Abst ract
Submitted: September 20, 2016 0RGL¿HG'HFHPEHU Accepted: February 2, 2017
Met rical analysis of disc- condyle
relat ion w it h different splint t reat m ent
posit ions in pat ient s w it h TMJ disc
displacem ent
Obj ect ive: To evaluat e t he effect of bit e posit ions charact erizing different splint t reat m ent s ( ant erior reposit ioning and st abilizat ion splint s) on t he disc- condyle relat ion in pat ient s w it h TMJ disc displacem ent w it h reduct ion ( DDw R) , using m agnet ic resonance im aging ( MRI ) . Mat erial and Met hods: 37 pat ient s, w it h a m ean age of 18.8± 4.3 years ( 7 m ale and 30 fem ales) and diagnosed w it h DDw R based on t he RDC/ TMD, w ere recruit ed. MRI m et rical analysis of t he spat ial changes of t he disc/ condyle, as w ell as t heir relat ionships, was done in t hree posit ions: m axim um int ercuspat ion ( Posit ion 1) , ant erior reposit ioning splint posit ion ( Posit ion 2) , and st abilizat ion splint posit ion ( Posit ion 3) . Disc/ condyle coordinat e m easurem ent s and disc condyle angles w ere det erm ined and com pared. Result s: I n Posit ion 1, t he average disc- condy le angle was 53.4° in t he 60 j oint s w it h DDw R, w hile it was
íZLWK3RVLWLRQDQGZLWK3RVLWLRQ7KHIUHTXHQF\RIVXFFHVVIXO ³GLVF UHFDSWXUH´ ZLWK 3RVLWLRQ ZDV VLJQL¿FDQWO\ KLJKHU
t han Posit ion 3 ( 20/ 60, 33.3% ) . I n Posit ions 2 and 3, t he condyle m oved forward and dow nward w hile t he disc m oved backward. The m ovem ent s w er e, how ever, m or e r em ar k able w it h Posit ion 2. Conclusions: Ant er ior reposit ioning of t he m andible im proves t he spat ial relat ionship bet w een t he disc and condyle in pat ient s w it h DDw R. I n addit ion t o ant erior and inferior m ovem ent of t he condyle, t ransit ory post erior m ovem ent of t he disc also occurred.
K e y w o r d s : Te m p o r o m a n d i b u l a r j o i n t . M a n d i b u l a r c o n d y l e . Tem porom andibular j oint disc. Magnet ic resonance im aging.
Mu-Qing LIU1,2,3
Jie LEI1,2,3
Jian-Hui HAN1,2,3
Adrian U-Jin YAP4,5,6
Kai-Yuan FU1,2,3
http://dx.doi.org/10.1590/1678-7757-2016-0471
1Peking University School & Hospital of Stomatology, Center for TMD & Orofacial Pain and
Department of Oral & Maxillofacial Radiology, Beijing, China.
2National Engineering Laboratory for Digital and Material Technology of Stomatology, Beijing, China. 3Beijing Key Laboratory of Digital Stomatology, Beijing, China.
4Ng Teng Fong General Hospital, Department of Dentistry, Jurong Health Services, Singapore,
Singapore.
5SIM University, School of Science and Technology, Singapore, Singapore. 6National University of Singapore, Faculty of Dentistry, Singapore, Singapore.
Corresponding address: Kai-Yuan Fu Center for TMD & Orofacial Pain and Department of Oral & Maxillofacial Radiology. Peking University School & Hospital of Stomatology. No. 22 Zhong Guan Cun South Ave. Beijing 100081 - P.R. China. Phone: 86-10-82195342 - Fax: 86-10-62173402.
I nt roduct ion
Tem porom andibular j oint ( TMJ) disc displacem ent
is t he m ost com m on t y pe of TMJ ar t hr opat hy and
involves an abnorm al relat ionship or m isalignm ent of
t he art icular disc relat ive t o t he condyle. The usual
dir ect ion for displacem ent of t he disc is ant er ior ly
or an t er ior - m ed ially2 9. I n sp it e of t h eir ap p ar en t
ef f i ca cy a n d w i d esp r ea d u se f o r t r ea t i n g TMD,
t h e p r ecise m ech an ism s of act ion of or al sp lin t s
rem ain cont roversial10. Hypot heses proposed include
reposit ioning of condyle and/ or art icular disc, reduct ion
LQPDVWLFDWRU\PXVFOHDFWLYLW\PRGL¿FDWLRQRISDWLHQW¶V
parafunct ional behaviours, and changes in pat ient ’s
occlusion6. Tw o com m on t ypes of oral splint s used
in clinical pract ice are t he st abilizat ion and ant erior
reposit ioning splint s.
