www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Obstructive
sleep
apnea
in
postmenopausal
women:
a
comparative
study
using
drug
induced
sleep
endoscopy
夽
Soo
Kweon
Koo
a,∗,
Gun
Young
Ahn
b,
Jang
Won
Choi
a,
Young
Jun
Kim
a,
Sung
Hoon
Jung
a,
Ji
Seung
Moon
a,
Young
Il
Lee
caBusanSaintMary’sHospital,DepartmentofOtorhinolaryngology,Busan,SouthKorea bUlsanHanaENTHospital,Ulsan,SouthKorea
cGoodSamsunHospital,DepartmentofOccupationalandEnvironmentalMedicine,Busan,SouthKorea
Received2December2015;accepted23March2016 Availableonline25April2016
KEYWORDS Sleepapnea syndrome; Endoscopy; Gender; Menopause
Abstract
Introduction:ThekeytosuccessfultreatmentofOSASistoindividuallytailorsuchtreatment. Thus,itisveryimportanttodeterminetheseverity ofOSAS,itspattern,andtheextentof collapse,bygender,age,andBMI.
Objective: Theobjectiveofthestudywastounderstandthecharacteristicsofobstructivesleep apneainpostmenopausalwomenbycomparingpostmenopausalandpremenopausalsubjects, andmen,usingDISE.Wehopethatourworkwillhelpthemedicalcommunitytoconsulton, diagnose,andtreatOSASmoreeffectively.
Methods:A total of 273 patients (195 males and 78 females) diagnosed with OSAS were enrolled. Female patients were divided into pre-menopausal (n=41) and post-menopausal patients(n=37).Thegroupofpost-menopausalfemalepatientswasmatchedwithagroupof malepatientswithsimilarageandbodymassindex(BMI).DISEfindingswerecomparedbetween pre-menopausalfemalepatientsandpost-menopausalfemalepatients,andalsobetween post-menopausalfemalepatientsandmalepatientsmatchedforageandBMI.
Results:UponPSGexamination,post-menopausalpatients(whohadasignificantlyhigherBMI thandidpre-menopausalpatients;25.6kg/m2vs.23.5kg/m2;p=0.019)tendedtohaveahigher
AHIandalowerlowestSaO2,butthedifferencesdidnotattainstatisticalsignificance.With
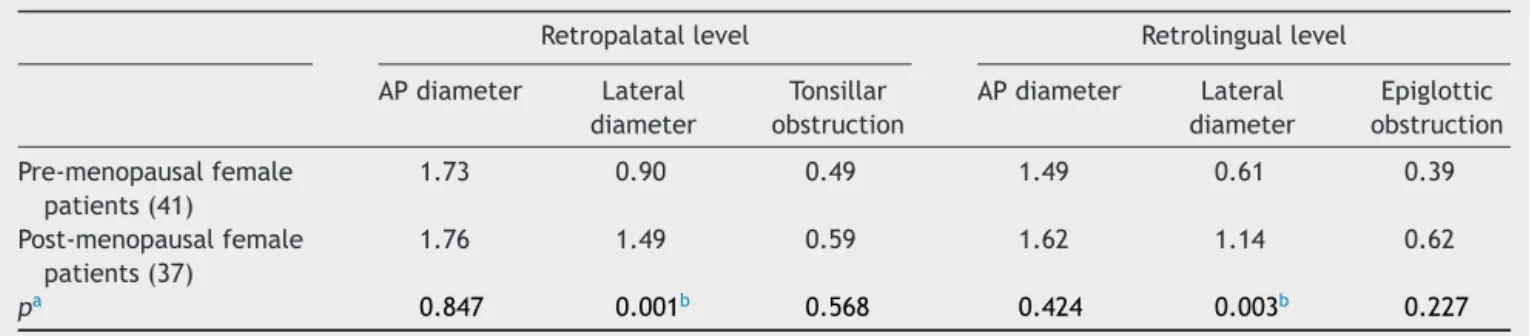
DISEanalysis,post-menopausalfemalepatientsshowedhighervaluesinallobstructionsites, withsignificantlyhighervalueinlateraldiameterofretropalatal(1.49vs.0.90;p=0.001)and retrolinguallevels(1.14vs.0.61;p=0.003)comparedtopre-menopausalfemalespatients. Post-menopausalfemalepatientsshowedsignificantlymoreretrolingualcollapse(antero-posterior,
夽 Pleasecitethisarticleas:KooSK,AhnGY,ChoiJW,KimYJ,JungSH,MoonJS,etal.Obstructivesleepapneainpostmenopausalwomen:
acomparativestudyusingdruginducedsleependoscopy.BrazJOtorhinolaryngol.2017;83:285---91.
