus,andWebofScience.
Theinclusioncriteriacomprisedarticleswritten onthe centraltopicofchildren/adolescentswithOSA,withfocus onoral language alterations. Thus, the exclusion criteria included: articles that assessed other concomitant medi-calconditionsthatjustifiedsleeporlanguagealterations, suchascleftlipandpalate,geneticsyndromes(Down, cra-niosynostosis,and velocardiofacial syndrome), and ADHD; thosewithfocusonmotorspeechdisorders,suchasspeech apraxia;andliteraturereviewarticles.Itisnoteworthythat thesearch was carriedout usingthe VPN (Virtual Private Network)systemandarticlesthatwerenotfullyavailable werealsoexcluded.
Articleselectionwascarriedoutbyreadingthetitlesand abstracts.Subsequently,thearticleswereanalyzedinfull, after which they weredefinitively included or not in the review.Thearticlesincluded inthereview wereanalyzed regarding their objectives, methods, results, and conclu-sions.Thespecificresultsoftheevaluationsregardingoral language,evaluatedorallanguagespecification(receptive and/orexpressive)werealsoanalyzed,andthelimitations ofeachstudywereidentified.
Results
ThesearchfoundnoarticlesinLilacs,37inPubMed,47in Scopus,and38inWebofSciencedatabases.
Afterfirstanalysis,readingthetitlesandabstracts,eight studieswereselected.Thelocationinoneormoredatabases wherethearticleswerefoundisshowninFig.1.
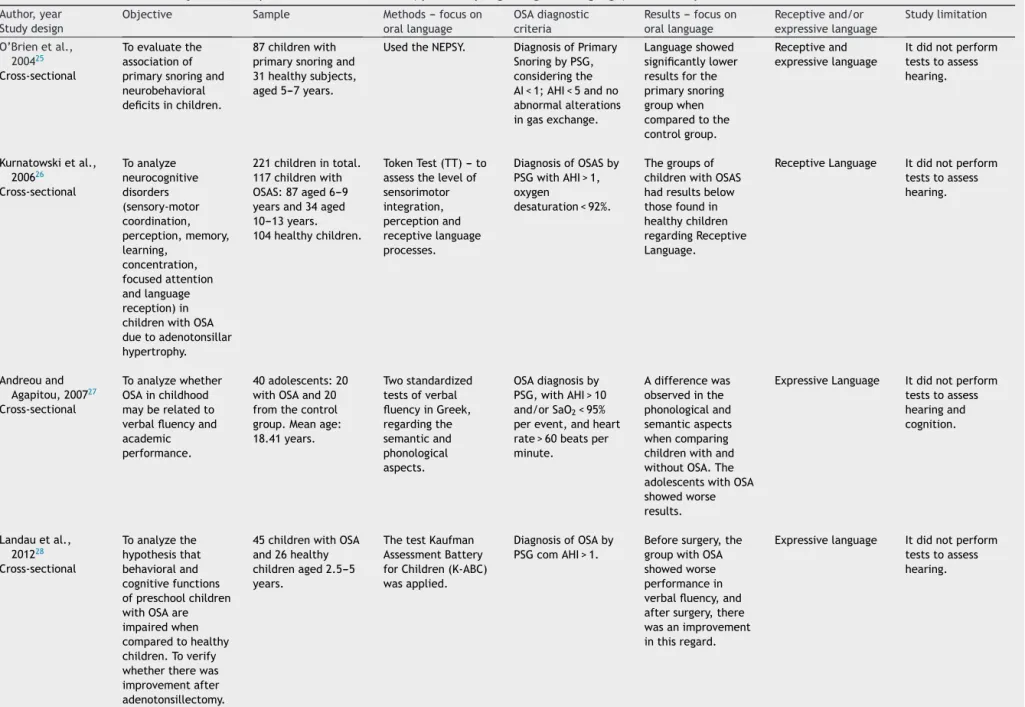
For the final inclusion, all articles were read in full, except two, whose full versions were not available and thuswereexcluded.Therefore,Table1showsthesix stud-iesincluded inthisstudy,withinformationonauthorship, year,journal,anddatabasefromwheretheywereretrieved, showninascendingchronologicalorder.
