ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Recommendations
of
the
Brazilian
Society
of
Rheumatology
for
the
induction
therapy
of
ANCA-associated
vasculitis
Alexandre
Wagner
Silva
de
Souza
a,∗,
Ana
Luisa
Calich
a,
Henrique
de
Ataíde
Mariz
b,
Manuella
Lima
Gomes
Ochtrop
c,
Ana
Beatriz
Santos
Bacchiega
c,
Gilda
Aparecida
Ferreira
d,
Jozelia
Rêgo
e,
Mariana
Ortega
Perez
f,
Rosa
Maria
Rodrigues
Pereira
f,
Wanderley
Marques
Bernardo
g,
Roger
Abramino
Levy
caUniversidadeFederaldeSãoPaulo(UNIFESP),EscolaPaulistadeMedicina(EPM),DisciplinadeReumatologia,SãoPaulo,SP,Brazil bUniversidadeFederaldePernambuco(UFPE),DisciplinadeReumatologia,Recife,PE,Brazil
cUniversidadedoEstadodoRiodeJaneiro(UERJ),HospitalUniversitárioPedroErnesto,Servic¸odeReumatologia,RiodeJaneiro,RJ,Brazil dUniversidadeFederaldeMinasGerais(UFMG),FaculdadedeMedicina,DepartamentoAparelhoLocomotor,BeloHorizonte,MG,Brazil eUniversidadeFederaldeGoiás(UFG),FaculdadedeMedicina,Servic¸odeReumatologia,Goiânia,GO,Brazil
fUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,DisciplinadeReumatologia,SãoPaulo,SP,Brazil gAssociac¸ãoMédicaBrasileira(AMB),ProjetoDiretrizes,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Keywords:
ANCA-associatedvasculitis Granulomatosiswithpolyangiitis Microscopicpolyangiitis Renal-limitedvasculitis Guidelines
a
b
s
t
r
a
c
t
Thepurposeoftheserecommendationsistoguidetheappropriateinductiontreatment ofantineutrophilcytoplasmic antibody-associatedvasculitis (AAV)patients withactive disease.TherecommendationsproposedbytheVasculopathiesCommitteeofthe Brazil-ianSocietyRheumatologyforinduction therapyofAAV,includinggranulomatosis with polyangiitis,microscopicpolyangiitisandrenal-limitedvasculitis,werebasedon system-aticliteraturereviewandexpertopinion.LiteraturereviewwasperformedusingMedline (PubMed),EMBASEandCochranedatabasetoretrievearticlesuntilOctober2016.PRISMA guidelineswereusedforthesystematicreviewandarticleswereassessedaccordingtothe Oxfordlevelsofevidence.Sixteenrecommendationsweremaderegardingdifferentaspects ofinductiontherapyforAAV.Thepurposeoftheserecommendationsistoserveasaguide fortherapeuticdecisionsbyhealthcareprofessionalsinthemanagementofAAVpatients presentingactivedisease.
©2017PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](A.W.Souza).
http://dx.doi.org/10.1016/j.rbre.2017.06.003
Recomendac¸ões
da
Sociedade
Brasileira
de
Reumatologia
para
a
terapia
de
induc¸ão
para
vasculites
associadas
ao
ANCA
Palavras-chave:
VasculiteassociadaaANCA Granulomatosecompoliangiite Poliangiitemicroscópica Vasculitelimitadaaorim Diretrizes
r
e
s
u
m
o
O objetivo destas recomendac¸ões é orientar o tratamento apropriado de induc¸ão em pacientescomvasculitesassociadasaanticorposanticitoplasmadeneutrófilos(VAA)ativa. As recomendac¸õespropostas pelo Comitê de Vasculopatiasda Sociedade Brasileira de Reumatologiaparaaterapiadeinduc¸ãoparaVAA,incluindogranulomatosecom poliangi-ite,poliangiitemicroscópicaevasculitelimitadaaorim,forambaseadasemumarevisão sistemáticadaliteraturaenaopiniãodeespecialistas.Arevisãodaliteraturafoifeitacomas basesdedadosMedline(PubMed),EmbaseeCochraneparaconsultarartigosatéoutubrode 2016.AsdiretrizesPrisma(PreferredReportingItemsforSystematicReviewsandMeta-Analyses
–Principaisitensparareportarrevisõessistemáticasemetanálises)foramusadaspara arevisãosistemáticaeosartigosforamavaliadosdeacordocomosníveisdeevidência Oxford.Dezesseisrecomendac¸õesforamfeitasemrelac¸ãoadiferentesaspectosda ter-apiadeinduc¸ãoparaVAA.Oobjetivodessasrecomendac¸õeséservircomoumguiapara decisõesterapêuticasporprofissionaisdasaúdenotratamentodepacientescomVAAque apresentemadoenc¸aativa.
©2017PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Antineutrophilcytoplasmicantibody(ANCA)-associated vas-culitis(AAV)isagroupofnecrotizingsystemicvasculitisthat affectspredominantlysmallvesselswithfewornoimmune deposits at vesselswall, associated with ANCA as a com-mon biomarker.1 ANCA are antibodies againstenzymes in
azurophilicgranulesofneutrophilsandlysosomesof mono-cytes with specificity for proteinase-3 (PR3-ANCA) and for myeloperoxidase(MPO-ANCA).2 AAV includes
granulomato-sis with polyangiitis (GPA, previously known as Wegener’s granulomatosis),microscopicpolyangiitis(MPA),eosinophilic granulomatosiswithpolyangiitis(EGPA,previouslyknownas Churg-Strausssyndrome)andorgan-limitedAAV,forexample renallimitedvasculitis(RLV).1
BeforestartingtherapyforAAVpatientsatonsetespecially GPAandMPA,itisnecessarytodeterminediseaseextension. TheEuropeanVasculitisStudy(EUVAS)classification catego-rizesdiseaseextensionintofivedifferentsubsetsasfollows: localizeddisease,earlysystemicdisease,generalizeddisease, severe disease and refractory disease (Table 1).3 However,
managementofanewlydiagnosedAAVpatientmaybealso plannedbasedonthepresenceoforgan/lifethreatening dis-easeornotorwhetherthereisrapidlyprogressiverenalfailure orpulmonaryhemorrhage.4Themainoutcomemeasuresfor
theassessmentofAAVdiseaseactivityarethethirdversion ofthe BirminghamVasculitis ActivityScore(BVAS)andthe BVAS-WGwhichwasadaptedforGPApatients.5,6
TheAAVtreatment isdivided ininductionand mainte-nancetherapy.Induction therapyisprescribed forpatients with active disease, either at disease onset or at disease relapsesduringfollow-up;itspurposeistoattaincomplete remissionandtoavoiddamageaccrual.Afterachieving remis-sion,maintenancetherapyisstartedanditsgoalistoprevent diseaserelapses.7
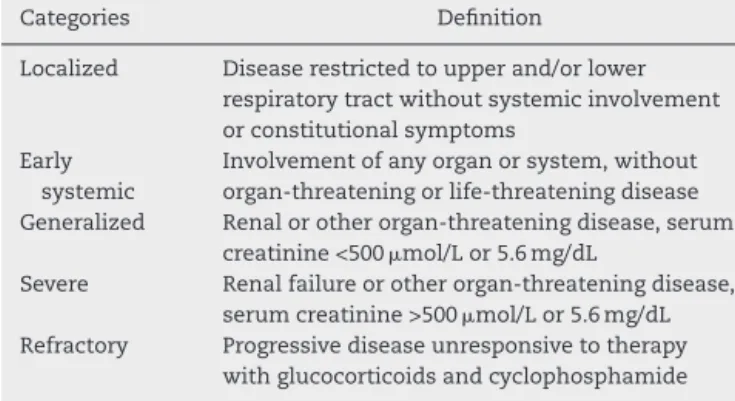
Table1–EUVASdiseasecategorizationforAAV accordingtodifferentlevelsofseverity.3
Categories Definition
Localized Diseaserestrictedtoupperand/orlower respiratorytractwithoutsystemicinvolvement orconstitutionalsymptoms
Early systemic
Involvementofanyorganorsystem,without organ-threateningorlife-threateningdisease Generalized Renalorotherorgan-threateningdisease,serum
creatinine<500mol/Lor5.6mg/dL
Severe Renalfailureorotherorgan-threateningdisease, serumcreatinine>500mol/Lor5.6mg/dL
Refractory Progressivediseaseunresponsivetotherapy withglucocorticoidsandcyclophosphamide
AAV, antineutrophil cytoplasmicantibody associated vasculitis; EUVAS,EuropeanVasculitisStudy.