Ant er ior r eposit ioning splint s ( ARS) hav e been
show n t o be effect ive for t he m anagem ent of
disc-co n d y l e d i so r d er s1 4 , 1 8 , 2 6. Al so k n o w n as an t er i o r
p osit ion in g ap p lian ces or m an d ib u lar or t h op ed ic
r eposit ion in g applian ces, t h ey ser v e t o dir ect t h e
m andibular condy le ant er ior ly in t he glenoid fossa
( i.e., pr ot r usive m andibular posit ion) . The pur pose
of ARS t reat m ent is not t o alt er t he condylar posit ion
perm anent ly, but t o change it during t he t reat m ent t o
help t he adapt ion of t he ret rodiscal t issues24. Based
on clinical and MRI assessm ent s, approxim at ely 70%
of reducing displaced discs was capt ured w it h t he use
of ARS18. ARS could also alt er m echanical st resses
on t he TMJ arising from t he im m ediat e physiologic
im provem ent in t he disc- condyle relat ionship4 and has
been shown t o facilit at e regenerat ive rem odeling of t he
TMJ22. Alt hough t he recapt ured discs can occasionally
m ov e back w ar d w it h su ccessfu l ARS t h er apy, t h e
am ount of disc m ovem ent was found t o be negligible19.
The im provedcondyle- disc relat ionship w it h ARS was
t hought t o be achieved prim arily by t he ant eroinferior
m ovem ent of t he condyle.
St abilizat ion splint s ( SS) cover all t he m axillary
and m andibular t eet h and are used t o t reat bot h j oint
and m ast icat ory m uscle disorders2,17. I n cont rast t o
ARS, SS are perm issive appliances ( allow s for t eet h
t o glide unim peded over t he bit ing surface) and do
not prot rude t he m andible. They serve t o provide a
t em porary and rem ovable ideal occlusion at increased
ver t ical dim ension and cent r ic r elat ion. The use of
SS in cr eases TMJ sp ace1 2 an d allow s f or an t er
o-inferior m ovem ent of t he condyles7,11,16. SS are also
used t o m anage disc- condy le disor der s3. They ar e
effect ive in elim inat ing t he signs/ sym pt om s of TMD,
except TMJ clicking28. When com pared t o ARS for t he
t r eat m ent of TMJ DDw R, r educt ion in dy sfunct ion
and TMJ sym pt om s w ere found t o be low er w it h SS
t herapy5,25,27.
The m echanism of act ion of bot h ARS and SS
r em ains lar gely hy pot het ical. The t w o oral splint s
w it h t heir variance in bit e and m andibular posit ioning
can pr oduce differ ent degr ees of disc and condy le
posit ional changes, w hich in t urn can affect t reat m ent
out com e. Most previous MRI st udies w ere conduct ed
on a single splint design w it h t he bet w een- subj ect
m et hod. Thus far, few st udies have com pared t he t w o
splint designs using a w it hin- subj ect approach ( every
single part icipant is subj ect ed t o every single splint
design) and at st andardized vert ical dim ension. This
st udy aim ed t o evaluat e t he effect s of bit e posit ions
charact erizing ARS and SS t herapy ( w it h and w it hout
ant er ior m ovem ent ) on disc/ condy le locat ions and
disc- condy le r elat ions in pat ient s w it h TMJ DDw R,
using MRI m et rical analysis.
Mat erial and Met hods
Pat ient s
A t ot al of 37 pat ient s, wit h a m ean age of 18.8± 4.3
years ( ranging from 12 t o 30 years, 7 m ale and 30
fem ale) and w it h com plaint s of TMJ clicking and/ or
int erm it t ent locking, w ere recruit ed. All pat ient s had
perm anent dent it ion, free of TMD- relat ed pain, and 16
were younger t han 18 years of age. To lessen t he effect
of confounding variables including m arked skelet al/
occlu sal d iscr ep an cies an d sy st em at ic d iseases,
exclusion cr it er ia w er e as follow s: Pr esence of ( 1)
crossbit es and open bit es; ( 2) deep overbit es ( vert ical
overlap of t he m axillary cent ral incisors > 1/ 2 of t he
m andibular cent ral incisors) ; ( 3) large overj et s ( > 5
m m ) ; ( 4) rheum at ic or degenerat ive j oint diseases.
The st udy was approved by t he Biom edical I nst it ut ional
Review Board. Writ t en inform consent was obt ained
from all part icipat ing subj ect s.
Fift y- one ( out of 74) j oint s of t he 37 pat ient s w ere
clinically diagnosed w it h DDw R using t he RDC/ TMD9.