Table2showstheanalysisoftheincludedarticles.
Discussion
AkeyfeatureofcurrentstudiesonOSAisaninterdisciplinary approachreflecting thevaried andheterogeneous impair-ments that this condition may cause; treatment requires a holistic view of the individual for greatest effective-ness.
Duringthis search,weobserved thattheselected arti-clesonORALLANGUAGEwerepublishedonlyrecently.The diagnosisofOSAhasincreasedinrecentyears,31whichmay explaintheincreaseinthenumberofchildrenwithOSAand thehighernumberofcurrentscientificresearch investigat-ingtheseaspects.
Moststudieswerepublishedinpediatricjournals(four), one in sleep medicine, and one in neuropsychology. It is noteworthy that there were no publications in speech
Pubmed 1
0 1
4
1 0
1
Scopus ScienceWeb of
Figure1 Databasedescriptionoftheabstractsconsideredfor thereview,innumbers,alsoshowingwhentheywerefoundin morethanonedatabase.
Table1 Dataonauthorship,year,journal,anddatabaseofassessedarticles.
Authors Year Journal Database
O’Brienetal.25 2004 Pediatrics PubMed---Webofscience---Scopus
Kurnatowskietal.26 2006 IntJPediatrOtorhinolaryngol PubMed---Webofscience---Scopus
AndreouandAgapitou27 2007 ArchivesofClinicalNeuropsychology Webofscience
Landauetal.28 2012 PediatricPulmonology PubMed
Liukkonenetal.29 2012 IntJPediatrOtorhinolaryngol PubMed---Webofscience---Scopus
Obstructive sleep apnea and oral language disorders 101
Table2 Informationontheobjective,sample,methods,andresults(specificallyregardingorallanguage)oftheanalyzedarticles.
Author,year Studydesign
Objective Sample Methods--- focuson orallanguage
OSAdiagnostic criteria
Results--- focuson orallanguage
Receptiveand/or expressivelanguage
Studylimitation
O’Brienetal., 200425
Toevaluatethe
associationof
primarysnoringand
neurobehavioral
deficitsinchildren.
87childrenwith
primarysnoringand
31healthysubjects,
aged5---7years.
UsedtheNEPSY. DiagnosisofPrimary
SnoringbyPSG,
consideringthe
AI<1;AHI<5andno
abnormalalterations
ingasexchange.
Languageshowed
significantlylower
resultsforthe
primarysnoring
groupwhen
comparedtothe
controlgroup.
Receptiveand
expressivelanguage
Itdidnotperform
teststoassess
hearing. Cross-sectional
Kurnatowskietal.,
200626 Toanalyze neurocognitive disorders (sensory-motor coordination, perception,memory, learning, concentration, focusedattention andlanguage reception)in
childrenwithOSA
duetoadenotonsillar
hypertrophy.
221childrenintotal.
117childrenwith
OSAS:87aged6---9
yearsand34aged
10---13years.
104healthychildren.
TokenTest(TT)--- to
assessthelevelof
sensorimotor integration,
perceptionand
receptivelanguage
processes.
DiagnosisofOSASby
PSGwithAHI>1,
oxygen
desaturation<92%.
Thegroupsof
childrenwithOSAS
hadresultsbelow
thosefoundin
healthychildren
regardingReceptive
Language.
ReceptiveLanguage Itdidnotperform
teststoassess
hearing. Cross-sectional
Andreouand
Agapitou,200727
Toanalyzewhether
OSAinchildhood
mayberelatedto
verbalfluencyand
academic performance.
40adolescents:20
withOSAand20
fromthecontrol
group.Meanage:
18.41years.
Twostandardized
testsofverbal
fluencyinGreek,
regardingthe
semanticand
phonological aspects.
OSAdiagnosisby
PSG,withAHI>10
and/orSaO2<95%
perevent,andheart
rate>60beatsper
minute.
Adifferencewas
observedinthe
phonologicaland
semanticaspects
whencomparing
childrenwithand
withoutOSA.The
adolescentswithOSA
showedworse
results.