The purposeofthese recommendations is toguide the managementofAAVpatientsaccordingtocurrentevidence fromliterature,facilitatingtheaccesstoavailabletherapiesas wellasminimizingpermanentdamageduetouncontrolled diseaseactivity.Theserecommendationsaddressedaspects ofinductiontherapyinpatientswithAAV,includingGPA,MPA andRLV.
Methods
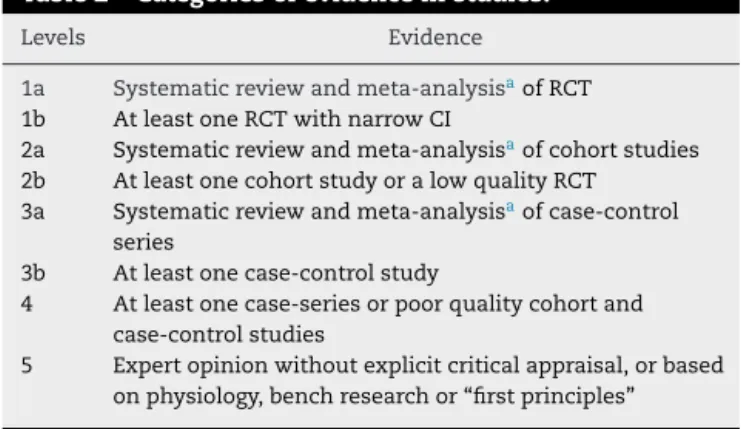
Table2–Categoriesofevidenceinstudies.9
Levels Evidence
1a Systematicreviewandmeta-analysisaofRCT
1b AtleastoneRCTwithnarrowCI
2a Systematicreviewandmeta-analysisaofcohortstudies
2b AtleastonecohortstudyoralowqualityRCT
3a Systematicreviewandmeta-analysisaofcase-control
series
3b Atleastonecase-controlstudy
4 Atleastonecase-seriesorpoorqualitycohortand
case-controlstudies
5 Expertopinionwithoutexplicitcriticalappraisal,orbased
onphysiology,benchresearchor“firstprinciples”
CI,confidenceinterval;RCT,randomizedcontrolledtrials.
a Homogeneityisnecessaryformeta-analysis.
ofpatientswithAAV,including GPA,MPAand RLV.Studies evaluatingEGPApatientswerenotincludedinthissystematic reviewsinceits pathophysiologyisdifferentfromtheother formsofAAVandEGPApatientsarenotincludedinclinical trialsthatassessedtherapyinAAV.
Thefollowingtermswereusedforthesystematicsearch of the literature: ANCA-Associated Vasculitis OR Pauci-ImmuneVasculitisORAnti-NeutrophilCytoplasmic Antibody-AssociatedVasculitisORGranulomatosiswithPolyangiitisOR WegenerORmicroscopicpolyangiitisORSubgloticestenosis AND Induction Chemotherapy OR Remission Induction OR Induction.Applyingthe“random”filter,thetermsrelatedto eachmodalityofinductiontreatmentforAAVpatientswere added.
Inclusion criteria for studies in this systematic review wereasfollows:randomizedcontrolledclinicaltrials(RCTs) addressingAAVtreatment,withanumberofpatientsgreater than100andwithaminimumfollow-upof6months, exten-sionstudiesperformedfromRCTswiththeabovementioned criteriaandsystematicreviewswithmeta-analysisofRCT.In someinstances,historicalcohortstudiesandreviewarticles wereincluded,aswellasintheabsenceofRCTforspecific therapymodalities,open-labelstudiesorlower-qualitycohort studieswereincluded.
The steps of this systematic review of the literature followed PRISMA guidelines.8 Selected studies were
evalu-atedand the degreeofrecommendation foreach question was based on the level of evidence from the studies (Tables2and 3).9–11 Sixteen recommendations were
devel-opedtocoverdifferentaspectsoftheinductiontherapyofAAV (Table4).
Table3–Gradesofrecommendationforeachevidence.9
Grades Definition
A Consistentlevel1studies
B Consistentlevel2or3studiesorextrapolationsfromlevel1 studies
C Level4studiesorextrapolationsfromlevel2or3studies D Level5evidenceortroublinglyinconsistentorinconclusive
studiesofanylevel
Results
1.Areglucocorticoidsrecommendedforthetreatmentof activeAAV?
ThetreatmentprotocolforeveryAAVpatientwithactive dis-easemustincludesystemicglucocorticoids(GC).Theinitial dose for prednisone or equivalentis 1mg/kg/day(grade of recommendationC).GCtherapyneedstobeassociatedwith an immunosuppressiveagentor with abiological agentin patientswithactiveAAV(gradeofrecommendationC).
Literaturereview
AlthoughthereisnodatafromstudiescomparingGCwith placeboinAAVpatients,GCwereusedinallRCTsthat evalu-atedAAVinductiontherapy.12–17 TreatmentofAAVwithGC
alone, without immunosuppressiveor associatedbiological therapy, is notrecommended. In historical series, addition of GC to the treatment of active GPA did not yield any improvement insurvival (level ofevidence 4).18,19 In
addi-tion,treatmentofnon-severeAAVrelapsesexclusivelywith anincreaseinprednisonedosewasassociatedwithahigh relapserateaftertaperingthedrug,despitetheinitial favor-ableresponseobservedinmostcases(levelofevidence2b).20
2.IsthereanydifferencebetweenoralandintravenousGC intheinductiontherapyofAAV?
There is no evidence that intravenous (IV) GC are more efficient than oralGC inAAV patients withactive disease. However,patientswithseveremanifestations(i.e.life threat-eningdiseasewiththeinvolvementofvitalorgans)IVpulse therapy with methylprednisolone should be prescribed at 15mg/kg/dayor0.5–1.0g/dayfor1–3dayswhenstarting treat-ment(gradeofrecommendationD).
Literaturereview
Todate,no study hascomparedoralandIVGCuse inthe treatmentofAAVpatients.IVpulsetherapywith methylpred-nisolonewasadministeredbeforeprednisoneinmoststudies that evaluatedinductionand maintenancetherapyinAAV. Methylprednisolonedoserangedfrom0.5to1.0gperdayfor 1–3 days or15mg/kg(maximumdose per pulseof1g) per dosefor1–3daysor(levelofevidence5).12–17,21–23 However,
theassessmentofefficacyofIVpulsetherapywith methyl-prednisolonewasnotoneoftheaimsoftheseRCT.
3.WhatistheoptimaldoseanddurationoforalGCinthe inductiontherapyofAAV?
Table4–RecommendationsforinductiontherapyofAAV.
PICOquestions Recommendations
1.Areglucocorticoidsrecommended forthetreatmentofactiveAAV?