∗Correspondingauthor.
E-mail:[email protected](S.K.Koo).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.03.011
AP,p≤0.0001, andlateral diameter,p=0.042) inthelower BMIgroup (BMI<25)and more concentricretropalatalcollapse(lateraldiameter,p=0.017andtonsillarobstruction,p=0.003) inhigherBMIgroup(BMI≥25)thanBMIandagematchedmalepatients.
Conclusion:Post-menopausalfemalepatientsshowedadifferentpatternofairwayobstruction comparedtopre-menopausalfemalepatientsandmalepatientsmatchedforageandBMIbased onDISEfindings.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Síndromedaapneia dosono;
Endoscopia; Gênero; Menopausa
Apneiaobstrutivadosonoemmulheresnapós-menopausa:estudocomparativo usandoendoscopiadosonoinduzidoporfármaco
Resumo
Introduc¸ão:Achaveparaosucessodotratamentodasíndromedaapneiaobstrutivadosono (SAOS)éadaptarindividualmenteessetratamento.Assim,émuitoimportantedeterminara gravidadedaSAOS,seupadrãoeamedidadocolapso,porsexo,idadeeIMC.
Objetivo:O objetivo doestudo foicompreender ascaracterísticas daapneia obstrutiva do sonoemmulheresnapós-menopausa,comparandoestascaracterísticasentremulheresna pós-menopausaepré-menopausa,ehomens,utilizandoendoscopiadosonoinduzidoporfármacos (DISE).Esperamos queonossoestudoajude acomunidademédicaadiagnosticaretratara SAOSdemaneiramaiseficaz.
Método: Foramrecrutados273pacientes(195dosexomasculinoe78dofeminino)com diag-nósticodeSAOS.Aspacientesdosexofemininoforamdivididasempacientesnapré-menopausa (n=41)enapós-menopausa(n=37).Ogrupodepacientesdosexofemininonapós-menopausa foipareadacomumgrupodepacientesdosexomasculinocomidadeeÍndicedeMassaCorporal (IMC)semelhantes.OsachadosdaDISEforamcomparadosentreaspacientesdosexofeminino napré-menopausaeaspacientesdosexofemininopós-menopausaetambémentrepacientes dosexofemininonapós-menopausaepacientesdosexomasculinopareadosporidadeeIMC.
Resultados: AoexamedePSG,aspacientesnapós-menopausa(quetinhamumIMC significativa-mentemaiordoqueaspacientesnapré-menopausa;25,6vs23,5kg/m2;p=0,019)tenderama
terumIAHsuperioreumasaturac¸ãoarterialdeoxigênio(SaO2)mínimamenor,masasdiferenc¸as
não atingiram significânciaestatística.NaanálisedoDISE, pacientesdosexo feminino pós-menopausaapresentaramvaloresmaiselevadosemtodososlocaisdeobstruc¸ão,comumvalor significativamentemaiordediâmetrolateraldosníveisretropalatal(1,49vs.0,90;p=0,001) eretrolingual(1,14 vs.0,61; p=0,003)emcomparac¸ão compacientesdo sexofemininona pré-menopausa.Aspacientesdosexofemininonapós-menopausaapresentaramcolapso signi-ficativamentemaisretrolingual(anteroposterior,AP,p≤0,0001ediâmetrolateral,p=0,042) nogrupodeIMCmenor(IMC<25)ecolapsoretropalatalmaisconcêntrico(diâmetro lateral,
p=0,017eobstruc¸ãotonsilar,p=0,003)nogrupodemaiorIMC(IMC≥25)doquepacientesdo
sexomasculinopareadosporIMCeidade.
