REVIEW
1. Departamento de Clínica e Odontologia Preventiva, Universidade Federal de Pernambuco, Recife, PE, Brazil
2. Oral Medicine unit, Division of Maxillofacial Diagnostics, Surgical and Medical Sciences, Eastman Dental Institute for Oral Health Care Sciences, University of London, UK
Email: [email protected]
Received for publication on June 12, 2007 Accepted for publication on August 27, 2007
ULCERATIVE LESIONS OF THE MOUTH: AN UPDATE
FOR THE GENERAL MEDICAL PRACTITIONER
Jair Carneiro Leão1, Valder Barbosa Gomes1,Stephen Porter2
Leão JC, GomesVB, Porter S. Ulcerative lesions of the mouth: an update for the general medical practitioner. Clinics.
2007;62(6):769-80.
Oral ulceration is a common complaint of patients attending out-patient clinics. Because of the diversity in causes of oral ulceration, patients presenting with oral mucosal disease can be challenging to diagnose and manage. Patients with signs or symptoms of oral ulcers are sometimes referred to gastroenterology clinics; however, in most instances the ulcers do not result from gastrointestinal disease. The aim of the present article is to review aspects of the etiology, diagnosis and management of common ulcerative disorders of the oral mucosa. A search in the National Library of Medicine computerized bibliographic database MEDLINE was performed. Selection of publications, extraction of data, and validity assessment were then performed by the authors. Based upon the searched literature, it is concluded that there are several systemic disorders that can present with similar clinical signs and symptoms, and knowledge of each disease is necessary for the clinician to provide proper management.
KEYWORDS Oral Ulceration. Oral Medicine. Oral Lesions. Recurrent Aphthous Stomatitis. Recurrent Oral Ulceration.
INTRODUCTION
Oral ulcers are one of the most common complaints of the oral mucosa. The term ulcer is used where there is dam-age to both the epithelium and lamina propria. Several pre-disposing factors have been suggested and oral ulcers can be a feature of various systemic disorders including inflam-matory bowel disease. Oral ulcers are determined by the underlying systemic condition such as the nature, site, du-ration and frequency. In addition, histopathological exami-nation usually produces a definitive diagnosis for the ma-jority of conditions described in this paper. The aim of this review is to provide a focus on ulcerative disorders, either of general clinical significance, or relevant to gastroen-terology.
Oral ulcers of traumatic (physical and chemical) etiology
The majority of cases of ulcers of the oral mucosa are due to physical trauma. However, chemical trauma must also be considered. Salicylic acid (aspirin) and its deriva-tives are extensively used for the treatment of systemic and local diseases. However, injudicious use of these com-pounds may cause systemic and oral complications, such as mucosal burns and oral ulcers.1 In addition, ulcers may
arise (e.g. on the palate)2 with the use of powdered cocaine
or through the smoking crack cocaine. The effects of co-caine in the oral cavity vary depending on the form used and the route of administration. Rarely, snorting cocaine may cause necrosis, possibly associated with ischemia, of the floor of the nose; and eventually causing ulcers of the hard palate as well as oronasal fistula formation.3
Oral ulcers can be caused by local radiotherapy and some cytotoxic chemotherapy regimes (mucositis) (Fig.1). The mucosistis manifests as multiple areas of painful mu-cosal erythema, ulcers and sloughing.4 The precise etiology
a loss of basal cell proliferation5 rather than a reaction to
changes in the local oral microflora (e.g. increases in Gram-negative bacteria, particularly Enterobacteriaceae).6 This
mucositis, akin to that of the bowel, is difficult to manage specifically. Benzydamine hydrochloride mouth rinse or spray may provide symptomatic relief, but effective anal-gesia often requires opioids. The clinical features of oral mucositis do not significantly improve with topical chlorhexidine gluconate, although this compound is com-monly used in clinical practice. Novel regimes for the treat-ment of mucositis include granulocyte-macrophage colony-stimulating factor (GM-CSF) and protegrins.7, 8
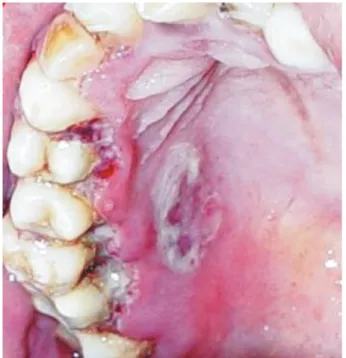
Necrotizing sialometaplasia
Necrotizing sialometaplasia is an uncommon disorder that typically gives rise to large areas of deep ulcers on one side of the hard and/or soft palate.9 This condition is
con-sidered to be associated with an ischemic event, and is as-sociated with clinical factors such as smoking, alcohol use, denture wearing, recent surgery, systemic disease, and it can also be a feature of bulimia nervosa.10 It has been
sug-gested that the local traumas mentioned above cause ischemia with resultant tissue necrosis. The clinical features may mimic those of squamous cell carcinoma (SCC), and histopathologically, the profound epithelial hyperplasia, together with the salivary gland squamous metaplasia seen with necrotizing sialometaplasia, can be confused with neo-plasia.