ThetreatmentprotocolforeveryAAVpatientwithactivediseasemustincludesystemic glucocorticoids.Theinitialdoseforprednisoneorequivalentis1mg/kg/day(gradeof
recommendationC).Glucocorticoidtherapyneedstobeassociatedwithanimmunosuppressive agentorwithabiologicalagentinpatientswithactiveAAV(gradeofrecommendationC). 2.Isthereanydifferencebetweenoral
andIVglucocorticoidsinthe inductiontherapyofAAV?
ThereisnoevidencethatIVglucocorticoidsaremoreefficientthanoralglucocorticoidsinAAV patientswithactivedisease.However,patientswithseveremanifestations(i.e.lifethreatening diseasewiththeinvolvementofvitalorgans)IVpulsetherapywithmethylprednisoloneshouldbe prescribedat15mg/kg/dayor0.5–1.0g/dayfor1–3dayswhenstartingtreatment(gradeof recommendationD).
3.Whatistheoptimaldoseand durationoforalglucocorticoidsin theinductiontherapyofAAV?
TreatmentofpatientswithactiveAAVshouldbeplannedinanindividualizedbasis.Prednisone orprednisoloneisprescribedataninitialdailydoseof0.5–1.0mg/kg/day(maximum80mg/day) foronetofourweeks(gradeofrecommendationB)followedbytapering10mgeverytwotofour weeksuntil20mg/day.Afterwards,dosereductionshouldbe2.5–5.0mgevery2–4weeksuntil completewithdrawal(gradeofrecommendationD).Thedurationofglucocorticoidtherapyshould beatleast6monthsandinsomeinstances,itmaybeupto1or2years.Longerglucocorticoid therapycouldbenecessaryinrelapsingpatients(gradeofrecommendationB).
4.Whatistheroleof
cyclophosphamideintheinduction therapyofAAV?
CyclophosphamideisindicatedininductiontherapyinAAVpatientswithgeneralizeddiseaseor inthosepresentinglife/organ-threateningdisease(gradeofrecommendationA).Additionally, patientswithlesssevereformsofAAV,suchaslocalizeddiseaseandtheearlysystemicformmay benefitfromcyclophosphamidetherapy,especiallyinpatientswhodonotrespondto
methotrexatetherapy(degreeofrecommendationD).Thedurationofcyclophosphamidetherapy inpatientswithAAVshouldbelimitedto3–6monthsinordertoavoidadverseeventsduetoits cumulativedoseandcyclophosphamideshouldbeswitchedtoalesstoxicmaintenancetherapy assoonasremissionisaccomplished(gradeofrecommendationA).
5.Aretheredifferencesbetweenoral andIVpulsetherapy
cyclophosphamidefortherapy inductionofAAV?
Intheshortterm,therearenodifferencesininductionofremissionratesbetweenoralandIV pulsetherapyofcyclophosphamide.Therefore,patientswithactiveAAVmaybetreatedwith eitheroralcyclophosphamideatadoseof2mg/kg/day(maximum200mg/day)orIVpulse cyclophosphamideatadoseof15mg/kg(maximum1.2gperpulse)given3timesinthefirst monthwith2weeksinterval,andthenwithinevery3weeksupto3–6monthsoruntilremission isachieved(gradeofrecommendationA).Inpatientswithrenalinsufficiency,cyclophosphamide doseshouldbecorrectedaccordingtoageandrenalfunction.
6.Ismethotrexateindicatedfor remissioninductioninAAV?
Methotrexate,20–25mg/week,isanalternativetocyclophosphamideforremissioninductionin AAVpatientswithnon-organthreateningdisease,i.e.localizedorearlysystemicdisease(gradeof recommendationA).Methotrexatedosesshouldbereducedby50%inpatientswithGFRbetween 10and50mL/minanditshouldnotbeusedinend-stagerenaldisease(i.e.GFRunder10mL/min) (gradeofrecommendationD).
7.Whatistheroleofrituximabinthe inductiontherapyofAAV?
Rituximabisanalternativetocyclophosphamideintheinductiontherapyingeneralizedformsof AAV,especiallyinpatientswithorgan/life-threateningdisease(gradeofrecommendationA). Rituximab(375mg/m2weeklyfor4weeks)isnon-inferiortocyclophosphamideforinduction
therapyinAAVanditmaybeprescribedwhentherearecontraindicationsforcyclophosphamide use,suchasinpatientswithahighcumulativedoseandinyoungpatientsofchildbearingage withoutestablishedoffspring,orinAAVpatientswithrelapsingdisease(gradeof
recommendationA).Alternatively,rituximabcanbeusedintwoinfusionsatadoseof1gtwo weeksapart.
8.Whichprecautionsshouldbetaken whenprescribingrituximab?
Table4– (Continued)
PICOquestions Recommendations
9.Isplasmaexchangeindicatedinthe treatmentofpatientswithactive AAV?
PlasmaexchangeisindicatedinAAVpatientswithrapidlyprogressiveglomerulonephritiswith serumcreatinine>5.8mg/dL,sinceitleadstoimprovementinrenalsurvivalwhenassociated withglucocorticoidsandcyclophosphamide(gradeofrecommendationA).Plasmaexchangeis prescribedina7-sessionscheduleonalternatedaysata60mL/kgvolumeexchangeoneach occasion,volumereplacementneedstobedonewith5%albuminandoccasionallywithfresh frozenplasmaattheendoftheproceduretoreplenishcoagulationfactors(gradeof
recommendationA).Thereisstillinsufficientevidencetosupportplasmaexchangetotreat patientswithAAVpresentingalveolarhemorrhage,possiblythesepatientsmaybenefitfrom plasmaexchange(gradeofrecommendationD).
10.IsIVIGasanalternativetherapy fortheinductiontherapyofAAV?
IVIGisanalternativefortheinductiontherapyofAAVpatientswithactivediseaseatan immunomodulatorydose(i.e.2g/kgdividedin2–5days),inspecificscenariossuchasininfected AAVpatientswithpersistentdiseaseactivityandinpatientsrefractorytostandardtreatment withglucocorticoidsandcyclophosphamide(gradeofrecommendationB).Additionally,AAV patientswithpersistentandactivediseasewhopresentcontraindicationstocyclophosphamide orrituximabmayalsobenefitfromIVIGtherapy(gradeofrecommendationD).
11.Ismycophenolatemofetil(MMF) indicatedfortheinductiontherapy ofAAV?
Todate,thereisnotenoughevidencetorecommendtheuseofMMFinAAVinductiontherapy,it shouldbereservedasanalternativetocyclophosphamide,rituximabormethotrexate,sincesmall studieshaveshownsomebenefitsovercyclophosphamideinAAVpatientswithactivedisease (gradeofrecommendationC).
12.Isthereanyplaceforanti-TNF␣
agentsintheinductiontherapyof AAVpatients?
TheTNFreceptorblockeragentetanerceptisnotrecommendedintheinductiontherapyofAAV patients(gradeofrecommendationA).Otheranti-TNF␣agentshavenotbeenstudiedproperlyin
AAV.
13.Isazathioprineindicatedforthe inductiontherapyofAAVpatients?
AzathioprineisnotindicatedforinductiontherapyofAAVpatientswithactivedisease(gradeof recommendationD).
14.Howsubglotticstenosisshouldbe approachedinGPApatients?