ExpressiveLanguage Itdidnotperform
teststoassess
hearingand
cognition. Cross-sectional
Landauetal.,
201228
Toanalyzethe
hypothesisthat
behavioraland
cognitivefunctions
ofpreschoolchildren
withOSAare
impairedwhen
comparedtohealthy
children.Toverify
whethertherewas
improvementafter
adenotonsillectomy.
45childrenwithOSA
and26healthy
childrenaged2.5---5
years.
ThetestKaufman
AssessmentBattery
forChildren(K-ABC)
wasapplied.
DiagnosisofOSAby
PSGcomAHI>1.
Beforesurgery,the
groupwithOSA
showedworse
performancein
verbalfluency,and
aftersurgery,there
wasanimprovement
inthisregard.
Expressivelanguage Itdidnotperform
teststoassess
102
Corrêa
CC
et
al.
Table2 (Continued)
Liukkonenetal., 201229
Toassessthe
associationbetween
sleep-disordered
breathingand
cognitivefunctionin
children.
44childrenwith
primarysnoringand
51healthyones,
aged1---6years.
TheNEPSY
assessmenttool
(comprehensionof
instructions,speeded
namingandbody
partnaming).
DiagnosisofPrimary
snoringbyPSG,with
AHI<1.Hypopnea
wasdefinedasan
airflowvolume
reductionof<50%,
followedby
awakening, oxyhemoglobin
desaturation>2%.
Thegroupofchildren
withprimarysnoring
obtainedthelowest
scoresinlanguage
functions
(comprehensionof
instructions,speeded
naming).
Receptiveand
expressivelanguage
Itdidnotperform
teststoassess
hearing. Cross-sectional
Yorbiketal.,201430 Toinvestigatethe
effectsofsnoring
andfragmented
sleeponmental
developmentin
preschoolchildren.
212children,37with
complaintsofsnoring
and25with
fragmentedsleep
complaints,aged
3.1---6years.
PeabodyPicture
VocabularyTestwas
used.
Througha
questionnaire.
Childrenwith
complaintsofsnoring
andwithfragmented
sleephadlower
scoresonlanguage.
ReceptiveLanguage Itdidnotperform
PSGassessmentand
didnotassess
hearing. Cross-sectional
Obstructivesleepapneaandorallanguagedisorders 103
therapy and audiology journals, i.e., those professional responsible for the understanding and speech therapy aspects of the peripheral and central auditory function, vestibularfunction, oral andwritten language,voice, flu-ency, speech articulation and myofunctional, orofacial, cervical,anddeglutitionsystems.32
In general, the assessed studies evaluated behavioral and neurocognitive functions; one study analyzed verbal fluency and academic performance. Thus, there were no studiesthatexclusivelyanalyzedorallanguage,butrather tried toeffectivelyunderstand languageat all levels.For theunderstandingoforallanguage,theabilitiesof Expres-siveandReceptiveLanguageshouldbeconsidered,thatis, thethoughtorganizationandexpressionprocessesthat,as well-organizedbehavior,can bedescribedby theaspects: phonological(inventoryofsoundsofalanguageandthe com-binationofrulestoformmeaningfulunits);syntactic(verbal production rules as a structure, taking into account the morphological and grammatical analysis);semantic (char-acterized by the lexical repertoire and related to the meaningof wordsandtheir combinations);andpragmatic (rules related to intentionality, context, and function of speech).33---36
Moreover,consideringthatthedevelopmentoflanguage occursgradually,respectingthechild’smaturationprocess andinfluencedbytheassociationsestablishedwiththe envi-ronmentwherethechildlives,32thehighvariabilityofthe agerangeofthesubjectsincludedinthestudiesanalyzedin thisreviewwasalimitingfactor,thispreventedcomparisons amongthestudies.Threestudiesassessedchildrenyounger than6years,27,29,30oneassessedchildrenaged5---7years,25 anotherassessedchildrenaged6---13years,26andonestudy assessedadolescents.28