Viral diseases
Herpes simplex virus 1
The most common viral precipitant of ulcers is herpes simplex virus type 1 (HSV 1). Affected individuals may
have widespread, small, superficial ulcers of the oral mu-cosa (Fig. 2). The gingiva are often swollen and ulcerated, giving rise to features akin to acute necrotizing ulcerative gingivitis (ANUG). While previously regarded as a disease of childhood, primary HSV-1 infection often arises in the second or third decade of life.11 Severe and/or recurrent
HSV-1 infection, sometimes presenting atypically, may be suggestive of underlying immunodeficiency, in particular lymphoproliferative disease or HIV disease.12
About 5% of patients who have a primary HSV-1 infec-tion will develop recurrent episodes of herpes labialis (cold sores), as illustrated in Figure 3. This comprises episodes of paresthesia, erythema, vesiculation, pustulization, and ulcers at the mucocutaneous junctions of the lips and/or nose.13-15
Precipitants of herpes labialis include concurrent illness, UV light exposure, and pregnancy. Effective therapy en-tails 5% aciclovir16 or 1% penciclovir.17 Herpes labialis may
itself be a precipitant of erythema multiforme.18 Figure 1 - Chemotherapy induced oral mucositis
Figure 2 - Primary infection of HSV-1 affecting the gingival, tongue and skin
This therapy typically provides symptomatic relief, al-though systemic aciclovir and other anti-virals should be considered when disease is severe, recurrent, or atypical.13
Aciclovir resistance may arise in immunosuppressed pa-tients receiving repeated treatments, hence the need for
famciclovir, valciclovir or foscarnet.14 Interestingly,
foscarnet may itself give rise to oral ulcers,15 and while
aciclovir may be effective and useful in the treatment of erythema multiforme, it can also give rise to this mucosal disorder.
Herpes simplex virus 2, Epstein-Barr virus and Cytomegalovirus
Although uncommon, HSV-2 can give rise to oral ul-cers similar to that of mild primary HSV-1 infection. This oral ulcer arises as a consequence of orogenital transmis-sion of the causative virus.
Ulcers caused by Epstein–Barr virus (EBV) are rare, but may be a feature of infectious mononucleosis. The ulcers comprise a few small superficial ulcers of the oral mucosa. EBV is more typically associated with the ulcers of some
non-Hodgkin’s lymphomas19 or white patches termed oral
hairy leukoplakia (OHL) that may arise in cases of immu-nodeficiency (e.g. HIV, or with corticosteroid or other sys-temic immunosuppressant therapy, etc.). It is also impor-tant to remember that OHL has been observed in patients with inflammatory bowel disease receiving immunosup-pressive regimes.20
Cytomegalovirus (CMV) may give rise to large, chronic ulcers of the oral mucosa or gingiva.21 These CMV-related
ulcers occur exclusively under conditions of significant immunodeficiency, notably severe HIV disease. The diag-nosis of such ulcers is difficult and is often only confirmed by resolution of ulcers with ganciclovir therapy.22
Human herpesvirus 8 (Kaposi’s sarcoma herpes virus)
Human herpesvirus 8 (HHV-8) is an oncogenic virus, which causes Kaposi’s sarcoma (KS). It is theorized that this virus, when infecting circulating KS cell-progenitors, predisposes a patient to KS development in the setting of exposure to Th1 inflammatory cytokines. Lytic replication caused by the virus can further promote tissue inflamma-tion, thereby providing a proangiogenic stimulus that, among other things, increases generation of matrix metalloproteinases. In this multifactorial model of infec-tion, hypoxia and injury can lead to the clinical expression of KS. Commonly arising within the mouth of patients with severe HIV disease or as a feature of profound iatrogenic immunosuppression (e.g. in patients with inflammatory bowel disease). Oral KS typically affects the palate or gingiva and manifests as red, blue or purple macules,
papules, nodules or ulcers (Fig. 4).23 Oral KS may also
oc-casionally be non-pigmented, and hence may mimic SCC.24
Kaposi’s sarcoma of the anterior gingiva may be un-sightly, and in rare instances, gingival lesions will cause the destruction of underlying periodontal tissues, leading to tooth loss and sequestration of bone.
Oral KS in HIV may be reduced or resolved with highly active antiretroviral therapy (HAART); although some oral lesions have been reported to resolve (probably transiently) with local radiotherapy, local injection of cytotoxics, or sclerosants.25 27
Human immunodeficiency virus
The oral consequences of HIV have been reviewed in de-tail elsewhere.28,29 Infection with HIV gives rise to a wide
spec-trum of oral ulcerative lesions. The majority of these are de-tailed in other sections of the review. A minority of patients with severe HIV disease can develop deep, necrotic ulcers of unknown etiology. These ulcers are painful, can cause pro-found dysphagia and/or dysarthria, and can arise on any oral mucosal surface, although the buccal and pharyngeal mucosae are the more commonly affected sites. The precise etiology
of these HIV-related ulcers is unknown.30 HHV-8 DNA has
been detected within such ulcers, although it is unclear whether the virus is causative or merely a passenger.31 Of note,
such ulcers typically resolve with systemic thalidomide (e.g. 200 mg daily), perhaps reflecting an antitumor necrosis fac-tor (TNF)-á effect, which supports a viral etiology.32 Small
numbers of patients with HIV disease may have ulcers simi-lar to those of recurrent aphthous stomatitis (RAS) (Fig. 5); to date, the cause of RAS has not been established. This limi-tation continues to compromise the clinician’s ability to pro-vide effective therapy. Whether the frequency of RAS is truly increased in HIV also remains unclear.33
Vincent’s disease manifests as painful ulcers of the gingival margins, particularly the interdental areas. The ul-cers may be localized or generalized and, when severe, they will give rise to cervical lymphadenopathy and, very rarely, to pyrexia and malaise. There is often oral malodor asso-ciated with Vincent’s disease. Long-standing or recurrent disease may lead to destruction and loss of interdental pa-pillae.