GPApatientspresentingSGSinthepresenceofsystemicdiseaseactivityshouldbetreatedwith glucocorticoidsandimmunosuppressiveagentsaccordingtodiseaseseverityinassociationwith localtreatment.IncaseofSGSinGPApatientsinremission,werecommendonlylocaltreatment (gradeofrecommendationD).Asfirstlinelocaltherapy,mechanicalintratrachealdilation associatedwithintralesionalinjectionofalong-actingglucocorticoid(e.g.methylprednisolone acetateortriamcinolone)isrecommended,sometimesrequiringrepeatedprocedures(gradeof recommendationC).InrefractorycasesandinpatientspresentingseveremanifestationsofSGS, opensurgerywithlaryngotrachealreconstructionorpermanenttracheostomyshouldbe performed.Indeed,tracheostomyshouldbereservedonlyasanurgentinterventionfor life-threateningsituations(gradeofrecommendationD).
15.Isprophylaxisforpneumocystis pneumoniaindicatedinAAV patientsduringinductiontherapy?
ProphylaxisforPCPwith400mg/80mgdose/dayor800mg/160mgthreetimesaweekofSMT-TMP isindicatedtoAAVpatientundergoinginductiontherapywithglucocorticoidsand
cyclophosphamideorrituximab(gradeofrecommendationA).Patientswithatotallymphocyte countbelow300cells/mm3mustalsoreceiveprophylactictreatmentforPCPregardlessofthe
immunosuppressivetherapyprescribed(gradeofrecommendationB).IfGFRisbetween15and 30mL/minute,SMT-TMPdoseshouldbereducedto400mg/80mgthreetimesaweek.InAAV patientspresentingterminalrenalfailure,duringmethotrexatetherapyorinsulfaallergy,inhaled pentamidineat300mg/monthshouldbepreferred(gradeofrecommendationC).
16.Whatshouldbeconsidered regardingvaccinationinpatients withAAVreceivinginduction therapy?
Wheneveritispossible,patientswithAAVshouldbevaccinatedpriortostarting
immunosuppressivetreatment,ideallythreeweeksbefore.Influenzavaccineseemstobesafe andeffectiveforAAVpatientsinremissionanditshouldbegivenannually(gradeof recommendationB).ConsideringthehighfrequencyofpulmonaryinfectionsinAAVpatients, pneumococcalvaccineshouldalsobeadministered(gradeofrecommendationD).Immunization scheduleinAAVpatientsshouldfollowtheImmunizationGuidepublishedbytheBrazilian SocietyofImmunization/BrazilianSocietyofRheumatology.
AAV,ANCA-associatedvasculitis;ANCA,antineutrophilcytoplasmicantibodies;GFR,glomerularfiltrationrate;GPA,granulomatosiswith polyangiitis;HBV,hepatitisBvirus;HIV,humanimmunodeficiencyvirus;IV,intravenous;IVIG,intravenousimmunoglobulin;PCP,Pneumocystis jiroveciipneumonia;SGS,subglotticstenosis;SMT-TMP,sulfamethoxazoleandtrimethoprim;TNF,tumornecrosisfactor.
LongerGCtherapycould benecessaryinrelapsingpatients (gradeofrecommendationB).
Literaturereview
InallRCTsthatincludedAAVpatients,prednisoneor pred-nisolonewasgivenataninitialdoseof1.0mg/kg/day,12–17,21–24
with a daily dose limited to 60–80mg/day in some
studies.15,16,22 Only one RCT, started prednisone at
0.5–1.0mg/kg/day as initial dose (level of evidence 2b).17
(levelofevidence2b).12–17,21–24InonlytwoRCTs,prednisone
wascompletelywithdrawnwithin5–6months,15,17 whereas
inmostRCTs,thetotaldurationofprednisonetherapyranged from12to24months(levelofevidence2b)(Supplementary TableS1).12–14,16,21–24 Inacohort study,themediantime to
totaloralGCwithdrawalwas8months(levelofevidence2b).25
Ameta-analysisofRCTandcohortstudiesobservedthatthe relapserateislowerinAAVpatientswho havemaintained long-termGCuseevenatlowdosecomparedwithpatients whodiscontinuedGCtherapywithinlessthan12months14% [95%confidenceinterval(95%CI:10–19%)]versus48%(95%CI: 39–58%), respectively (level of evidence 5).26 However, this
issuestillremainsopensincethismeta-analysishadahigh heterogeneityandnostudyhasassessedwhetherlong-term GChasanyimpactonoutcomesofAAVpatients.
4.Whatistheroleofcyclophosphamideintheinduction
therapyofAAV?
CyclophosphamideisindicatedininductiontherapyinAAV patients with generalized disease or in those presenting life/organ-threateningdisease(Table1)(gradeof recommen-dationA).Additionally,patientswithlesssevereformsofAAV, suchaslocalized diseaseand theearlysystemicformmay benefitfromcyclophosphamidetherapy,especiallyinpatients whodonotrespondtomethotrexatetherapy(degreeof rec-ommendationD).Thedurationofcyclophosphamidetherapy in patients with AAV should be limited to 3–6 months in ordertoavoidadverseeventsduetoitscumulativedoseand cyclophosphamideshouldbeswitchedtoalesstoxic mainte-nancetherapyassoonasremissionisaccomplished(gradeof recommendationA).
Literaturereview
TheintroductionofcyclophosphamideinGPAtreatment mod-ifiedthenaturalhistoryofthedisease,improvingtreatment responseandsurvival(levelofevidence4).Despitethebenefits ofcyclophosphamideinthetreatmentofGPA,severaladverse eventswereobserved,suchashemorrhagiccystitis,bone mar-rowtoxicity,severeinfections,includingPneumocystisjirovecii
pneumoniaandanincreasedriskofcancer,mainlybladder cancer.Thelong-termtoxicityofcyclophosphamideis associ-atedwithitscumulativedoseandahighfrequencyofadverse events attributed to cyclophosphamide was observed in a largecohortstudyofGPApatientsduetotheitsextendeduse foratleast1yearafterachievingremission.27Then,attempts
weretriedtominimizecyclophosphamideexposureand tox-icity.Firstly,acohortstudyshowedthatcompleteremissionof GPAwithGCandcyclophosphamidewasachievedatamedian of3monthsoftreatment(levelofevidence2b)25and
subse-quentlyaRCTdemonstratedthatoralcyclophosphamideuse for3–6monthswiththereplacementbyazathioprinedidnot increasetheriskofrelapses whencomparedwith continu-oususeofcyclophosphamidefor12months(levelofevidence 1b).24Currently,GCassociatedwith3–6months
cyclophos-phamidetherapyisthemainmodalityofinductiontherapy forAAV,especiallyingeneralizedformsofthedisease and itisusedasthegoldstandardtreatmentinRCTevaluating efficacyofotheragentsinAAV.13,15,16,28
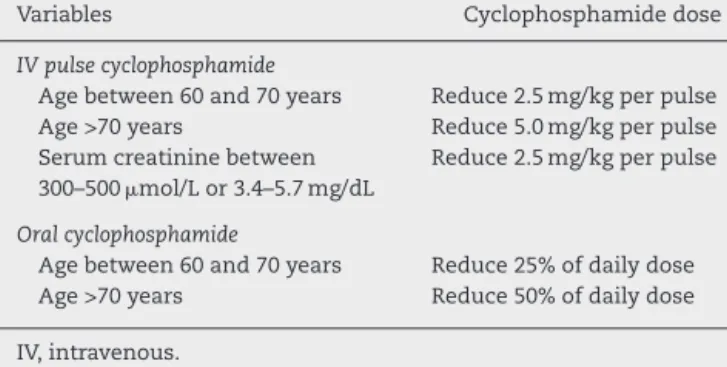
Table5–Dosereductionofpulsedcyclophosphamide basedonageandserumcreatinine.12
Variables Cyclophosphamidedose
IVpulsecyclophosphamide
Agebetween60and70years Reduce2.5mg/kgperpulse
Age>70years Reduce5.0mg/kgperpulse
Serumcreatininebetween 300–500mol/Lor3.4–5.7mg/dL
Reduce2.5mg/kgperpulse
Oralcyclophosphamide
Agebetween60and70years Reduce25%ofdailydose
Age>70years Reduce50%ofdailydose
IV,intravenous.