Bilat eral DDw R was obser ved in 14 pat ient s. Upon
MRI exam inat ion, 9 of t he 23 clinically asym pt om at ic
j oint s w ere also diagnosed w it h DDw R, based on t he
ZLWKFOLQLFDOGLDJQRVLVRI''Z5ZHUHDOOFRQ¿UPHGE\
MRI exam inat ion. Thus, a t ot al of 60 j oint s wit h DDwR
w ere included in t his st udy. 4 asym pt om at ic j oint s
w ere diagnosed w it h DDw oR and 10 j oint s w ere found
t o be norm al w it h bot h clinical and MRI assessm ent .
Det erm inat ion of bit e and m andibular posit ions
The condyle and disc locat ions w ere assessed in
t hree bit e posit ions: Posit ion 1: m axim al int ercuspat ion
( MI CP) ; Posit ion 2 : ch ar act er izin g ARS p osit ion ;
Posit ion 3: charact erizing SS posit ion ( Figure 1) . For
Posit ion 1, subj ect s w er e asked t o bit e t heir back
t eet h com plet ely t oget her. The dist ance bet w een t he
gingival m argins of t he left upper and low er cent ral
incisors ( D1) and t he overj et of t he left upper cent ral
i n ci so r w er e r eco r d ed u si n g a cal i p er ( Gu an g l u
SF2000, Guangx i, China) . For Posit ion 2, subj ect s
w er e asked t o open t heir m out hs fully beyond t he
clicking point and inst ruct ed t o close in a prot ruded
posit ion w it h t he incisors in an edge- t o- edge relat ion.
Th e m an d ib u lar p osit ion w as r eg ist er ed u sin g a
silicone bit e r egist rat ion m at er ial ( Occlufast Rock ,
Z h er m ack , Rov ig o, I t aly ) . Th e d ist an ce b et w een
t h e gin giv al m ar gin s of t h e lef t u pper an d low er
cent ral incisors ( D2) was det erm ined. For Posit ion 3,
subj ect s w ere asked t o open fully beyond t he clicking
point and guided int o t he m ost r et r uded/ r ear m ost
m andibular locus. This was repeat ed several t im es t ill
a reproducible “ cent ric” relat ion posit ion was achieved
at t he dist ance D2 w it hout prot rusion and regist ered.
The dist ance bet w een t he gingival m argins of t he left
upper and low er cent ral incisors ( D3) and t he overj et
of t he left upper cent ral incisor w ere again recorded.
All bit e regist rat ions and m andibular m easurem ent s
w ere m ade by a single invest igat or.
Magnet ic Resonance I m aging
MRI was perform ed w it h a 1.5-Tesla MR scanner
( NOVUS, Siem ens, Munich, Germ any) wit h TMJ surface
coils. Subj ect s w ere placed supine w it h t heir heads
posit ioned w it h t he Frankfurt plane perpendicular t o
WKHÀRRU7KHFHQWHUEHDPZDVWKHQOLQHGXSZLWKWKH
sagit t al plane. All j oint s w ere scanned in t he t hree
m andibular posit ions in single visit using a fact orial
design or der. For Posit ions 2 and 3, subj ect s w er e
direct ed t o open t heir m out hs fully beyond t he clicking
point and gent ly close/ bit e int o t he pr epar ed bit e
regist rat ions. An init ial low- resolut ion T1- weight ed ( TR
300 m s; TE 10 m s) axial localizing scan was follow ed
by Prot on- w eight ed ( TR 1760 m s, TE 15 m s) oblique
sagit t al scan acquired vert ical t o t he long axis of each
FRQG\OH7KH¿HOGRIYLHZZDVîFPDQGPDWUL[ VL]H ZDV î 6OLFH WKLFNQHVV DQG LQWHUVOLFH
spacing w ere set at 2 m m and 1 m m , respect ively.
Met rical and st at ist ical analysis
The im ages w ere analyzed using im age analysis
soft ware ( Volview 3.4, Kit ware, New York) . The slice
t hrough t he cent er of t he horizont al long axis of t he
condyle was select ed for evaluat ion ( Figure 1) . The
disc- condyle angle was det erm ined according t o t he
m et hod descr ibed by Drace and Enzm ann8 ( 1990)
( Figure 2A) . The norm al range for disc- condyle angle is
EHWZHHQíWR1. Joint s wit h disc- condyle angles
great er t han 15° are considered t o have ant erior disc
displacem ent .
X- Y co o r d i n a t e m ea su r em en t s w er e u sed t o
det er m ine disc and condy le posit ions ( Figur e 2B) .