Conclusão:CombasenosachadosdoDISE,aspacientesdosexofemininonapós-menopausa apresentaram umpadrão diferentede obstruc¸ão dasviasrespiratóriasemcomparac¸ãocom pacientesdosexofemininonapré-menopausaecomospacientesdosexomasculinopareados poridadeeIMC.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Severalpopulationbasedstudies acrossvarious geographi-calregionsandethnicgroupshavereportedtheprevalence ofsleepdisorderedbreathing(SDB)fromobstructivesleep apneasyndrome(OSAS).OSASisadiseasethatisrelatively morecommoninmenthanwomen,especiallymiddle-aged men.1Andaccordingtovariousstudies,incidenceofOSASin
womenincreasesaftermenopause.1,2Thusbesidesgender differences,incidenceofOSASmaybeduetotheinfluence ofhormones changingwithage,racialmakeupand differ-encesindiet.
according togender andage,determination ofthe sever-ityofOSAS,patternanddegreeofairwaycollapsearevery importantinindividuallytailoringatreatment.A compara-tivestudyofOSASbetweenmenandwomenbasedonthe naturalphysiologicsleepstateofthesubjectshasnotbeen conductedyet.Sleepnasoendoscopyordruginducedsleep endoscopy(DISE), firstintroducedbyCroftandPringle3in 1991, is a procedure that uses a flexible nasoendoscope tovisualize the upperairway undersedation. DISE evalu-atesthelocalizationofflutterandcollapseinpatientswith SDB.SeveralcentersarenowavailablethatperformDISEis nowavailableinmultiplesleepstudyclinics.AlthoughDISE hassomelimitationssuchaslimitedperiodof observation andmultiple classificationsystems,it addressesthe natu-ralphysiologicstateofsleepmorethananyothercurrently availablediagnostictool.4
The keyto successfultreatment of OSAS is to individ-ually tailor suchtreatment. Thus, it is very important to determinetheseverityofOSAS,itspattern,andtheextent of collapse, by gender, age, and BMI; then it is possible toconstructa personalizedtreatment plan. Menopauseis associated withimportant physical andhormonal changes infemales,andthusmustbeconsideredwhentherapeutic approachesareplanned.Wesoughttounderstandthe char-acteristics of obstructive sleep apnea in postmenopausal women by comparingpostmenopausal andpremenopausal subjects,andmen,usingDISE.Wehopethatourworkwill help themedicalcommunitytoconsult on,diagnose, and treatOSASmoreeffectively.
Methods
Patientsselectionandoutcomeassessment
Theretrospectiveobservationalstudywasconductedatour ENTDepartmentwhereDISEwasperformedbyoneexaminer in273subjects(195males,meanage41.1yearsold;and78 females,meanage46.0yearsold)consecutiveOSASpatients from2013to2014.
BeforeDISE,allpatientsreceivedathoroughear,nose, andthroatexamination, focusingonnasalpathology, ton-sil size, uvula and palate aspect and tongue size. Their medicalhistorywastaken.Allpatientsunderwentfullnight polysomnography(PSG,WEE-1000K,NihonKohden,Japan). To minimize morphological bias, we excluded patients withskeletal frameworkanomalies such assevere retrog-nathia or jaw retrusion patients. In addition, to exclude bias introduced by tonsil size, we excluded patients with tonsils of grades III and IV. Patients who had undergone prior surgery of the soft palate or tongue were also excluded. Post-menopause was defined as a patient who did not have menstruation for more than a year and post-menopausal women receiving hormonal replacement therapywerealsoexcluded.Thefemalegroupsconsistedof 41pre-menopausal(meanage,36.7yearsold)and37 post-menopausalfemalepatients(meanage,56.3yearsold).All post-menopausal femalepatients were over 50 yearsold. Individuals with a BMI of 25---29.9 were considered over-weight,while individuals witha BMI 30 were categorized asobese.5 The matching limitswere 50yearsor olderfor age,and25kg/m2orhigherforBMIinourstudy.
According to these criteria, we compared DISE find-ingsbetweenpre-menopausalfemaleandpost-menopausal female patients or between post-menopausal female and malespatientsmatchedforage(over50yearsold)andBMI.