The development of language is characterized by the presence ofsome markers,one of whichis age from4to 7 years,when the child graduallystarts toproduce more complexsounds,startingwiththeappropriateproductionof simplerwordsprogressingtolongerwords.35Regardingthe samplesassessedinthestudies,themaximumageof7years wasobservedinfourofthem,andtheothertwoconsidered childrenthatwereolderthantheexpectedageforthe sta-bilityofthephonologicalsystem.Althoughitisnotpossible toestablishassociationsbetweenthesamplesregardingthe phonologicaldevelopmentduetotheage range,it should benotedthattheperiodbetween3and7yearsisthepeak ofadenoidhypertrophyinchildrenwithOSA,37anditisalso whenmostspeechsoundsareacquired.35
The studies alsodifferregardingthe sleep characteris-tics,asthreeofthemanalyzedchildrenwithOSAassessed bypolysomnography(PSG),twoanalyzedchildrenwith pri-mary snoring, and one study did not include PSG among theirassessment methods, characterizingthe sampleonly throughquestionnaires.The definitionofOSA diagnosisby PSGanditsdegree,isnecessarytoallowforthecorrelation of changes in oral language with the evaluation of phys-iological impairment.38 Moreover, of the five studies that included PSG amongtheirassessment methods, the crite-ria/parametersutilizedtoconsiderOSAwerealsodifferent (withAHIrangingfrom>1to>10).Thus,itisdifficultto com-paretheincludedstudiesandconsidering thatallofthem hada cross-sectional design,their levelof evidenceis an intermediateone.
Regardingthemethodologyoflanguageanalysisthrough thedifferenttestsusedtoassess orallanguage(Kaufman, Peabody, Token, NEPSY, and an unspecified Greek test), itwas notpossible toperforma more thorough compari-sonoftheoutcomes,suggestingtheneed forstudies with thestandardizationoftheseprotocols,toprovideabetter understandingofthecorrelationbetweenOSAandoral lan-guage.However,despitetheabsenceof statisticalindices comparingtheresultsofthepresentinvestigation,thereis growingevidenceoforallanguageimpairmentinOSAcases. Among the oral language levels, the results of the aforementioned studies showed difficulties in the seman-tic,phonological,andverbalfluency levels.Someauthors havetriedtoexplainhowtheneurocognitiveperformance of children may be affected by sleep alterations. Fur-thermore, it has been stated that language deficits and verbalfluency can beexplained by thecumulative effect of sleep architecture disruptionassociated with the neu-rologicalmaturationperiod,whichover aperiodof afew yearsinterfereswiththedevelopmentofneuronalsynaptic networks,occurringrapidlyandintensivelyinchildren.19,39 Verbalfluency deficits arealsoassociated withprefrontal cortexdysfunction.40,41
Therefore, the early diagnosis and treatment of OSA should be emphasized, not only because of the possible implications for oral language, as demonstrated in the reviewedstudies,whichtendtoworsenasthechronological ageincreases,27 butalsoforthebenefitsinneurocognitive performanceandqualityoflifeofthesechildren.18,42---44
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.AmericanAcademyofSleepMedicine.TheAASMmanualforthe scoringofsleepandassociatedevents:rules,terminologyand technicalspecifications.1sted.Westchester:Illinois;2007.
2.KatzES,D’AmbrosioCM.Pediatricobstructivesleepapnea syn-drome.ClinChestMed.2010;31:221---34.
3.Marcus CL. Pathophysiology of childhood obstructive sleep apnea:currentconcepts.RespPhysiol.2000;119:143---54.
4.American Academy of Pediatrics. Clinical practice guideline diagnosisandmanagementofchildhoodobstructivesleepapnea syndrome.Pediatrics.2002;109:704---12.
5.MarcusCL,BrooksLJ,DraperKA,GozalD,HalbowerAC,Jones J,et al.Diagnosisand managementofchildhoodobstructive sleepapneasyndrome.Pediatrics.2012;130:1---9.
6.MarcusCL,MooreRH, RosenCL,GiordaniB, GaretzSL, Tay-lor HG, et al. A randomized trialof adenotonsillectomy for childhoodsleepapnea.NEnglJMed.2013;368:2366---76.