An ANUG-like disease termed cancrum oris (noma) (Figs. 7 and 8) can arise in profoundly malnourished chil-dren and adults. Unlike the ANUG in immunocompetent individuals, the ulcers of cancrum oris spread to the adja-cent soft tissues, leading to necrosis of the lips and/or cheeks. Cancrum oris has most commonly been reported in children in Central Africa, where malnourishment arises from poverty that results from political and economical unrest.35
An ANUG-like disorder that spreads to the underlying bone and adjacent soft tissues – termed necrotizing stoma-titis – has been reported in a small number of patients with severe HIV disease. Occasionally, this disorder may be the first, and/or only clinical manifestation of HIV disease.36
Bacterial infection
Acute necrotizing ulcerative gingivitis
Acute necrotizing ulcerative gingivitis (Vincent’s dis-ease, trench mouth, acute ulcerative gingivitis) is a non-specific ulcerative disorder that is almost always localized to the gingivae (Fig. 6).34 Associated contributing factors
include poorly controlled diabetes mellitus, tobacco smok-ing, immunodeficiency (notably severe HIV disease), and possibly psychological stress. This condition is also asso-ciated with poor oral hygiene. Measles and malnutrition have also been implicated as predisposing factors to Acute Necrotizing Ulcerative Gingivitis (ANUG), common oral diseases prevalent among children ages 3-6 years living in rural communities.
Figure 5 - Oral ulceration in HIV infected patient
Figure 6 - Acute necrotizing ulcerative gingivitis also affecting the hard
palate Figure 8 - Cutaneous necrosis secondary to cancrum oris
Ulcers of ANUG typically resolve with the removal of deposits of plaque and calculus and the topical application of chlorhexidine gluconate mouth rinse (0.2%) or gel (1%). Systemic antimicrobials (e.g. metronidazole or phenoxymethyl penicillin) may be required when the gin-givitis is profound and/or there is systemic upset. Cancrum oris also requires tissue debridement and correction of the underlying malnourishment; however, prognosis for the af-fected children is often poor.37 Post-healing fibrosis and
scarring represent a significant complication of cancrum oris.
Treponema pallidum
The frequency of oral ulcers due to infective syphilis is likely to increase as a consequence of the rising number of subjects affected with Treponema pallidum; this may re-flect changes in sexual attitudes and behavior, changing trends in HIV disease, and increased foreign travel.38 Oral
ulcers can arise in primary, secondary or tertiary disease. In primary disease, a chancre can develop on the oral mu-cosa as a consequence of direct contact with an infective lesion. Ulcers of a primary infection typically arise on the upper (in females) or lower lip (in males) and manifest as a superficial to deep isolated ulcer that sometimes has a rolled edge. Occasionally, there can be isolated ulcers of the gingiva.39 The oral chancre typically resolves with
an-timicrobial therapy.40 Secondary syphilis can give rise to
multiple areas of superficial papules and ulcers, some of the latter being serpiginous, and are thus termed snail-track ulcers. Tertiary disease may produce ulcers as a conse-quence of gumma formation, with the ulcers manifesting as isolated areas of chronic ulceration, sometimes with the destruction of the underlying soft and/or hard tissues (e.g. palate or tongue).
Mycobacterial infection
Primary oral infection of Mycobacterium tuberculosis
is rare;41 more commonly, tuberculosis infection of the oral
mucosa arises secondary to pulmonary disease. Tubercu-losis typically presents as solitary, necrotic ulcers of the tongue. Infection by atypical mycobacteria (e.g. Mycobac-terium avium complex) is rare, but may affect the oral mu-cosa or gingiva, usually in HIV-infected individuals.42
Yeast and Fungal infections
While Candida species, usually Candida albicans, are the most common fungal infection of the mouth, these rarely give rise to oral ulcers. Chronic mucocutaneous can-didiasis (CMC) is one of the most common T-cell diseases,
but the exact underlying defect is unknown. The disease usually starts in early childhood, but it may also start as late as early adolescence. Affected children have persist-ent oral thrush, napkin dermatitis, skin infections, dys-trophic nails, alopecia, and thrush on the genital skin and oral mucous membranes. Candida granulomas rarely oc-cur. Although fungal infection is the most important fea-ture of this disease, in rare cases, recurrent bacterial infec-tions and viral infecinfec-tions such as herpes simplex, herpes zoster and hepatitis can occur. This condition may occa-sionally give rise to ulcers of the dorsum of tongue.43
Systemic mycoses can cause oral ulcers, typically in
immunosuppressed hosts. In HIV disease, Aspergillus
fumigatum may give rise to long-standing ulcers of the gingiva44 or oral mucosa as may Histoplasma capsulatum.45
South America paracoccidiodomycosis (South American Blastomycosis) may give rise to large areas of ulcers remi-niscent of oral SCC, with this infection arising in both
im-munocompetent and immunosuppressed individuals.46,47
Idiopathic ulcers
Recurrent aphthous stomatitis
The most common non-infectious and non-traumatic oral mucosal ulcerative disorder is recurrent aphthous sto-matitis (RAS) (Fig. 9). The disease affects non-keratinized oral mucosa, especially the vestibulum, soft palate, tongue and sublingual area. It is clinically characterized by recur-rent episodes of oral ulceration in an otherwise healthy in-dividual. The ulcers arise every 4–12 weeks and may be classified as minor, major, or herpetiform. The ulcers are superficial, rounded and have a yellow-colored slough with surrounding erythema. The ulcers of major RAS may cause scarring upon healing, and it has been suggested that ul-cers of herpetiform RAS may coalesce to produce large ar-eas of ulcers that heal with scarring. Rarely, major
thous stomatitis causes tissue destruction (e.g. of the soft palate).