5.AretheredifferencesbetweenoralandIVpulsetherapy cyclophosphamidefortherapyinductionofAAV?
In the short term, there are no differences in induction of remission rates between oral and IV pulse therapy of cyclophosphamide.Therefore,patientswithactiveAAVmay be treatedwith eitheroralcyclophosphamide atadose of 2mg/kg/day (maximum200mg/day)or IVpulse cyclophos-phamide at adose of 15mg/kg (maximum1.2gper pulse) given3timesinthefirstmonthwith2weeksinterval,and thenwithinevery3weeksupto3–6monthsoruntil remis-sion is achieved(grade ofrecommendation A). In patients with renalinsufficiency, cyclophosphamidedose shouldbe correctedaccordingtoageandrenalfunction(Table5).12
Literaturereview
Inanefforttoreducetheexposuretocyclophosphamideinthe treatmentofAAV,smallstudiesevaluatedtheefficacyoforal andIVpulsetherapywithcyclophosphamideintheinduction ofremissioninAAVpatients, andno differencewasfound between bothtreatment regimens.29–31 However, this issue
wasdefinitelysolvedbytheEUVAStrialCyclophosphamideOral versusPulsed(CYCLOPS),thelargestRCTperformed compar-ingoralandIVpulseofcyclophosphamideinnewlydiagnosed GPA, MPA and RLV with active glomerulonephritis. In this study,IVpulsetherapyandoralcyclophosphamidehad sim-ilarefficacyregardingtimetoremission(meanof3months forbothgroups)andtheproportionofpatientswhoachieved complete remission.However,moreepisodesofleukopenia andahighercumulativedoseofcyclophosphamide(almost twicewhencomparedtopulsetherapygroup)wasfoundin patients onoralcyclophosphamide(level ofevidence1b).12
In the long-termfollow-up oftheCYCLOPS study,patients wereevaluatedinanaverageof4.3yearsandahigherriskof relapseswasobservedinpatientstreatedwithIV cyclophos-phamidepulsetherapy,especiallyinthose withPR3-ANCA. Theincreaseinthefrequencyofdiseaseflaresdidnotresult inanincreaseinmortalityorrenalfailurecomparedwiththe groupwithoutrelapses(levelofevidence2b).32
6.Ismethotrexateindicatedforremissioninductionin AAV?
non-organthreateningdisease,i.e.localizedorearlysystemic disease (grade of recommendation A). Methotrexate doses shouldbereducedby50%inpatientswithglomerular filtra-tionrate(GFR)between10and50mL/minanditshouldnot beusedinend-stagerenaldisease(i.e.GFRunder10mL/min) (gradeofrecommendationD).
Literaturereview
AlthoughcyclophosphamidechangeddiseasecourseofAAV, therewasagrowinginterest inminimizingtoxicitycaused bylong-termtherapyandacaseserieshadalready demon-strated the benefitof methotrexate use inless severelyill patientswithAAV(levelofevidence4).7,33IntheRCTNonrenal
Wegener’sGranulomatosisTreatedAlternativelywithMethotrexate
(NORAM),no differences were observedinterms of remis-sion inductionbetween methotrexate (20–25mg/week) and oral cyclophosphamide(2mg/kg/day) at 6months of ther-apy.Patientspresentingseverediseasemanifestationssuchas serumcreatininelevels>1.7mg/dL,urinaryredcellcasts, pro-teinuria>1g/day,severehemoptysisassociatedwithbilateral infiltrates,cerebralvasculitis,orbitalpseudotumor,massive gastrointestinal bleeding, heart failure due to pericarditis or myocarditis and rapidly progressive neuropathy were excluded. Itshouldbenotedthat inbothgroups immuno-suppressiveagentsweretaperedanddiscontinuedbymonth 12.Relapserateat18monthswashigherinthe methotrex-ate group,but thesemostly occurred after discontinuation of therapy (level of evidence 1b).13 After a mean
follow-up timeof6years,inAAV patientsoriginallyevaluated at NORAMstudy,therewasnosignificantdifferenceregarding therelapseratebetweenpatientstreatedwithmethotrexate andcyclophosphamide.34Itisimportanttoemphasizethat
immunosuppressivetherapyshould notbediscontinuedin AAVpatientsat12monthsinordertopreventrelapses(level ofevidence4).13
7.Whatistheroleofrituximabintheinductiontherapy
ofAAV?
Rituximab is an alternative to cyclophosphamide in the inductiontherapyingeneralizedformsofAAV,especiallyin patientswithorgan/life-threateningdisease(gradeof recom-mendationA).Rituximab(375mg/m2 weeklyfor4weeks)is
non-inferiorto cyclophosphamidefor inductiontherapy in AAVanditmaybeprescribedwhenthereare contraindica-tionsforcyclophosphamideuse, suchasinpatientswitha highcumulativedoseandinyoungpatientsofchildbearing age without establishedoffspring, or inAAV patients with relapsingdisease(gradeofrecommendationA).Alternatively, rituximabcanbeusedintwoinfusionsatadoseof1gtwo weeksapart.
Literaturereview
TwoRCTevaluatedtheefficacyofrituximabinAAVinduction therapycomparedtocyclophosphamide,bothat375mg/m2
ofbody surfacearea,weeklyfor4consecutive weeks(level ofevidence1b).15,16 TheRAVE study (Rituximabfor
ANCA-associatedvasculitis)included197patientswithactiveAAV. Rituximab and conventional therapy groups comprised 99 and 98 patients respectively. In the group treated with a
conventionalprotocol,cyclophosphamidewasprescribedat 2mg/kg/dayfor3–6months,followedbyazathioprine.Unless a relapse occurred, GC had to be tapered and withdrawn at 6 months of treatment. Rituximab was non-inferior to cyclophosphamideandcompleteremissionwasachievedin 64% ofthepatientsinthe rituximabgroupand 53%ofthe patients in the cyclophosphamide group at 6 months of treatment (level ofevidence1b). However,inthe subgroup ofrelapsingpatients, rituximabwas superiorto cyclophos-phamide(67%vs.42%,p=0.01)(levelofevidence1b).15Inthe
long-termfollow-upoftheRAVEstudy,sustainedremission ratesremainedsimilarinbothgroupsat6,12and18months andnodifferencesinadverseeventswereobserved(levelof evidence2b).35
TheRITUXVAS(RituximabVersusCyclophosphamidein ANCA-Associated Vasculitis)studyprotocol wassomewhatdifferent from theRAVE studyand itsprimaryend pointswere sus-tained remissionat 12 monthsand severe adverse events. Forty-four patients with newly diagnosed AAV with renal involvement were randomly included ina 3:1ratio in two groupsasfollowsrituximab(375mg/m2fourweeklyinfusions)
with two infusions of cyclophosphamide and the other groupreceivedIVcyclophosphamidepulsesfor3–6months, followed by azathioprine. Patients on dialysis were not excluded,althoughtheywereasmallsubgroup,someofthese patients underwent plasma exchange.Sustained remission at12monthswassimilarbetweenrituximaband cyclophos-phamide AAV patients with severe disease manifestations (76% vs. 82%,p=0.68, respectively). Severe adverse events, deathrateandtheimprovementinGFRwerealsosimilarin bothgroups(levelofevidence1b).16At24months,relapserate
remainedsimilarbetweenrituximabandcyclophosphamide groups,butintheformerrelapseswereassociatedwithBcell normalizationinperipheralblood(levelofevidence2b).36
8.Whichprecautionsshouldbetakenwhenprescribing rituximab?