7.AmericanThoracic Society.Cardiorespiratorysleep studiesin children.AmJRespirCritCareMed.1999;160:1381---7.
8.BrunettiL,RanaS,LospallutiML,PietrafesaA,FrancavillaR, Fanelli M,et al. Prevalence of obstructive sleep apnea syn-drome ina cohortof1207children ofsouthernItaly.Chest. 2001;120:1930---5.
104 CorrêaCCetal.
10.BixlerEO,VgontzasAN,LinHM,LiaoD,CalhounS,Vela-BuenoA, etal.Sleepdisorderedbreathinginchildreninageneral popula-tionsample:prevalenceandriskfactors.Sleep.2009;32:731---6.
11.ZorziJL.Aintervenc¸ãofonoaudiológicanasalterac¸õesde lin-guageminfantil.RiodeJaneiro:Revinter;2002.
12.Nelson HD, Nygren P, Walker M, Panoscha R. Screening for speechand languagedelay inpreschool children:systematic evidencereviewfortheUSPreventiveServicesTaskForce. Pedi-atrics.2006;117:298---310.
13.OliveiraCEN,SalinaME,AnnunciatoNF.Fatoresambientaisque influenciamaplasticidadedoSNC.ActaFisiátrica.2001;8:6---13.
14.Anderson V, Spencer-Smith M, Wood A. Do children really recoverbetter? Neurobehavioural plasticity afterearly brain insult.Brain.2011;134:2197---221.
15.Owens J, Spirito A, Marcotte A, McGuinn M, Berkelhammer L.Neuropsychologicalandbehavioralcorrelatesofobstructive sleepapneasyndrome inchildren:apreliminary study.Sleep Breath.2000;4:67---78.
16.BlundenS,LushingtonK,KennedyD,MartinJ,DawsonD. Behav-iorandneurocognitiveperformanceinchildrenaged5---10years who snore compared to controls. J Clin Exp Neuropsychol. 2000;22:554---68.
17.KennedyJD,BlundenS,HirteC,ParsonsDW,MartinAJ,Crowe E,etal.Reducedneurocognitioninchildrenwhosnore.Pediatr Pulmonol.2004;37:330---7.
18.GozalD.Sleep-disorderedbreathingandschoolperformancein children.Pediatrics.1998;1023Pt1:616---20.
19.BeebeDW,GozalD.Obstructivesleepapneaandtheprefrontal cortex:towardsacomprehensivemodellinkingnocturnalupper airwayobstructiontodaytimecognitiveandbehavioraldeficits. JSleepRes.2002;11:1---16.
20.Uema SFH, Pignatari SSN, Fujita RR, Moreira GA, Pradella-Hallinan M, Weckx L. Avaliac¸ão da func¸ão cognitiva da aprendizagememcrianc¸ascomdistúrbiosobstrutivosdosono. RevBrasOtorrinolaringol.2007;73:315---20.
21.FeldmanHM,CampbellTF,Kurs-LaskyM,Rockette.Concurrent andpredictive validityofparentreportsofchildlanguageat ages2and3years.ChildDev.2005;76:856---68.
22.Rondal JA, Esperet E, Gombert JE, Thibaut JP, Comblain A. Desenvolvimentodalinguagemoral.In:PuyueloM,RondalJA, editors.Manualdedesenvolvimentoealterac¸õesdalinguagem nacrianc¸aenoadulto.SãoPaulo:Artmed;2007.p.17---86.
23.SmeekensS, Riksen-Walraven JM,vanBakel HJA. Profilesof competenceandadaptationinpreschoolersasrelatedtothe qualityofparent---childinteraction.JResPers.2008;42:1490---9.
24.GurgelLG,PlentzRDM,JolyMCRA,ReppoldCT. Instrumentos deavaliac¸ãodacompreensãodelinguagemoralemcrianc¸ase adolescentes:umarevisãosistemáticadaliteratura.Rev Neu-ropsicolLatinoamericana.2010;2:1---10.