The condyle and disc posit ions w ere expressed as C
and D point coordinat es ( x, y) , respect ively. The MRI
dat a w ere evaluat ed by a t rained radiologist w ho was
blinded t o clinical inform at ion. I nt ra- class correlat ion
FRHI¿FLHQWV,&&ZHUHXVHGWRGHWHUPLQHWKHLQWUD
and int er- observer reliabilit y. A m ean int ra- observer
I CC of > 0.900 was est ablished for all variables ( t he
r ad iolog ist m ad e all m easu r em en t s t w ice w it h a
one- w eek int erval) . I nt er- observer I CC ranged from
0.868 t o 1 for t he different variables. The lat t er was
det erm ined wit h t he assist ance of anot her independent
radiologist w ho was also blinded t o pat ient s’ clinical
dat a.
Disc and condyle X-Y coordinat es and disc- condyle
angles for Posit ions 1, 2, and 3 w ere com pared. SPSS
version 20 ( SPSS I BM, Chicago, USA) was used for
st at ist ical analysis. Dat a was subj ect ed t o one- way
$129$/6'DQGWWHVWDWVLJQL¿FDQFHOHYHOP v alu es
< 0.05.
Result s
Mandibular posit ion
The average vert ical dist ance bet ween t he gingival
m argins of left upper and low er cent ral incisors was
1 4 . 2 ± 2 . 0 m m in Posit ion 1 an d 1 6 . 9 ± 2 . 0 m m in
Posit ions 2 and 3. The average over j et of t he left
upper cent ral incisor was 3.1± 1.1 m m in Posit ion 1
and 3.0± 1.2 m m in Posit ion 3. Posit ion 2 t hus post ured
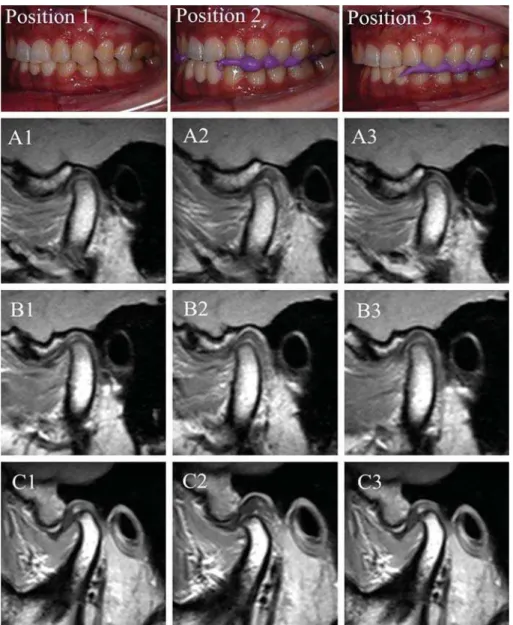
Figure 1- Representative MRIs of three joints in Position 1 (ICP – column 1), Position 2 (ARS – column 2), and Position 3 (SS – column 3). Joint A was normal while Joints B and C were diagnosed with DDwR
Figure 2- A: Drace’s measurement for disc-condyle angle. C point estimated the center of the condylar head. Line 1 was drawn from C point perpendicular to the Frankfort horizontal plane. Line 2 was drawn through C point to the midpoint of the posterior margin of
WKH SRVWHULRU EDQGRIWKH GLVF ' SRLQW7KH DQJOH EHWZHHQ OLQH DQGOLQH ZDV GH¿QHG DV WKH GLVFFRQG\OH DQJOH %&RRUGLQDWH
3 m oved t he m andible only dow nward w it h reference
t o Posit ion 1.
Disc- condyle angle
Disc- condy le angle in nor m al and DDw R j oint s
for Posit ions 1 t o 3 are show n in Table 1. I n norm al
MRLQWVQ QRVLJQL¿FDQWGLIIHUHQFHLQGLVFFRQG\OH
an gle w as obser v ed bet w een t h e t h r ee posit ion s
(P> 0.05) . Disc- condyle angle was w it hin t he norm al
UDQJHía,QMRLQWVZLWK''Z5Q
m ean disc- condyle angle was reduced from 53.4° in
3RVLWLRQWRíLQ3RVLWLRQDQGLQ3RVLWLRQ
3. The percent age of displaced disc reduct ion or disc
³UHFDSWXUH´SRVWWUHDWPHQWDQJOHEHWZHHQíDQG
+ 15° ) in DDw R j oint s was 96.7% ( 58/ 60 j oint s) for
Posit ion 2 and 33.3% ( 20/ 60 j oint s) for Posit ion 3
(P< 0.001) . The average disc- condyle angle of DDw oR
j oint s ( n= 4) in Posit ions 1, 2, and 3 were 82.1° , 65.5° ,
DQG UHVSHFWLYHO\ 1R VLJQL¿FDQW GLIIHUHQFH LQ
disc- condyle angle was observed bet w een t he t hree
posit ions (P> 0.05) .