Undoubtedly, RAS has an immunologically mediated pathogenesis; however, the precise cause of RAS remains unclear. Reduced percentages of CD4 and CD8 cells in pe-ripheral blood have been documented, but the results are still controversial.48 Suggested etiologies include idiopathic
hematoma deficiency, cessation of tobacco smoking, and psychological stress, but there is little scientific evidence to support of any of these. While superficial ulcers similar to RAS may arise in gluten-sensitive enteropathy,49 the vast
majority of patients with RAS have no clinical, gastroenterological, or serological features of this small bowel disorder. To date, no common viral or bacterial in-fection of the mouth has been implicated in the etiology of RAS.48 There is also no consistent association between Helicobacter pylori infection and RAS.50
Therapy for RAS is directed towards reducing the du-ration and/or frequency of episodes of ulcedu-ration.51
Topi-cal corticosteroids are used in the most cases; however, few of these have been found to be significantly effective in appropriate clinical studies. Chlorhexidine gluconate mouth rinse may be of some benefit (and has been evaluated in detail),52 but it has only limited clinical value in the
man-agement of RAS. Benzydamine hydrochloride spray or mouth rinse provides some symptomatic relief, but does not hasten ulcer healing. Although effective, systemic therapy with prednisone is rarely warranted, and the mechanism of this effect is unclear.53-55 Thalidomide is highly effective,
but in view of the adverse side effects including teratogenicity and neurotoxicity, its routine application for such a recurrent and minor disorder is contraindicated.56
Ulcers similar to RAS are one of the cardinal features of Behcet’s disease. The ulcers have only rarely been de-scribed in detail, but seem to have the same clinical fea-tures as RAS. A detailed discussion of Behcet’s disease can be found elsewhere.57 Other disorders that can give rise to
RAS-like ulcers include a variant of Behcet’s disease termed MAGIC syndrome, Sweet’s syndrome, and HIV dis-ease.58 A rare disorder in childhood that is characterized
by pyrexia, pharyngitis, cervical lymphadenopathy and aph-thous-like ulcers, sometimes termed PFAPA (periodic fe-ver, aphthae, pharyngitis and adenitis), has also been de-scribed.59
Oral ulcers related to systemic disease
Gastrointestinal disease
Gluten-sensitive enteropathy
Superficial oral mucosal ulcers similar to RAS may be
a feature of 1–5% patients with undiagnosed, untreated glu-ten-sensitive enteropathy.60 The ulceration is presumably
due to the associated hematinic deficiencies.
Dermatitis herpetiformis and related disorders
Oral lesions in dermatitis herpetiformis have been de-scribed only rarely. These may comprise oral mucosal vesi-cles, blood-filled blisters, irregular ulcers and desquama-tive gingitivitis. Linear IgA disease may likewise give rise to blood-filled vesicles or bullae, irregular ulcers and desq-uamative gingivitis. A long-term gluten-free diet (GFD) has been used successfully as a first-choice treatment for der-matitis herpetiformis (DH).61
Crohn’s disease and related disorders
Oral ulcers arise in approximately 9% of patients with undiagnosed Crohn’s disease and can be the first and/or only clinical features of this disorder. Crohn’s disease is a systemic chronic inflammatory disorder that may involve any part of the gastrointestinal tract, including the oral cav-ity. The prevalence rates of oral manifestations vary be-tween 5 and 20 per cent; however, in pediatric patients, the
prevalence is much higher (48% to 80%).62 Two types of
oral ulcers can arise in orofacial granulomatosis (OFG) and Crohn’s disease – chronic deep linear ulcers, usually of the buccal vestibules, which often have a rolled edge because of mucosal tags; and superficial oral mucosal ulcers (Fig. 10) presumably resulting from hematinic deficiency. The diagnosis of such ulcers requires establishing the presence of non-caseating granulomas and the exclusion of other granulomatous diseases, such as sarcoidosis.
The precise relationship between OFG and gastrointestinal Crohn’s disease remains unclear since there are few studies examining the gastrointestinal tract of
dren and adults with OFG. Certainly, there are reports of OFG as an initial presentation of Crohn’s disease.63,64
Simi-larly, OFG-like disease may be a feature of patients with concurrent gastrointestinal Crohn’s disease.65,66 The human
leukocyte antigen (HLA) haplotype of patients with OFG differs from that of Crohn’s disease.67 The precise
associa-tion between OFG and gastrointestinal Crohn’s disease re-mains unknown.
Ulcerative colitis
Ulcerative colitis can give rise to either aphthous ul-cers or to multiple pustules called pyostomatitis vegetans. The ulcers of the latter arise on the upper and lower ante-rior vestibules, the soft palate, and the posteante-rior hard pal-ate. Pyostomatitis vegetans tends to arise in patients with undiagnosed or active ulcerative colitis. Although most fre-quently associated with ulcerative colitis, pyostomatitis vegetans may occasionally arise in Crohn’s disease.68
Pyo-derma gangrenosum, manifesting as a solitary, necrotic mucosal ulcer has also been reported in the mouth in rare cases.69
Others
As discussed above, necrotizing sialometaplasia may arise secondary to palatal trauma in bulimia nervosa. Gastro-esophageal reflux does not cause oral ulceration, although it has been associated with erosion of the palatal aspects of the upper teeth.70
Lichen planus
Lichen planus is by far the most common dermatologi-cal disorder that gives rise to oral ulcers. Lichen planus is an immunologically mediated disorder that is histopatho-logically characterized by an intense dermal infiltrate of T-lymphocytes. The precise trigger for this immunologi-cal reaction is unclear. There is no evidence that the clini-cal features of idiopathic oral lichen planus are any differ-ent from those of the drug-associated diseases (Figs. 11 and 12).71
Similarly, although histopathological differences be-tween idiopathic lichen planus and drug-related diseases have been described, there is profound inconsistency among the proposed pathological hallmarks of these two disor-ders.72 Drugs that may commonly give rise to lichen
pla-nus-like disease include sulphonyureas, non-steroidal anti-inflammatory drugs, β-blockers, antimalarials, penicilla-mine and gold. Associations between hepatitis C virus and oral lichen planus probably reflect the epidemiology of hepatitis C virus infection and/or use of interferon-α.73 A
lichen planus-like disorder can also arise in chronic graft-versus-host disease.