Before the infusionof rituximabin AAV patients, serology testsforHIV,HBVandsyphilisshouldbechecked.Patients withchronicHBV and HIVshouldonlybetreatedwith rit-uximab with concomitant prescription of antiviral therapy andtheconsultationfromaspecialistininfectiousdiseases (gradeofrecommendationC).37Vaccinationshouldbegiven
priortorituximabinfusionwheneveritispossible,especially forannualinfluenza,pneumococcalandHBV.Administration of other vaccines suchas anti-tetanus and anti-diphtheria oranti-meningoccocalisoptionalbutimmunizationrecords shouldbeupdated(gradeofrecommendationD).37Baseline
serumimmunoglobulinlevelsandB-cellcountinperipheral blood are recommended to be measured before rituximab infusion and thereafter. It isimportant to measure serum immunoglobulins,especiallyserumIgG,priortoeach admin-istrationofrituximaband4–6monthsafterandtoassessthe needforreplacementofIVimmunoglobulin(IVIG)(gradeof recommendationC).37–39Incasesofsevere
ifpatient presents serum IgGpersistently below500mg/dL and severe recurrentinfections (grade of recommendation C).37,39,40However,itshouldbetakenintoaccountthebalance
betweentreatmentbenefitstocontrolinflammatoryactivity andtheriskofsevereadverseeventswithrituximabtherapy.
Literaturereview
LowIgGlevelsisobservedinupto34%ofpatientswith mul-tisystemautoimmunediseases afterrituximabtherapyand higherGCdoses aswell astotaldoseofrituximab≥6gare
associatedwithIgGfall(levelofevidence3b).41Inaddition,in
AAVpatientstheuseofcyclophosphamideisassociatedwitha decreaseinimmunoglobulinlevelsthatarefurtherdecreased withsubsequentrituximabtherapy(levelofevidence3b).42Up
to24monthsoffollow-up,severeinfectionswerenot differ-entbetweenAAVpatientstreatedwithrituximabandpatients treatedwithconventionaltherapyforAAVinRCT.15,16,35,36
9. Isplasmaexchangeindicatedinthetreatmentof
patientswithactiveAAV?
Plasmaexchange isindicatedinAAV patientswithrapidly progressive glomerulonephritis with serum creatinine >5.8mg/dL,sinceit leadstoimprovementinrenal survival whenassociated withGC and cyclophosphamide(grade of recommendation A). Plasma exchange is prescribed in a 7-sessionscheduleon alternatedaysata60mL/kgvolume exchange on each occasion,volume replacement needs to bedonewith5%albuminandoccasionallywithfreshfrozen plasmaattheendoftheproceduretoreplenishcoagulation factors(gradeofrecommendationA).Thereisstillinsufficient evidencetosupportplasmaexchangetotreatpatientswith AAVpresentingalveolarhemorrhage,possiblythesepatients maybenefitfromplasmaexchange(gradeofrecommendation D).
Literaturereview
Plasmaexchangewasintroducedinthetreatmentof pauci-immunevasculitiswithrenalinvolvementafteritssuccessful useinanti-glomerularbasementmembraneantibody (anti-GBM)disease.43Initially,twosmallRCTevaluatedtheaddition
ofplasmaexchangetoconventionaltreatmentinAAVpatients withrenalimpairmentandobservedabetterrecoveryofrenal function,especiallyinpatientswithelevatedcreatinineand thoseonhemodialysis.However,noimpactwasobservedon mortality(levelofevidence2b).44,45
ThelargestRTC thatevaluatedplasmaexchangeinAAV was thePlasma Exchange versus Methylprednisolone forsevere renalvasculitis(MEPEX)study.Inthisstudy,137patientswith AAVandrapidlyprogressiveglomerulonephritiswith creati-nineabove5.8mg/dLwere treatedwithsessions ofplasma exchangeorwithIVmonthlypulsesofmethylprednisolone. Bothgroupsreceivedoralprednisoneandcyclophosphamide. After 3 months, 69% of patients who underwent plasma exchangewerefreefromdialysis,comparedto49%ofthose receiving methylprednisolone pulses(p=0.02) (level of evi-dence1b).Plasmaexchangewasassociatedwithareduction intheriskofprogressiontoend-stagerenaldiseaseby24%at 12months(95%CI:6.1–41.0%).However,survivalandadverse events were similar between both groups after 1 year of
follow-up (level of evidence 1b).14 The benefit of plasma
exchangeonsurvivalandontheriskofdevelopingend-stage renaldiseasearenotevidentat3.95yearsoffollow-up(levelof evidence2b).46RegardingalveolarhemorrhageinAAV,thereis
noevidenceofbenefitfromplasmaexchangeyet.ThePlasma ExchangeandGCdosinginthetreatmentofanti-neutrophil cyto-plasmassociatedvasculitis(PEXIVAS)studyisanongoingRCT that evaluatesthe efficacy ofplasma exchange inpatients withGPAandMPAwithrenalinvolvementanddecreasedrenal functionand/oralveolarhemorrhage.47
10.IsIVIGasanalternativetherapyfortheinduction
therapyofAAV?
IVIGisanalternativefortheinductiontherapyofAAVpatients withactivediseaseatanimmunomodulatorydose(i.e.2g/kg dividedin2–5days),inspecificscenariossuchasininfected AAVpatientswithpersistentdiseaseactivityandinpatients refractory to standard treatment with GC and cyclophos-phamide (grade of recommendation B). Additionally, AAV patientswithpersistentandactivediseasewhopresent con-traindications to cyclophosphamideor rituximab may also benefitfromIVIGtherapy(gradeofrecommendationD).
Literaturereview
AsatisfactoryresponsewasobservedinmostAAVpatients treatedwithIVIG insmall open-labelstudies thatincluded patients with active AAV refractory to GC and immuno-suppressive agents, or in patients withrapidly progressive glomerulonephritisassociatedwithMPO-ANCA(levelof evi-dence4).48–50 AmulticenterRCTevaluatedtheefficacy ofa
single dose ofIVIG in 34 patients withactive GPA or MPA despitetreatment.SeventeenAAVpatientsweretreatedwith IVIGand17withplacebo.Theprimaryoutcomewas reduc-tion ofmorethan 50%intheBVAS inthreemonthsand it wasachievedby14patients.However,afterthreemonthsno significantdifferenceswerefoundinserumCRPlevelsorin diseaseactivitybetweengroups(levelofevidence2b).Adverse eventsweremorefrequentinIVIGgroup.51AFrench
multicen-tricretrospectivestudyevaluated92AAVpatientswho had receiveddifferentIVIGdoseregimensandobservedcomplete remissioninonly56%atsixmonths(levelofevidence4).52
11.Ismycophenolatemofetil(MMF)indicatedforthe inductiontherapyofAAV?
Todate,thereisnotenoughevidencetorecommendtheuse ofMMFinAAVinductiontherapy, itshould bereservedas analternativetocyclophosphamide,rituximabor methotrex-ate, since small studies have shown some benefits over cyclophosphamideinAAVpatientswithactivedisease(grade ofrecommendationC).
Literaturereview
nodifferencebetweenthetwotherapeuticmodalitiesinMPA (levelofevidence3b).53,54
12.Isthereanyplaceforanti-TNF˛agentsinthe
inductiontherapyofAAVpatients?