Coordinat e m easurem ent s of condyle and disc
C point s represent ing condylar posit ions in X- and
Y- axis are show n in Table 2. C point m ovem ent s w ere
indicat ed by t he num erical difference of coordinat e
valu es bet w een t w o poin t s. I n n or m al j oin t s, t h e
condyle m oved 2.22 m m forward and 1.49 dow nward
fr om Posit ion 1 t o Posit ion 2, and shift ed 0.7 m m
f or w ar d an d 0 . 0 6 m m dow nw ar d f r om Posit ion 1
t o 3. I n j oint s w it h DDw R, t he condyle m oved 3.28
m m for war d and 2.6 m m dow nwar d fr om Posit ion
1 t o 2, and shift ed 0.97 m m forward and 0.68 m m
dow nward from Posit ion 1 t o Posit ion 3. St at ist ical
DQDO\VLVLQGLFDWHGDVLJQL¿FDQWO\JUHDWHUIRUZDUGDQG
downward m ovem ent of t he condyle wit h ARS posit ion
w hen com pared t o t he SS posit ion.
D point s ( post erior m argin of t he post erior band of
disc) represent ing disc posit ions in t he X- and Y- axis
are also present ed in Table 2. I n norm al j oint s, t he D
point was locat ed 1.21 m m behind and 1.70 m m below
t he G point ( t he highest point of glenoid fossa) . The
disc m oved 0.93 m m forward and 0.64 m m downward
f r om Posit ion 1 t o Posit ion 2 , w h ile t h e con d y le
m oved forward and dow nward. The disc did not m ove
VLJQL¿FDQWO\IURP3RVLWLRQWR3RVLWLRQLQQRUPDO
j oint s. I n DDw R j oint s, t he disc was locat ed 2.02 m m
ant erior and 2.81 m m below t he G point in Posit ion 1,
LQGLFDWLQJLWZDVVLJQL¿FDQWO\GLVSODFHGDQWHULRUO\DQG
inferiorly w hen com pared t o norm al j oint s ( Table 2) .
I n cont rast t o norm al j oint s, t he disc m oved 2.23m m
backward from Posit ions 1 t o 2 in DDw R j oint s. Disc
m ovem ent from Posit ion 1 t o 3 was, how ever, only
0.75 m m backward. The coordinat e values of D point
in bot h X- and Y- axis for Posit ion 2 in DDw R j oint s
w ere sim ilar t o norm al j oint s, indicat ing t hat t he disc
was fully reduced in t he prot rusive posit ion. For all t he
PHDVXUHPHQWVQRVLJQL¿FDQWGLIIHUHQFHZDVGHWHFWHG
Positions Normal joints(n=10) DDwR joints(n=60)
Position 1 ía a
Position 2 í íA
Position 3 ía a,A
/RZHUFDVHOHWWHUVLQWKHVDPHURZLQGLFDWHVLJQL¿FDQWGLIIHUHQFHEHWZHHQWZRJURXSVS 8SSHUFDVHOHWWHUVLQWKHVDPHFROXPQLQGLFDWHVLJQL¿FDQWGLIIHUHQFHEHWZHHQWZRSRVLWLRQVS
Table 1-'LVFFRQG\OHDQJOHVIRUWKHWKUHHSRVLWLRQVLQQRUPDODQG''Z5MRLQWVPHDQ6'
Coordinates Condyle Disc
Normal joints (mm, mean±SD)
DDwR joints (mm, mean±SD)
Normal joints (mm, mean±SD)
DDwR joints (mm, mean±SD)
X coordinate Position 1 a,A a,A b,A íb,A
Position 2 íA,B íA A A
Position 3 B A a ía,A
Y coordinate Position 1 ía,C ía,B íb,B íb
Position 2 íC,D íB ía,B,C ía
Position 3 íD íB ía,C ía
/RZHUFDVHOHWWHUVLQWKHVDPHURZLQGLFDWHVLJQL¿FDQWGLIIHUHQFHEHWZHHQWZRJURXSVS 8SSHUFDVHOHWWHUVLQWKHVDPHFROXPQLQGLFDWHVLJQL¿FDQWGLIIHUHQFHEHWZHHQWZRSRVLWLRQVS
bet w een adolescent and adult pat ient s.