Lichen planus only warrants treatment in patients who are having painful symptoms and/or signs of erosion, ul-cers, or blister formation. Typical treatment involves topi-cal corticosteroids,74 although severe cases may warrant
lo-cal (e.g. topilo-cal tacrolimus) and systemic immunosuppres-sant therapy75, 76, the latter of which does not have a strong
evidence base.
Of note, it has been suggested that oral lichen planus may be potentially malignant. The evidence for this is gen-erally based upon retrospective studies of large numbers of affected patients. It is suggested that approximately 1– 3% of patients with long-standing lichen planus may de-velop oral SCC.77 Often, however, the descriptions have not
detailed whether the tumor arose within existing lichen
pla-Figure 12 - Lateral view of erosive non-striated oral lichen planus affecting the dorsum of the tongue
nus, and no detailed prospective control studies of the de-velopment of oral SCC in long-standing lichen planus have ever been undertaken.
Malignancy
The common malignancies of the mouth may manifest as oral ulcers. SCC is the most common tumor of the mouth, typically manifesting as a solitary ulcer of the dor-sum of tongue or floor of mouth (Fig. 13). The ulceration is locally destructive and, when affecting the tongue, may give rise to lingual and/or hypoglossal nerve damage with or without dysarthria or dysphagia. Gingival SCC may give rise to tooth mobility and, very rarely, to a pathological fracture of the mandible.
Oral SCC remains one of the more common cancers worldwide, particularly in developing countries such as In-dia.78-80 There is a rising frequency of oral SCC in the
mid-dle-aged adult population in the developed world. High to-bacco (in any form) and alcohol consumption are the prin-cipal etiological factors of oral SCC. Other suggestive etiologies include human papilloma virus, malnourishment
(in particular deficiencies of vitamins A and C), and pos-sibly poor oral hygiene.
Non-Hodgkin’s lymphoma
Non-Hodgkin’s lymphoma may manifest as a solitary area of necrotic ulcers typically affecting the gingiva, pal-ate and fauces. This tumor may arise de novo, but is often associated with iatrogenic immunosuppression in HIV dis-ease. A detailed review of non-Hodgkin’s lymphoma of the
mouth can be found elsewhere.81 NK/T-cell lymphoma
tends to affect the upper anterior gingival and palate; this is a T-cell lymphoma, which is in contrast to most
non-Hodgkin’s lymphoma of the mouth.82,83
Drug therapy
A wide range of drugs can give rise to ulcers of the oral
mucosa.84 The mechanisms by which drugs cause oral
ul-cers include drug-induced neutropenia and anemia (e.g.
cytotoxics), lichenoid disease (e.g. sulphanylureas, â
-blockers, gold, penicillamine), pemphigus (e.g. angiotensin-converting enzyme inhibitors), lupus, and IgA dermatoses.
Leishmaniasis
Cutaneous leishmaniasis, endemicin some parts ofthe
Americas, is causedby Leishmania viannia and
Leishma-nia mexicanaspecies complexes. Infection withL. viannia
species, particularly Leishmania viannia braziliensis,results in skin lesionsthat tend to bepersistent and may befurther
complicated by mucocutaneousinvolvement. Mucosal
leishmaniasisprobably results from earlyhematogenous or
lymphatic spreadfrom cutaneous lesions. Itcauses destruc-tion of thefacial structure, which maylead to aspiration,
infection,and even death. Mucosalleishmaniasis may
ap-pear atany time, from thefirst months after infectionto dec-ades afterward. Risk factors includelarge or multiple cu-taneouslesions, male gender, andlong-standing skin lesions
forwhich adequate systemic treatmenthas not been
admin-istered.85 Figure 13 - Oral squamous cell carcinoma on the dorsum of the tongue and
floor of the mouth.
RESUMO
Leão JC, GomesVB, Porter S. Lesões ulcerativas da boca:
atualização para o clínico geral. Clinics. 2007;62(6):769-80.
A ulceração oral é uma queixa comum dos pacientes que são atendidos em ambulatórios. Com freqüência é difícil estabelecer um diagnóstico preciso e atingir o controle dos
da etiologia, diagnóstico e tratamento das desordens ulcerativas mais comuns da mucosa oral. Foi realizada uma busca no banco de dados MEDLINE da National Library of Medicine. A seleção dos artigos, coleta de dados e julgamento em termos da pertinência de inclusão foram realizadas pelos autores. Baseado na literatura pesquisada, foi concluído que existem várias doenças sistêmicas que
podem apresentar sinais e sintomas clínicos semelhantes e o conhecimento de cada doença poderá guiar o clínico para uma intervenção apropriada.
UNITERMOS: Ulceração Oral. Medicina Oral. Lesões Orais. Estomatite Aftosa Recorrente. Ulceração Oral Recorrente
REFERENCES
1. Gandara-Rey JM, Diniz-Freitas M, Gandara-Vila P, Blanco-Carrion A, Garcia-Garcia A. Lesions of the oral mucosa in cocaine users who apply the drug topically. Med Oral. 2002;7(2): 03-7.