The TNF receptor blocker agent etanercept is not recom-mendedintheinductiontherapyofAAV patients(gradeof recommendationA).Otheranti-TNF␣agentshavenotbeen
studiedproperlyinAAV.
Literaturereview
ThestudyWegener’sGranulomatosisEtanerceptTrial(WGET)was theonlyrandomizedcontrolledtrialthatevaluatedtheuse ofanti-TNF␣agentsinGPA.Inthisstudy,180GPApatients
received standard therapy with GCand cyclophosphamide ormethotrexateplus etanerceptor placebo.Nodifferences werefoundbetweenetanerceptandplaceboregardingthe fre-quencyofdiseaserelapses,sustainedremission,irreversible damage, quality of life or side effects. However, six cases ofsolidtumorswereidentifiedinpatientsfromthe etaner-ceptgroupwhowerealsoundercyclophosphamidetherapy, whereasnosolidtumorswereobservedintheplacebogroup (level of evidence 1b).17 The occurrence of solid tumors
remainedincreasedduringlong-termfollow-up(levelof evi-dence2b).55
13.Isazathioprineindicatedfortheinductiontherapyof
AAVpatients?
AzathioprineisnotindicatedforinductiontherapyofAAV patientswithactivedisease(gradeofrecommendationD).
Literaturereview
Todate,noRCThasevaluatedazathioprineintheinduction therapyofAAVpatients(levelofevidence5).Azathioprine pre-ventsdiseaserelapsesinAAVpatientswhoattainedremission (levelofevidence1b).21,22,24
14.HowsubglotticstenosisshouldbeapproachedinGPA patients?
GPApatientspresentingsubglotticstenosis(SGS)inthe pres-enceofsystemicdiseaseactivityshouldbetreatedwithGC andimmunosuppressiveagentsaccordingtodisease sever-ity in association with local treatment. In case of SGS in GPApatientsinremission, werecommendonlylocal treat-ment(gradeofrecommendationD).Asfirstlinelocaltherapy, mechanical intratracheal dilation associated with intrale-sionalinjectionofalong-actingGC(e.g.methylprednisolone acetateortriamcinolone)isrecommended,sometimes requir-ing repeated procedures (grade of recommendation C). In refractorycasesandinpatientspresentingsevere manifesta-tionsofSGS,opensurgerywithlaryngotrachealreconstruction orpermanenttracheostomyshouldbeperformed.Indeed, tra-cheostomyshouldbereservedonlyasanurgentintervention forlife-threateningsituations(gradeofrecommendationD).
Literaturereview
SGSisapotentiallylife-threateningcomplicationofGPAandit affectmorefrequentlypatientswithdiseaseonsetinyounger ages.56SGShavebeendescribedinastateofdisease
remis-siondespiteimmunosuppressivetherapy.TherearenoRCT assessingtherapeuticoptionsforthisdiseasemanifestation but numerouscase reportsand case series including from 2to36patientshavebeenpublished.Approximately25%of patients with SGS respond tooral GC with or without an immunosuppressiveagent.56,57Theremainderwillneedlocal
therapy. One ofthe mostwell described localintervention ismechanicalintratrachealdilationassociatedwith intrale-sionalinjectionofalong-actingGC.56,58–60Inthetwolargest
caseserieswith20and21GPApatientswithSGSwho under-went this procedure, no new tracheostomy was necessary anddecannulationwaspossibleinalmostallpreviously tra-cheostomizedpatients.Anaverageof2.4–3.0procedureswas necessaryperpatient.56,58Intralesionalinjectionisperformed
with a long-acting GC (e.g. methylprednisolone 40–120mg or triamcinolone 40mg) in a 4-quadrant submucosal pat-tern ofthe stenotic ring before mechanical dilation.Some authors suggest to perform the lysis of stenotic ring with radialincisionsbeforemanualdilation.58–60IVGCwas
admin-istered duringtheprocedure insomepapers.Regarding its antifibrotic effects, topical mitomycin C was proposed to preventrestenosis, butcontradictoryresultswere observed in different case series.59,61,62 Local laser therapy (CO2 or
NG:YAG) hasbeen described asan alternative forSGS, but resultsweredivergent,includingcasesofstenosis exacerba-tion afterthisprocedure.57,58,63 Opensurgicalinterventions
suchaslaryngotracheoplastyare describedinpatientswho failed endoscopicprocedures.57 In view ofnewendoscopic
techniques,tracheostomyhavebeenreservedforemergency situations.64,65Intratrachealstentshavebeencontraindicated
bysomeauthorsinGPApatientsduetothehighfrequencyof complications.66
15.Isprophylaxisforpneumocystispneumoniaindicated inAAVpatientsduringinductiontherapy?
Prophylaxis forPneumocystis jirovecii pneumonia (PCP) with 400mg/80mgdose/dayor800mg/160mgthreetimesaweekof sulfamethoxazoleandtrimethoprim(SMT-TMP)isindicated to AAV patientundergoing inductiontherapy withGC and cyclophosphamideorrituximab(gradeofrecommendationA). Patientswithatotallymphocytecountbelow300cells/mm3
mustalsoreceiveprophylactictreatmentforPCPregardless oftheimmunosuppressivetherapyprescribed(gradeof rec-ommendation B). If GFR is between 15 and 30mL/minute, SMT-TMP dose should be reduced to 400mg/80mg three timesaweek.InAAVpatientspresentingterminalrenal fail-ure,duringmethotrexatetherapyorinsulfaallergy,inhaled pentamidineat300mg/monthshouldbepreferred(gradeof recommendationC).
Literaturereview
Severeinfectionsareobservedinupto39%oftheGPApatients and PCP affects a third of them (level of evidence 2b).67
systematicreviewevaluatedtheefficacyofprophylaxisforPCP inimmunocompromisedpatientswhowerenotHIV-infected andfoundthatSMT-TMPuseresultedin85%reductionofPCP (relativerisk:0.15;95%CI:0.04–0.62)(levelofevidence1a).69
InasmallRCTthatcomparedoralandIVpulse cyclophos-phamidetotreatGPA,upto20%ofpatientsdevelopedPCP. Amongstpatientswhodidnotreceiveprophylaxiswith SMT-TMP,theincidenceofPCPwashigherinthosetreatedwithoral cyclophosphamide(30.4%)comparedwiththosetreatedwith IVpulsecyclophosphamide(11.1%)(levelofevidence2b).29In
thetrialJapanesepatientswithMPO-ANCA-associatedvasculitis
(JMAAV)thatevaluatedtheAAVtreatmentbasedondisease severity,31outof48patientsreceivedSMT-TMPprophylaxis forPCP.Duringthe study,threePCP eventswere observed, twoinpatientswithoutPCPprophylaxisandathirdeventtwo monthsafterPCPprophylaxiswithdrawalduetolivertoxicity. Indeed,nopatientsunderprophylaxisdevelopedPCP(levelof evidence2b).70
Intworeviewarticlesthatapproachedinfectionsobserved inobservationalandinterventionalstudiesthatincludedAAV patients,theauthorsstate:(1)SMT-TMPorpentamidine(in caseofintoleranceorcontraindication)shouldbeprescribed routinely,duringtheinitialphaseofinductiontherapy,and this prophylaxis should be maintained in the presence of riskfactors such asage above 55 years,lymphocyte count below300/mm3,long-termtreatmentwithGCatdosesabove
15–20mg/day,andtreatmentwithotherimmunosuppressive agents,particularlycyclophosphamide(levelofevidence2a); (2)SMT-TMPshouldbeprescribedduringinductiontherapy withother agents,especiallyrituximab,untilGCdailydose isreducedto10mg/day(levelofevidence3b);(3)Inpatients usingmethotrexateasinductiontherapy,theuseof pentami-dineshouldbeconsidered,inviewofdruginteractionswith SMT-TMP(levelofevidence3b).71,68
16.Whatshouldbeconsideredregardingvaccinationin patientswithAAVreceivinginductiontherapy?