Discussion
I n t his st udy, w e det erm ined t he spat ial changes
in disc and condy le posit ions and t he disc- condy le
r elat ion w it h m andibular posit ions of ARS and SS
t herapy in adolescent s and adult s. Met rical analysis
was done w it h MRI , as it is a non- invasive diagnost ic
m et hod t hat enables bot h qualit at ive and quant it at ive
evaluat ion of t he st ruct ures w it hin t he j oint , including
t he TMJ disc. I t is also generally painless and does not
involve t he use of ionizing radiat ion. As splint t hickness
can affect disc and condyle posit ions, a sim ilar vert ical
d im en sion w as m ain t ain ed f or b ot h ARS an d SS
posit ions in t his st udy. The use of m andibular posit ions
m im icking ARS and SS inst ead of act ual appliances
n egat ed t h e con f ou n din g ef f ect s of t ech n ical an d
clinical discrepancies associat ed wit h splint fabricat ion,
adj ust m ent , and use. The m easurem ent m et hod of
disc- condyle angle and posit ions of condyle/ disc was
reliable and reproducible.
I n t h e m a x i m a l i n t e r cu sp a t i o n ( Po si t i o n 1 ) ,
t h e disc in DDw R j oin t s w as displaced an t er ior ly
an d in f er ior ly, w h ile t h e con d y le w as p osit ion ed
backward and upward, in relat ion t o norm al j oint s.
7KLVFRUURERUDWHGWKH¿QGLQJVRIHDUOLHUVWXGLHV13,20.
The condyle m oved forward and dow nward in bot h
ARS and SS t reat m ent posit ions ( Posit ions 2 and 3,
UHVSHFWLYHO\EXWPRYHPHQWZDVPRUHVLJQL¿FDQWZLWK
ARS. The m echanism of act ion of ARS was previously
t hought t o involve t he “ recapt uring” of t he discs, since
t he condyles are m oved dow nward and forward. I t
was believed t hat t he disc- condyle com plex could be
gradually walked back int o t he fossa by adj ust ing t he
bit ing surface of ARS23. Kurit a, et al.19 ( 1998) found
t h at appr ox im at ely 6 0 % of t h e “ r ecapt u r ed” disc
m oved post eriorly, but t he am ount of m ovem ent was
m inor. I n our st udy, disc m ovem ent was not iceably
large ( 2.23 m m post eriorly) in j oint s w it h DDw R for
t he ARS posit ion. The D point ( post erior band of t he
disc) act ually shift ed back t o t he G point ( highest point
of t he glenoid fossa) , indicat ing com plet e reduct ion
of t he displaced disc. I n cont rast , t he displaced disc
only m oved back 0.75 m m for t he SS posit ion. The
r educt ion of t he displaced disc w it h ARS m ight be
one of t he key fact or s t o t he adapt ion and r epair
of t he r et r odiscal t issues. The elim inat ion of j oint
click in g is com m on ly u sed t o h elp det er m in e t h e
appropriat e m andibular posit ion for ARS19,26. I n t his
st udy, t he ant ero- inferior m ovem ent of t he m andible
for elim inat ion of j oint clicking is usually less t han t he
prot ruded posit ion wit h t he incisors in an edge- t o- edge
relat ion. There m ay be a link bet w een reduct ion of
t he displaced disc and t he forward m ovem ent of t he
condyle. The st abilit y of t he reduced disc posit ion,
how ever, depends on m aint aining t he condyles in t he
forward and downward posit ion, necessit at ing t he
full-t im e use of ARS over a period of full-t im e. Upon sfull-t opping
ARS use, reduced discs m ay once again get displaced,
as t he condyle m oves post eriorly.
A proper disc- condyle- fossa relat ionship is t hought
t o be im port ant for norm al TMJ funct ion, alleviat ing
j oint pain, pr event ing degenerat ive j oint changes,
and prom ot ing m andible grow t h in adolescent s15,21.
Alt hough som e j oint s w it h DDw R achieved nor m al
disc- condyle relat ionship in t he SS posit ion ( increased
vert ical w it hout m andibular ant erior posit ioning) , t he
SHUFHQWDJHRIGLVFUHGXFWLRQZDVVLJQL¿FDQWO\ORZHU
t han w it h ARS ( 33% as opposed t o 96.7% w it h ARS) .
Use of ARS achieved an im m ediat e physiologic
disc-condyle- fossa relat ionship and increased t he prospect
of disc reduct ion. This explains in part t heir superior
effect iveness in decreasing pain and dysfunct ion in
pat ient s w it h DDw R w hen com pared t o SS5,25,27.