Druginducedsleependoscopyandclassification system
AllDISEprocedureswereperformedby thesameENT sur-geonin a semi-dark and silent operation roomwith each patient lying supine. Sleep was induced by intravenous administrationof midazolam with respiratory monitoring. Theanesthesiologistslowlytitratedthedrugto0.07mg/kg perpatient;bolusesof1---2.5mgweregiven(toamaximum of7.5mgperpatient)usingatarget-controlledinfusion sys-tem. An extra bolus was often required by patients who wereextremelynervous.Oncethepatientwasdeeplyasleep enough to snore, show obstructions and responded slug-gishtoalightglabellaorloudauditorystimulus(Ramsay’s levelofsedationscale5),6a4mm-diameterflexiblevideo laryngoscopewasgentlyintroducedthroughthenose.Video images of all DISE procedures were later evaluated by a singleotolaryngologist.
WeoftenperformedDISEpostoperativelytoobservethe extentof improvementaftersurgery; preoperative proce-dureswereprincipallydiagnosticinnature.
Each procedure took 20---30min. When possible, we performedonlyonecycle,aftercarefulpreparation,to min-imizetheriskofrespiratorycomplications.
We divided the pharynx into two portions: the retropalatal level (the region of posterior to the soft palate)andtheretrolinguallevel(the regionof the phar-ynx posterior to the vertical portion of the tongue). We madetheclassification systemaccording toourpublished procedures.4,7 Briefly, our classification system included the following: the obstruction site, degree of SDB, and the anatomical structure contributing the most to sleep apnea. The retropalatal level was subdivided into palate (antero-posterior diameter), lateral pharyngeal wall (lat-eraldiameter), and tonsil (specific structure contributing to obstruction). The retrolingual level was divided into tonguebase(antero-posteriordiameter),lateralpharyngeal wall (lateral diameter), and epiglottis (specific structure contributingtoobstruction). Degreeof airwayobstruction was categorized as no obstruction (rated as 0), partial obstruction(ratedas1;50---75%obstruction),andcomplete obstruction(ratedas2,>75%)(Table1).
Statisticalanalysis
We evaluated the difference between female and male patientgroups accordingtoDISEfindings. Student’st-test was used to compare BMI, AHI, and lowest arterial oxy-gensaturation (SaO2) betweenmaleand femalepatients. Mann---Whitney U test was used if the data was not nor-mallydistributed.Allstatisticaltestswereperformedusing SPSSversion 18.0 (SPSS Inc., Chicago IL, USA). Statistical significancewasmetwhenp-valuewaslessthan0.05.
Table1 DISEclassificationsystem.
Obstructionlevel Configurationa
APdiameter Lateraldiameter Contributingstructure
Retropalatal PalateAP LPW Tonsil
0/1/2 0/1/2 0/1/2
Retrolingual TonguebaseAP LPW Epiglottis
0/1/2 0/1/2 0/1/2
AP,anteroposterior.
aDegreeofobstructionhasonenumberforeachstructure:0,noobstruction(novibration);1,partialobstruction(vibration,50---75%); 2,completeobstruction(collapse,>75%).
AdaptedfromKooetal.7
Table2 Demographyandpatient’scharacteristicsofPSGfinding.
Sex Number Age(yr) BMI(kg/m2) AHI(events/h) LowestSaO 2(%)
Male 195 41.1 26.0 23.2 79.6
Female 78 46.0 24.5 13.9 83.2
pa 0.005c 0.001c 0.001c 0.026c
Female
Pre-menopausalfemalepatients 41 36.7 23.5 12.8 85.0
Post-menopausalfemalepatients 37 56.3 25.6 15.0 81.2
pb <0.0001c 0.019c 0.630 0.130
PSG,polysomnography;BMI,bodymassindex;AHI,apnea/hypopneaindex;SaO2,arterialoxygensaturation. aStudent’st-testbetweenmaleandfemale.
b Student’st-testbetweenpre-menopausalandpost-menopausalfemalepatients.
c Statisticallysignificantdifferencesbetweengroupsregardingage,BMI,AHIandlowestSaO 2.