25.O’Brien LM, Mervis CB, Holbrook CR, Bruner JL, Klaus CJ, RutherfordJ,et al.Neurobehavioralimplicationsofhabitual snoringinchildren.Pediatrics.2004;114:44---9.
26.KurnatowskiP,Puty´nskiL,LapienisM,KowalskaB. Neurocogni-tiveabilitiesinchildrenwithadenotonsillarhypertrophy.IntJ PediatrOtorhinolaryngol.2006;70:419---24.
27.AndreouG, AgapitouP.Reduced languageabilitiesin adoles-centswhosnore.ArchClinNeuropsychol.2007;22:225---9.
28.LandauYE,Bar-YishayGreenberg-DotanS,GoldbartAD, Tara-siukA,TalA.Impairedbehavioralandneurocognitivefunction inpreschoolchildrenwithobstructivesleepapnea.Pediatr Pul-monol.2012;47:180---8.
29.LiukkonenK, Virkkula P, HaavistoA, Suomalainen A, Aronen ET,PitkärantaA,etal.Symptomsatpresentationinchildren withsleep-related disorders. Int JPediatr Otorhinolaryngol. 2012;76:327---33.
30.YorbikO,MutluC,KocD,MutluerT.Possiblenegativeeffects ofsnoringandincreasedsleepfragmentationondevelopmental statusofpreschoolchildren.SleepBiolRhythms.2014;12:30---6.
31.ValeraFCP,DemarcoRC,Anselmo-LimaWT.Síndromedaapnéia edahipopnéiaobstrutivasdosono(SAHOS)emcrianc¸as.Rev BrasOtorrinolaringol.2004;70:232---7.
32.Conselho Federal de Fonoaudiologia. Exercício profissional
do fonoaudiólogo 2002. Brasília (DF): CFF; 2002. [cited 21
Mar2015].Availablefrom:http://www.fonoaudiologia.org.br/
publicacoes/epdo1.pdf
33.HageSRV,ResegueMM,ViveirosDCS,PachecoEF.Análisedo per-fildashabilidadespragmáticasemcrianc¸aspequenasnormais. Pró-FonoRevAtualizac¸ãoCientífica.2007;19:49---58.
34.BooneDR,PlanteE.Acomunicac¸ãohumanaeseusdistúrbios. PortoAlegre:ArtesMédicas;1983.
35.WertznerHF.Fonologia:desenvolvimentoealterac¸ões.In: Fer-reira LP, Befi-Lopes DM, Limongi SCO, editors. Tratado de Fonoaudiologia.1stedSãoPaulo:Roca;2004.p.772---86.
36.PenningtonBF,BishopDV.Relationsamongspeech,language, andreadingdisorders.RevPsychol.2009;60:283---306.
37.GreenfeldM,TaumanR,DeRoweA,SivanY.Obstructivesleep apneasyndromeduetoadenotonsillarhypertrophyininfants. IntJPediatrOtorhinolaryngol.2003;67:1055---60.
38.RyanCM,BradleyTD.Pathogenesisofobstructivesleepapnea. JApplPhysiol.2005;99:2440---50.
39.O’BrienLM,GozalD.Behavioralandneurocognitiveimplications ofsnoring andobstructivesleepapneainchildren:factsand theory.PediatricRespirRev.2002;3:3---9.
40.Desmond J, Fiez J. Neuroimaging studies of the cerebel-lum:language,learningandmemory.TrendsCognSci.1998;2: 355---62.
41.JanowskiJS,ShimamuraAP,SquireLR.Sourcememory impair-mentinpatientswithfrontallobelesions. Neuropsychologia. 1989;27:1043---56.
42.Goldstein NA, Post JC, Rosenfeld RM, Campbell TF. Impact oftonsillectomy and adenoidectomyon child behavior. Arch OtolaryngolHeadNeckSurg.2000;126:494---9.
43.FriedmanBC,Hendeles-AmitaiA, KozminskyE,LeibermanA, FrigerM,TarasiukA,etal.Adenotonsillectomyimproves neu-rocognitivefunctioninchildrenwithobstructivesleep apnea syndrome.Sleep.2003;26:999---1005.