As w it h all st u d ies, t h e cu r r en t r esear ch h as
som e lim it at ions. Since act ual oral splint s w ere not
IDEULFDWHG WKH LQÀXHQFH RI VSOLQW PDWHULDO VWLIIQHVV
on disc and condyle posit ions/ relat ionships could not
be ascer t ained. The long t er m effect s of ARS and
SS on disc- con dy le- f ossa r elat ion sh ips w er e also
QRW GHWHUPLQHG 3DWLHQWV ZLWK VLJQL¿FDQW VNHOHWDO
d i scr e p a n ci e s, m a l o ccl u si o n , a n d r h e u m a t i c o r
degenerat iv e j oint diseases w er e ex cluded, w hich
m ay also affect disc “ recapt ure” in j oint s w it h DDw R.
Conclusions
I n sum m ary, ant erior reposit ioning of t he m andible
im pr oved t he spat ial r elat ionship bet w een t he disc
and condyle, increasing t he prospect of disc reduct ion
in pat ient s w it h DDw R. I n addit ion t o ant erior and
inferior m ovem ent of t he condyle, t ransit ory post erior
m ovem ent of t he disc also occurs w it h t he ant erior
References
1- Ahm ad M, Hollender L, Anderson Q, Kart ha K, Ohrbach R, Truelove
EL, et al. Research diagnost ic crit eria for t em porom andibular disorders
( RDC/ TMD) : developm ent of im age analy sis cr it er ia and ex am iner
reliabilit y for im age analysis. Oral Surg Oral Med Oral Pat hol Oral Radiol
Endod. 2009; 107: 844- 60.
2- Al- Ani Z, Gray RJ, Davies SJ, Sloan P, Glenny AM. St abilizat ion splint
t herapy for t he t reat m ent of t em porom andibular m yofascial pain: a
syst em at ic review. J Dent Educ. 2005; 69: 1242- 50.
3- Badel T, Marot t i M, Kern J, Laskarin M. A quant it at ive analysis of
splint t herapy of displaced t em porom andibular j oint disc. Ann Anat .
2009; 191: 280- 7.
4- Boero RP. The physiology of splint t herapy: a lit erat ure review. Angle
Ort hod. 1989; 59: 165- 80.
5- Cont i PC, Miranda JE, Cont i AC, Pegoraro LF, Araúj o CR. Part ial
t im e use of ant erior reposit ioning splint s in t he m anagem ent of TMJ
pain and dysfunct ion: a one- year cont rolled st udy. J Appl Oral Sci.
2005; 13( 4) : 345- 50.
6- Dao TT, Lavigne GJ. Oral splint s: t he crut ches for t em porom andibular
disorders and bruxism ? Crit Rev Oral Biol Med. 1998; 9: 345- 61.
7- Dem ling A, Fauska K, I sm ail F, St iesch M. A com parison of change
in condylar posit ion in asym pt om at ic volunt eers ut ilizing a st abilizat ion
and a pivot appliance. Cranio. 2009; 27: 54- 61.
'UDFH-((Q]PDQQ'5'H¿QLQJWKHQRUPDOWHPSRURPDQGLEXODU j oin t : closed - , p ar t ially op en - , an d op en - m ou t h MR im ag in g of
asym pt om at ic subj ect s. Radiology. 1990; 177: 67- 71.
9 - D w o r k i n SF, Le Re sch e L. Re se a r ch d i a g n o st i c cr i t e r i a f o r
t em por om andibular disor der s: r ev iew, cr it er ia, ex am inat ions and VSHFL¿FDWLRQVFULWLTXH-&UDQLRPDQGLE'LVRUG 10- Dylina TJ. A com m on- sense approach t o splint t herapy. J Prost het
Dent . 2001; 86: 539- 45.
11- Ekberg EC, Sabet ME, Pet ersson A, Nilner M. Occlusal appliance
t herapy in a short- t erm perspect ive in pat ient s wit h t em porom andibular
d i so r d e r s co r r e l a t e d t o co n d y l e p o si t i o n . I n t J Pr o st h o d o n t .
1998; 11: 263- 8.
12- Et t lin DA, Mang H, Colom bo V, Palla S, Gallo LM. St ereom et ric
assessm ent of TMJ space variat ion by occlusal splint s. J Dent Res.
2008; 87: 877- 81.
13- Gat eno J, Anderson PB, Xia JJ, Horng JC, Teichgraeber JF, Liebschner
MA. A com parat ive assessm ent of m andibular condylar posit ion in
pat ient s w it h ant erior disc displacem ent of t he t em porom andibular
j oint . J Oral Maxillofac Surg. 2004; 62: 39- 43.
*|NDOS + 7XUNNDKUDPDQ + &KDQJHV LQ SRVLWLRQ RI WKH t em por om andibular j oint disc and condy le aft er disc r eposit ioning
appliance t herapy: a funct ional exam inat ion and m agnet ic resonance
im aging st udy. Angle Ort hod. 2000; 70: 400- 8.