Results
Demography of patients used in this study is summarized inTable 2. Total273 subjects (195males, meanage 41.1 years old; and 78 females, mean age 46.0 years old). Male patients had significantly higher BMI (26.0 vs. 24.5;
p=0.001),higherAHI (23.2vs.13.9;p=0.001),andlower lowest SaO2 (79.6 vs. 83.2; p=0.026). The average ages of pre-menopausal and post-menopausal female patients
were 36.7 and 56.3years, respectively. Upon PSG exami-nation, post-menopausalpatients (whohad a significantly higher BMI than did pre-menopausal patients; 25.6kg/m2 vs.23.5kg/m2;p=0.019)tendedtohaveahigherAHIand alowerlowestSaO2,butthedifferencesdidnotattain sta-tisticalsignificance(Table2).
Comparisons between pre-menopausal and post-menopausal female patients accordingto DISEfindingare summarized in Table 3. In DISE finding, post-menopausal
Table3 ComparisonofDISEscorebetweenpre-menopausalandpost-menopausalfemalepatients.
Retropalatallevel Retrolinguallevel
APdiameter Lateral diameter
Tonsillar obstruction
APdiameter Lateral diameter
Epiglottic obstruction
Pre-menopausalfemale patients(41)
1.73 0.90 0.49 1.49 0.61 0.39
Post-menopausalfemale patients(37)
1.76 1.49 0.59 1.62 1.14 0.62
pa 0.847 0.001b 0.568 0.424 0.003b 0.227
(),numberofpatients;DISE,drug-inducedsleependoscopy;AP,anteroposterior. aStudent’st-test.
Table4 ComparisonofDISEscorebetweenpost-menopausalfemalepatients(BMI<25)andmen(age≥50;BMI<25).
Retropalatallevel Retrolinguallevel
APdiameter Lateral diameter
Tonsillar obstruction
APdiameter Lateral diameter
Epiglottic obstruction
Men(26) 1.81 0.88 0.31 0.85 0.81 0.62
Post-menopausalfemale patients(17)
1.88 1.24 0.35 1.76 1.24 0.71
pa 0.710 0.166 0.935 <0.0001b 0.042b 0.716
(),numberofpatients;DISE,drug-inducedsleependoscopy;AP,anteroposterior. a Mann---Whitneytest.
b Statisticallysignificantdifferencesbetweengroups.
Table5 ComparisonofDISEscorebetweenpost-menopausalfemalepatients(BMI≥25)andmen(age≥50;BMI≥25).
Retropalatallevel Retrolinguallevel
APdiameter Lateral diameter
Tonsillar obstruction
APdiameter Lateral diameter
Epiglottic obstruction
Men(31) 1.68 1.19 0.16 1.10 0.87 0.52
Post-menopausalfemale patients(20)
1.65 1.70 0.80 1.50 1.05 0.55
pa 0.882 0.017b 0.003b 0.057 0.461 1.000
(),numberofpatients;DISE,drug-inducedsleependoscopy;AP,anteroposterior. a Mann---Whitneytest.
b Statisticallysignificantdifferencesbetweengroups.
femalepatientsshowedhighervaluesinalltheobstruction sites.Significantdifferencewasseenforbothlateral diame-terofretropalatal(0.90vs.1.49;p=0.001)andretrolingual levelmeasures(0.61vs.1.14;p=0.003)(Table3).
IncomparisontoDISEfindingbetweenpost-menopausal femalepatients(n=37)andmalepatientsmatchedforage (over 50 years old) and BMI, the total number of male patients was 195, of these, 26 and 31 were matched for age(over50years)andBMI(BMI<25kg/m2),andage(over 50 years) and BMI (BMI≥25kg/m2), with females.
Post-menopausalfemalepatientshadsignificantlyhighervalues inAP(p<0.0001)andlateraldiameterofretrolinguallevel (p=0.042)inlowerBMIgroup(BMI<25)(Table4).Inhigher BMIgroup(BMI≥25),post-menopausalfemalepatientshad
significantly higher values in lateral diameter (p=0.017) and tonsillar obstruction (p=0.003) of retropalatal level (Table5).