2. Blanksma CJ, Brand HS. Cocaine abuse: orofacial manifestations and implications for dental treatment. Int Dent J. 2005;55:365-9. 3. Goodger NM, Wang J, Pogrel MA. Palatal and nasal necrosis resulting
from cocaine misure. Br Dent J. 2005;198:333-4.
4. Epstein JB, Klasser GD. Emerging approaches for prophylaxis and management of oropharyngeal mucositis in cancer therapy. Expert Opin Emerg Drugs. 2006;11:353-73.
5. Dorr W, Reichel S, Spekl K. Effects of Keratinocyte growth factor (palifermin) administration protocols on oral mucositis (mouse) induced by fractionated irradiation. Radiother Oncol. 2005;75:99-105. 6. Fleisher G, Dorr W. Amelioration of early radiation effects in oral mucosa
(mouse) by intravenous or subcutaneous administration of amifostine. Strahlenther Onkol. 2006;182:567-75.
8. Robinson JA, Shankaramma Sc, Jetter P, Kienze U, Schwendener RA, Vrijbloed JW, Obrecht D. Properties and structure-activity studies of cyclic beta-hairpin peptidomimetics based on the cationic antimicrobial peptide protegrin I. Bioorg Med Chem. 2005;13:2055-64.
9. Kominek P, Blasch P. Necrotizing sialometaplasia: a potential diagnostic pitfall. Ear Nose Throat J. 2006;85:604-5.
10. Solomon LW, Merzianu M, Sullivan M, Rigual NR. Necrotizing sialometaplasia associated with bulimia: case report and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:39-42. 11. Bunzli D, Wietlisbach V, Barazzoni F, Sahki R, Meylan PR.
Soroepidemiology of herpes simplex virus type 1 and 2 in Western and Southern Switzerland in adults aged 25-74 in 1992-93: a population-based study. BMC Infect Dis. 2004;174:10.
12. Malkin JE. Epidemiology of genital herpes simplex virus infection in developed countries. Herpes. 2004;11 suppl 1:2A–23A.
13. Ficarra G. Oral ulcers in HIV-infected patients: an update on epidemiology and diagnosis. Oral Dis. 1997;3 suppl 1:S183-9. 14. Kleymann G. Agents and strategies in development for improved
management of herpes simplex virus infection and disease. Expert Opin Investig Drugs. 2005;14:135-61.
15. Wu JJ, Pang KR, Huang DB, Tyring SK. Advances in antiviral therapy. Dermatol Clin. 2005;23:313-22.
16. Van der Pijl JW. Prevention of genital ulcerations during treatment with foscarnet. Presse Med. 1992;21:395.
17. Morrel EM, Spruance SL, Goldberg DI and Iontophoretic Acyclovir Cold Sore Study Group. Topical iontophoretic administration of acyclovir for the episodic treatment of herpes labialis: a ramdomized, double-blind, placebo-controlled, clinic-initiated trial. Clin Infect Dis. 2006;43:460-7.
18. Sarisky RT, Bacon T, Boon R, Locke L, Nguyen TT, Leary J, et al. Penciclovir susceptibilities of herpes simplex virus isolates from patients using penciclovir cream for treatment of recurrent herpes labialis. Antimicrob Agents Chemother. 2002;46:2848–53.
19. Kokuba H, Imafuku S, Huang S, Aurelian L, Burnett JW. Erythema multiforme lesions are associated with expression of a herpes simplex virus (HSV) gene and qualitative alterations in the HSV-specific T-cell response. Br J Dermatol. 1998;138:952–64.
20. Szczepanski T, De Vaan GA, Beishuizen A, Bogman J, Jansen MW, van Wering ER et al. Acute lymphoblastic leukemia followed by a clonally-unrelated EBV-positive non-Hodgkin lymphoma and a clonally-related myelomonocytic leukemia cutis. Pediatr Blood Cancer. 2004;42:343–9. 21. Fluckiger R, Laifer G, Itin P, Meyer B, Lang C. Oral hairy leukoplakia in a patient with ulcerative colitis. Gastroenterology. 1994;106:506–8. 22. Firth NA, Rich AM, Reade PC. Oral mucosal ulceration due to cytomegalovirus associated with human immunodeficiency virus infection. Case report and brief review. Aust Dent J. 1994;39:273-5. 23. Flaitz CM, Nichols CM, Hicks MJ. Herpesviridae-associated persistent
mucocutaneous ulcers in acquired immunodeficiency syndrome. A clinicopathologic study. Oral Surg Oral Med Oral PatholOral Radiol Endod. 1996;81:433-41.
24. Lager I, Altini M, Coleman H, Ali H. Oral Kaposi’s sarcoma: a clinicopathologic study from South Africa. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:701-10.
25. Reichart PA, Schiodt M. Non-pigmented oral Kaposi’s sarcoma (AIDS). Report of two cases. Int J Oral Maxillofac Surg. 1989;18:197-9. 26. Diz DP, Ocampo HA, Miralles AC, Vazquez GE, Martinez VC.
Regression of AIDS-related Kaposi’s sarcoma following ritonavir therapy. Oral Oncol. 1998;34:236-8.
27. Le Bourgeois JP, Frikha H, Piedbois P, Le Pechoux C, Martin L, Haddad E. Radiotherapy in the management of epidemic Kaposi’s sarcoma of the oral cavity, the eyelid and the genitals. Radiother Oncol. 1994;30:263-6.