+DOO+',QWUDDUWLFXODUGLVFGLVSODFHPHQW3DUW,,,WVVLJQL¿FDQW r ole in t em por om andibular j oint pat hology. J Oral Maxillofac Sur g.
1995; 53: 1073- 9.
16- Hasegawa Y, Kakim ot o N, Tom it a S, Honda K, Tanaka Y, Yagi K, et
al. Movem ent of t he m andibular condyle and art icular disc on placem ent
of an occlusal splint . Oral Surg Oral Med Oral Pat hol Oral Radiol Endod.
2011; 112: 640- 7.
17- Jokst ad A, Mo A, Krogst ad BS. Clinical com parison bet w een t w o
different splint designs for t em porom andibular disorder t herapy. Act a
Odont ol Scand. 2005; 63: 218- 26.
18- Kurit a H, Kurashina K, Baba H, Oht suka A, Kot ani A, Kopp S.
Evaluat ion of disk capt ure wit h a splint reposit ioning appliance: clinical
and crit ical assessm ent w it h MR im aging. Oral Surg Oral Med Oral
Pat hol Oral Radiol Endod. 1998; 85: 377- 80.
19- Kurit a H, Kurashina K, Oht suka A, Kot ani A. Change of posit ion of
t he t em porom andibular j oint disk w it h insert ion of a disk- reposit ioning
ap p l i an ce. Or al Su r g Or al Med Or al Pat h ol Or al Rad i ol En d od .
1998; 85: 142- 5.
2 0 - Ku r it a H, Oh t su k a A, Kobayash i H, Ku r ash in a K. A st u dy of
t h e r elat ion sh ip bet w een t h e posit ion of t h e con dy lar h ead an d
displacem ent of t he t em porom andibular j oint disk. Dent om axillofac
Radiol. 2001; 30: 162- 5.
21- Kurit a H, Uehara S, Yokochi M, Nakat suka A, Kobayashi H, Kurashina
K. A long- t erm follow- up st udy of radiographically evident degenerat ive
changes in t he t em porom andibular j oint wit h different condit ions of disk
displacem ent . I nt J Oral Maxillofac Surg. 2006; 35( 1) : 49- 54.
2 2 - Li u MQ, Ch e n HM, Ya p AU, Fu KY. Co n d y l a r r e m o d e l i n g
accom panying splint t herapy: a cone- beam com put erized t om ography
st udy of pat ient s wit h t em porom andibular j oint disk displacem ent . Oral
Surg Oral Med Oral Pat hol Oral Radiol. 2012; 114: 259- 65.
2 3 - M o l o n e y F, H o w a r d JA . I n t e r n a l d e r a n g e m e n t s o f t h e
t em por om andibular j oint . I I I . Ant er ior r eposit ioning splint t herapy.
Aust Dent J. 1986; 31: 30- 9.
24- Okeson JP. Managem ent of t em por om andibular disor der s and
occlusion. 7t h ed. Saint Louis: Mosby; 2012.
25- Sant acat t erina A, Paoli M, Peret t a R, Bam bace A, Belt ram e A. A
com parison bet w een horizont al splint and reposit ioning splint in t he
t reat m ent of “ disc dislocat ion wit h reduct ion”. Lit erat ure m et a- analysis.
J Oral Rehabil. 1998; 25( 2) : 81- 8.
2 6 - Sim m on s HC 3r d, Boar d of Dir ect or s, Am er ican Academ y of
Cr an iof acial Pain . Gu idelin es f or an t er ior r eposit ion in g applian ce
t herapy for t he m anagem ent of craniofacial pain and TMD. Cranio.
2005; 23: 300- 5.
27- Tecco S, Fest a F, Salini V, Epifania E, D'At t ilio M. Treat m ent of
j oint pain and j oint noises associat ed w it h a r ecent TMJ int er nal
derangem ent : a com parison of an ant erior reposit ioning splint , a
full-arch m axillary st abilizat ion splint , and an unt reat ed cont rol group.
Cranio. 2004; 22: 209- 19.
28- Wassell RW, Adam s N, Kelly PJ. The t reat m ent of t em porom andibular
disorders w it h st abilizing splint s in general dent al pract ice: one- year
follow- up. J Am Dent Assoc. 2006; 137: 1089- 98.
2 9 - Why t e AM, McNam ar a D, Rosen ber g I , Why t e AW. Magn et ic
resonance im aging in t he evaluat ion of t em porom andibular j oint disc
displacem ent - a r ev iew of 144 cases. I nt J Oral Max illofac Sur g.