Discussion
OSAS is generally more common and severe in men and than women when matched for BMI and PSG parameters suchasAHIandlowestSaO2saturation.1Thesefindingsare in agreement with our resultand previous reports in the literature about sleep apnea patients of different ethnic origins.8---10 However, women experience hormone-related changessuchasmenopauseandpregnancythathaveagreat
influenceonincidenceOSAS.Therefore,genderdifferences areveryimportantinexamination andtreatmentof sleep disorders.
OSASgenerallyoccursmore frequentlyandwithhigher severityinpost-menopausal femalesthan pre-menopausal females aspre-menopausal females have higher levels of circulatingprogesteronethatcouldpreventairwayclosure by reducing the collapsibility of genioglossus muscle.10---15 Other than that the reasons behind influence of gender andthe menopause status for females in occurrence and severity of OSAS are still not completely understood. It hasbeen estimated that the prevalence of this condition among women in their sixth or seventh decade of life rangesfrom4%to22%dependingonthedefinitionusedand thepopulation examined.11 Inourstudy,post-menopausal femalepatientswithOSAShadasignificantlyhighervalueof BMI,higherAHIandlowerlowestSaO2saturation,although the differences were not statistically significant. There-fore,post-menopausalfemalepatientstendedtoshowmore severeOSASthanpre-menopausalfemalepatients.Although noclear causes for thesechanges have been established, theageparametersformenopausalstatusandupperairway muscletonemighthavecontributed.
thelateralwalloftheairwayobstructionplaysasignificant roleforwomenaftermenopause.Thisisanimportantpoint fromthe therapeutic point of view. Other research stud-iesfrom DISE finding of obstructive sleep apnea patients showedsimilarresults,emphasizingtheimportanceofthe lateraldiameter.4,16,17InthecurrentstudyfromDISE analy-sis,multileveland complete collapse wasmore prevalent in obese patients and in those with more severe OSA. Higher BMIvalueswere associated ahigher probabilityof complete concentric palatal collapse and also complete lateral hypopharyngeal collapse, which may be explained byfat accumulationat the lateral pharyngeal walls.16 On thecontrary, lowerBMIvalue wasassociated withtongue base collapse,and thismay beresultof less fat accumu-lationinthelateralpharyngeal wall,possiblyallowing for more backward movement of the tongue.16 In our study, post-menopausalfemalepatientsshowedmore concentric palatalcollapse(lateraldiameterandtonsillarobstruction ofretropalatal level) inhigherBMI groupand retrolingual collapse(AP and lateraldiameterof retrolinguallevel) in lower BMI group than male patients, and our result is in agreement with previous reports. These findings indicate that post-menopausal female patients have a higher ten-dencyofanatomicalchangeintheairwaythanmenofthe sameagegroupandlevelofobesity.Therefore,weshould pay more attention to anatomical changes when treating post-menopausalfemaleOSASpatients.
In general, a large upper airway soft tissuevolume in menmaycontributetoincreasedprevalenceofOSAS com-paredtowomen.Upperairwayresistanceisreportedtobe higherinmenthanthatinwomen.17,18But,post-menopausal femalepatientsshowed moresevereclosure in ourstudy. Thismightbeduetothefactthatthemuscletoneof post-menopausalwomenisdecreased.However,furtherresearch isrequiredtoexplorethispossibility.
Ourstudyhassomelimitations.Thestudypopulationwas smallthusreducingthepowerofanalysis.Alsothepatients ofthis study werecandidates for obstructivesleepapnea surgery,sodidnotrepresentthegeneralOSASpopulation.As aresult,therewasaninherentbiasfordrugselection, pro-cedure,andclassificationfromDISE.Alarge-scalestudyof thegeneralOSASpopulationisrequired,asitwouldobviate thistreatmentbias.