28. Ramirez-Amador V, Esquivel-Pedraza L, Lozada-Nur F, et al.
Intralesional vinblastine vs. 3% sodium tetradecyl sulfate for the treatment of oral Kaposi’s sarcoma. A double blind, randomized clinical trial. Oral Oncol. 2002;38:460-7.
29. Scully C, Laskaris G, Pindborg J, Porter SR, Reichart P. Oral manifestations of HIV infection and their management: II. Less common lesions. Oral Surg Oral Med Oral Pathol. 1991;71:167-71.
30. Scully C, Laskaris G, Pindborg J, Porter SR, Reichart P. Oral manifestations of HIV infection and their management: I. More common lesions. Oral Surg Oral Med Oral Pathol. 1991;71:158-66.
31. MacPhail LA, Greenspan JS. Oral ulceration in HIV infection: investigation and pathogenesis. Oral Dis. 1997;3:190-3.
32. Di Alberti L, Porter SR, Speight PM, Scully CM, Zakrzewska JM, Williams IG et al. Detection of human herpesvirus-8 DNA in oral ulcer tissues of HIV-infected individuals. Oral Dis. 1997;1:133-4. 33. Ramirez-Amador VA, Esquivel-Pedraza L, Ponce-de-Leon S,
Reyes-Teran G, Gonzalez-Guevara M, Ponce-de-Leon Set al. Thalidomide as therapy for human immunodeficiency virus-related oral ulcers: a double-blind placebo-controlled clinical trial. Clin Infect Dis. 1999;28:892-4. 34. Baccaglini L, Atkinson JC, Patton LL, Glick M, Ficarra G, Peterson DE. Managment of oral lesions in HIV-positive patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:21-23.
35. Okolo S, Chukwu G, Eqbuonu I, Ezeogu F, Onwuanaku C, Adeleke O et al. Oral hygiene and nutritional status of children aged 1-7 years in a rural community. Ghana Med J. 2006;40: 22-5.
36. Enwonwu CO, Falkler WA Jr, Idigbe EO, Afolabi BM, Ibrahim M, Onwujekwe D et al. Pathogenesis of cancrum oris (noma): confounding interactions of malnutrition with infection. Am J Trop Med Hyg. 1999;60:223-32.
37. Jones AC, Gulley ML, Freedman PD. Necrotizing ulcerative stomatitis in human immunodeficiency virus-seropositive individuals: a review of the histopathologic, immunohistochemical, and virologic characteristics of 18 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:323-32.
38. Adekeye EO, Ord RA. Cancrum oris: principles of management and reconstructive surgery. J Maxillofac Surg. 1983;11:160-70.
39. Alam F, Argiriadou AS, Hodgson TA, Kumar N, Porter SR. Primary syphilis remains a cause of oral ulceration. Br Dent J. 2000;189:352–4. 40. Steiner M, Alexander WN. Primary syphilis of the gingiva. Report of
two cases. Oral Surg Oral Med Oral Pathol. 1966;21:530–5. 41. Schofer H. Syphilis. Clinical aspects of Treponema pallidum infection.
42. Ajay GN, Laxmikanth C, Prashanth SK. Tuberculous ulcer of tongue with oral complications of oral antituberculosis therapy. Indian J Dent Res. 2006;17:87-90.
43. Ilyas SE, Chen FF, Hodgson TA, Speight PM, Lacey CJ, Porter SR. Labial tuberculosis: a unique cause of lip swelling complicating HIV infection. HIV Med. 2002;3:283-6.
44. Sathis Kumar T, Xavier SJ, Renu G. Chronic mucocutaneous candidiasis in a child. Indian J Dermatol Venerol Leprol. 2005;71:432-3. 45. Myoken Y, Sugata T, Kyo TI, Fujihara M. Pathological features of
invasive oral aspergillosis in patients with hematologic malignancies. J Oral Maxillofac Surg. 1996;54:263-70.
46. Loh FC, Yeo JF, Tan WC, Kumarasinghe G. Histoplasmosis presenting as hyperplastic gingival lesion. J Oral Pathol Med. 1989;18:533–6. 47. Scully C, de Almeida OP. Orofacial manifestations of the systemic
mycoses. J Oral Pathol Med. 1992;21:289-94.
48. Ranganathan K, Hemalatha R. Oral lesions in HIV infection in developing countries: an overview. Adv Dent Res. 2006;19:63-8. 49. Moraru RA, Grossman ME. Palatal necrosis in an AIDS patient: a case
of mucormycosis. Cutis. 2000;66:15-8.
50. Porter SR, Scully C, Pedersen A. Recurrent aphthous stomatitis. Crit Rev Oral Biol Med. 1998;9:306-21.
51. Srinivasan U, Weir DG, Feighery C, O’Farrelly C. Emergence of classic enteropathy after longstanding gluten sensitive oral ulceration. BMJ. 1998;316:206-7.
52. Porter SR, Barker GR, Scully C, Macfarlane G, Bain L. Serum IgG antibodies to Helicobacter pylori in patients with recurrent aphthous stomatitis and other oral disorders. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83:325-8.
53. Porter S, Scully C. Aphthous ulcers: recurrent. Clin Evid. 2002;8:1397-403.
54. Hunter L, Addy M. Chlorhexidine gluconate mouthwash in the management of minor aphthous ulceration. A double-blind, placebo-controlled cross-over trial. Br Dent J. 1987;162:106-10.
55. Barrons RW. Treatment strategies for recurrent oral aphthous ulcers. Am J Health Syst Pharm. 2001;58:41-50.
56. MacPhail L. Topical and systemic therapy for recurrent aphthous stomatitis. Semin Cutan Med Surg. 1997;16:301-7.
57. Eisen D, Lynch DP. Selecting topical and systemic agents for recurrent aphthous stomatitis. Cutis. 2001;68:201-6.
58. Shetty K. Thalidomide in the management of recurrent aphthous ulcerations in patients who are HIV-positive: a review and case reports. Spec Care Dentist. 2005;25:236-41.
59. Arayssi T, Hamdan A. New insights into the pathogenesis and therapy of Behcet’s disease. Curr Opin Pharmacol. 2004;4:183-8.
60. Femiano F, Gombos F, Scully C. Sweet’s syndrome: recurrent oral ulceration, pyrexia, thrombophlebitis, and cutaneous lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:324-7.
61. Feder HM Jr. Periodic fever, aphthous stomatitis, pharyngitis, adenitis: a clinical review of a new syndrome.Curr Opin Pediatr. 2000;12:253-6.
62. Nowak M, Dziechciarz P, Dwilewicz-Trojaczek J. The frequency of coeliac disease occurrence in patients with recurrent aphthous stomatitis (RAS) – preliminary report. Wiad Lek. 2002;55:542-6.
63. O’Regan E, Bane A, Flint S, Timon C, Toner M. Linear IgA disease presenting as desquamative gingivitis: a pattern poorly recognized in medicine. Arch Otolaryngol Head Neck Surg. 2004;130:469-72. 64. Harty S, Fleming P, Rowland M, Crushell E, McDermott M, Drumm B,
et al. A prospective study of the oral manifestations of Crohn’s disease. Clin Gastroenterol Hepatol. 2005;3:886-91.
65. Sanderson J, Nunes C, Escudier M, Barnard K. Oro-facial granulomatosis: Crohn’s disease or a new inflamatory bowel disease? Inflamm Bowel Dis. 2005;11:840-6.
66. Kauzman A, Quesnel-Mercier A, Lalonde B. Orofacial granulomatosis: 2 cases reports and literature review. J Can Dent Assoc. 2006;71:325-9. 67. Orosz M, Sonkodi I. Oral manifestations in Crohn’s disease and dental
management. Fogorv Sz. 2004;97:113-7.
68. Tyldesley WR. Oral Crohn’s disease and related conditions. Br J Oral Surg. 1979;17:1-9.
69. Gibson J, Neilly JB, Wray AP, Evans TJ, MacKenzie JR, McKillop JH. [99Tcm]-HMPAO leucocyte labelling in orofacial granulomatosis and gastrointestinal Crohn’s disease in childhood and early adulthood. Nucl Med Commun. 2000;21:155-8.
70. Ficarra G, Cicchi P, Amorosi A, Piluso S. Oral Crohn’s disease and pyostomatitis vegetans. An unusual association. Oral Surg Oral Med Oral Pathol. 1993;75:220-4.
71. Hernandez-Martin A, Arias-Palomo D, Hermida G, Gutiérrez-Ortega MC, Ramírez-Herrera M, Rodríguez-Vegas M et al. Oral pyoderma gangrenosum. Br J Dermatol. 2003;149:663-4.
72. Lackey MA, Barth J. Gastroesophageal reflux disease: a dental concern. Gen Dent. 2003;51:250-4.
73. Scully C, Beyli M, Ferreiro MC, Ficarra G, Gill Y, Griffiths M et al. Update on oral lichen planus: etiopathogenesis and management. Crit Rev Oral Biol Med. 1998;9:86-122.
74. McCartan BE, McCreary CE. Oral lichenoid drug eruptions. Oral Dis. 1997;3: 58-63.
75. Bratel J, Dahlgren U, Simark MC, Jontell M. The frequency of different T-cell receptor V-families in oral lichen planus and lichenoid contact lesions: an immunohistochemical study. J Oral Pathol Med. 1998;27:415-9.
76. Nagao Y, Sata M, Ide T. Development and exacerbation of oral lichen planus during and after interferon therapy for hepatitis C. Eur J Clin Invest. 1996;26:1171-4.
77. Hegarty AM, Hodgson TA, Lewsey JD, Porter SR. Fluticasone propionate spray and betamethasone sodium phosphate mouthrinse: a randomized crossover study for the treatment of symptomatic oral lichen planus. J Am Acad Dermatol. 2002;47:271-9.
78. Kaliakatsou F, Hodgson TA, Lewsey JD, Hegarty AM, Murphy AG, Porter SR. Management of recalcitrant ulcerative oral lichen planus with topical tacrolimus. J Am Acad Dermatol. 2002;46:35-41.
80. Rodstrom PO, Jontell M, Mattsson U, Holmberg E. Cancer and oral lichen planus in a Swedish population. Oral Oncol. 2004;40:131-8. 81. Silverman S, Bhargava K, Smith LW, Malaowalla AM. Malignant
transformation and natural history of oral leukoplakia in 57,518 industrial workers of Gujarat, India. Cancer. 1976;38:1790-5. 82. Gupta PC, Mehta FS, Pindborg JJ. Intervention study for primary
prevention of oral cancer among 36000 Indian tobacco users. Lancet. 1986;1:1235-9.
83. Rajkumar T, Sridhar H, Balaram P. Oral cancer in Southern India: the influence of body size, diet, infections and sexual practices. Eur J Cancer Prev. 2003;12:135-43.
84. Porter S, Scully C. HIV: the surgeon’s perspective: Part 3. Diagnosis and management of malignant neoplasms. Br J Oral Maxillofac Surg. 1994;32:241-7.