Conclusion
In conclusion, post-menopausal female patients showed more severe sleep apnea than pre-menopausal female patients.InDISEfindings,post-menopausalfemalepatients showed a tendency with a more severe airway obstruc-tion,especiallyinthelateralwall.Post-menopausalfemale patientsshowedmoreconcentricpalatalcollapseinhigher BMIgroupandretrolingualcollapseinlowerBMIgroupthan themalepatients.Post-menopausalfemalepatientsshowed atendencywithmoresevereairwayobstructioninallparts oftheairwayinDISEfindingthanmenwithsimilarageand BMI. The key to successfully treating OSAS is individually tailoredtreatment.Inthisrespect,determiningthe sever-ity of OSAS, pattern and degree of collapse according to gender,ageandBMIareveryimportantforapersonalized
treatmentplan.Therefore,withinsomelimits,our compar-ativestudybetweenmenandwomenthroughDISEmayhelp themedicalcommunityconsult, diagnose,andtreat OSAS moreeffectively.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.PeppardTE,YoungT,BarnetJH,PaltaM,HagenEW,HlaKM. Increasedprevalenceofsleep-disorderedbreathinginadults. AmJEpidemiol.2013;177:1006---14.
2.YoungT,PaltaM,DempseyJ,SkatrudJ,WeberS,BardS.The occurrenceofsleepdisorderedbreathingamongmiddle-aged adults.NEnglJMED.1993;328:1230---5.
3.CroftCB,PringleM.Sleepnasoendoscopy:atechniqueof assess-mentinsnoringandobstructivesleepapnoea.ClinOtolaryngol AlliedSci.1991;16:504---9.
4.De Vito A, Carrasco Llatas M, Vanni A, Bosi M, Braghiroli A, Campanini A, et al. European position paper on drug-induced sedation endoscopy (DISE). Sleep Breath. 2014;18: 453---65.
5.Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999---2008. JAMA. 2010;303:235---41.
6.Hernández-Gancedo C, Pesta˜na D, Pe˜na N, Royo C, Pérez-ChrzanowskaH,CriadoA.Monitoringsedationincriticallyill patients:bispectralindex,Ramsayandobserverscales.EurJ Anaesthesiol.2006;23:649---53.
7.Koo SK, ChoiJW, Myung NS,Lee HJ, KimYJ, KimYJ. Anal-ysisof obstructionsite in obstructive sleepapnea syndrome patientsbydruginducedsleependoscopy.AmJOtolaryngol. 2013;34:626---30.
8.Wahner-RoedlerDL,OlsonEJ,NarayananS,SoodR,HansonAC, LoehrerLL,etal.Gender-specificdifferencesinapatient popu-lationwithobstructivesleepapnea---hypopneasyndrome.Gend Med.2007;4:329---38.
9.Ip MS, Lam B, Tang LC,Lauder IJ, Ip TY, Lam WK. A com-munity study of sleep-disordered breathing in middle-aged Chinesewomen inHongKong:prevalenceandgender differ-ences.Chest.2004;125:127---34.
10.VagiakisE,KapsimalisF,LagogianniI,PerrakiH,Minaritzoqlou A,AlexandropoulouK,etal.Genderdifferenceson polysomno-graphicfindingsinGreeksubjectswithobstructivesleepapnea syndrome.SleepMed.2006;7:424---30.
11.Bixler EO, Vgontzas AN, Lin HM, Ten Have T, Lein J, Vela-BuenoA, et al. Prevalence of sleep-disordered breathing in women:effectsofgender.AmJRespirCritCareMed.2001;163: 608---13.
12.DanceyDR,HanlyPJ,SoongC,LeeB,ShepardJJr,HoffsteinV. Impactofmenopauseontheprevalenceandseverityofsleep apnea.Chest.2001;120:151---5.
13.PopovicRM, White DP. Upper airway muscle activity in nor-mal women: influence of hormonal status. J Appl Physiol. 1998;84:1055---62.
14.LeiterJC,DobleEA,KnuthSL,BartlettDJr.Respiratoryactivity ofgenioglossus.Interactionbetweenalcoholandthemenstrual cycle.AmRevRespirDis.1987;135:383---6.
16.VroegopAV,VandervekenOM,BoudewynsAN,ScholmanJ, Sal-dien V, Wouters K, et al. Drug-induced sleep endoscopy in sleep-disordered breathing: report on 1,249 cases. Laryngo-scope.2014;124:797---802.
17.RaveslootMJ,deVries N.One hundredconsecutive patients undergoingdrug-inducedsleependoscopy:resultsand evalua-tion.Laryngoscope.2011;121:2710---6.