Wheneveritispossible,patientswithAAVshouldbe vacci-natedpriortostartingimmunosuppressivetreatment,ideally three weeks before. Influenza vaccine seems to be safe and effective for AAV patients in remission and it should be given annually (grade of recommendation B). Consid-ering the high frequency of pulmonary infections in AAV patients,pneumococcalvaccineshouldalsobeadministered (gradeofrecommendationD).ImmunizationscheduleinAAV patients should follow the Immunization Guide published bytheBrazilianSocietyofImmunization/BrazilianSocietyof Rheumatology.72
Literaturereview
InfluenzavaccinationinAAVpatientsinremissionleadsto highantibodytitersandprotectionsimilarlytothatof con-trols,withno impacton disease activity (levelofevidence 2b).73–75Additionally,aretrospectivestudyhasdemonstrated
areductionintheriskofdiseaserelapseinAAVpatientswho weregiveninfluenzavaccinecomparedwithnon-vaccinated patients (level of evidence 3b).74 In fact, it is
recom-mendedtoimmunizeAAVpatientswithinactivatedvaccines suchashepatitisBvaccineandanti-pneumococcalvaccine,
particularlyinAAVpatientspriortorituximabtherapy(level ofevidence5).37
InthePneumovasPilot1study,19AAVpatientsweredivided intotwogroups(e.g.inductionandmaintenancetherapy),and weregiventheanti-pneumoccocalvaccine13valent,23valent or both.Preliminarydatahavedemonstratedthat the anti-pneumococcalvaccine,evenwhenboth13and23valentwere associated,wereineffectivewhenadministeredduring induc-tiontherapyforAAV.76
Funding
ThisstudywasfundedbyBrazilianSocietyofRheumatology.
Conflicts
of
interest
AWSS,GAF,JRandRALreceivedgrantsfromRoche.Theothers authorsdeclarenoconflictsofinterest.
Acknowledgements
TheauthorsthankVirginiaFernandesTrevisan,RachelRiera andCarolinaCruzfortheirvaluablecontributionforthis sys-tematicreviewoftheliterature.
Appendix
A.
Supplementary
data
Supplementarydataassociatedwiththisarticlecanbefound, intheonlineversion,atdoi:10.1016/j.rbre.2017.06.003.
r
e
f
e
r
e
n
c
e
s
1.JennetteJC,FalkRJ,BaconPA,BasuN,CidMC,FerrarioF,etal. 2012revisedInternationalChapelHillConsensusConference NomenclatureofVasculitides.ArthritisRheum.2013;65:1–11.
2.SilvadeSouzaAW.Autoantibodiesinsystemicvasculitis. FrontImmunol.2015;6:184.
3.MukhtyarC,GuillevinL,CidMC,DasguptaB,deGrootK, GrossW,etal.,EuropeanVasculitisStudyGroup.EULAR recommendationsforthemanagementofprimarysmalland mediumvesselvasculitis.AnnRheumDis.2009;68:310–7.
4.YatesM,WattsRA,BajemaIM,CidMC,CrestaniB,HauserT, etal.EULAR/ERA-EDTArecommendationsforthe
managementofANCA-associatedvasculitis.AnnRheumDis. 2016;75:1583–94.
5.MukhtyarC,LeeR,BrownD,CarruthersD,DasguptaB,Dubey S,etal.ModificationandvalidationoftheBirmingham VasculitisActivityScore(version3).AnnRheumDis. 2009;68:1827–32.
6.StoneJH,HoffmanGS,MerkelPA,MinYI,UhlfelderML, HellmannDB,etal.InternationalNetworkfortheStudyof theSystemicVasculitides(INSSYS).Adisease-specificactivity indexforWegener’sgranulomatosis:modificationofthe BirminghamVasculitisActivityScore.ArthritisRheum. 2001;44:912–20.
7.KallenbergCG.Keyadvancesintheclinicalapproachto ANCA-associatedvasculitis.NatRevRheumatol. 2014;10:484–93.
systematicreviewsandmeta-analysesofstudiesthat evaluatehealthcareinterventions:explanationand elaboration.BMJ.2009;339:b2700.
9. OxfordCentreforEvidence-basedMedicine.Levelsof Evidence(March2009).CEBM;2009.
10.GuyattGH,OxmanAD,KunzR,Falck-YtterY,VistGE,Liberati A,etal.,GRADEWorkingGroup.Goingfromevidenceto recommendations.BMJ.2008;336:1049–51.
11.GuyattGH,OxmanAD,VistGE,KunzR,Falck-YtterY, Alonso-CoelloP,etal.,GRADEWorkingGroup.GRADE:an emergingconsensusonratingqualityofevidenceand strengthofrecommendations.BMJ.2008;336:924–6.
12.deGrootK,HarperL,JayneDR,FloresSuarezLF,GregoriniG, GrossWL,etal.,EUVAS(EuropeanVasculitisStudyGroup). Pulseversusdailyoralcyclophosphamideforinductionof remissioninantineutrophilcytoplasmicantibody-associated vasculitis:arandomizedtrial.AnnInternMed.
2009;150:670–80.
13.DeGrootK,RasmussenN,BaconPA,TervaertJW,FeigheryC, GregoriniG,etal.Randomizedtrialofcyclophosphamide versusmethotrexateforinductionofremissioninearly systemicantineutrophilcytoplasmicantibody-associated vasculitis.ArthritisRheum.2005;52:2461–9.
14.JayneDR,GaskinG,RasmussenN,AbramowiczD,FerrarioF, GuillevinL,etal.,EuropeanVasculitisStudyGroup. Randomizedtrialofplasmaexchangeorhigh-dosage methylprednisoloneasadjunctivetherapyforsevererenal vasculitis.JAmSocNephrol.2007;18:2180–8.
15.StoneJH,MerkelPA,SpieraR,SeoP,LangfordCA,Hoffman GS,etal.,RAVE-ITNResearchGroup.Rituximabversus cyclophosphamideforANCA-associatedvasculitis.NEnglJ Med.2010;363:221–32.
16.JonesRB,TervaertJW,HauserT,LuqmaniR,MorganMD,Peh CA,etal.,EuropeanVasculitisStudyGroup.Rituximabversus cyclophosphamideinANCA-associatedrenalvasculitis.N EnglJMed.2010;363:211–20.
17.Wegener’sGranulomatosisEtanerceptTrial(WGET)Research Group.EtanerceptplusstandardtherapyforWegener’s granulomatosis.NEnglJMed.2005;352:351–61.
18.WaltonEW.Giant-cellgranulomaoftherespiratorytract (Wegener’sgranulomatosis).BrMedJ.1958;2:265–70.
19.HollanderD,ManningRT.Theuseofalkylatingagentsinthe treatmentofWegener’sgranulomatosis.AnnInternMed. 1967;67:393–8.
20.MiloslavskyEM,SpecksU,MerkelPA,SeoP,SpieraR,Langford CA,etal.,RituximabinANCA-AssociatedVasculitis-Immune ToleranceNetworkResearchGroup.Outcomesofnonsevere relapsesinantineutrophilcytoplasmicantibody-associated vasculitistreatedwithglucocorticoids.ArthritisRheumatol. 2015;67:1629–36.
21.PagnouxC,MahrA,HamidouMA,BoffaJJ,RuivardM,Ducroix JP,etal.,FrenchVasculitisStudyGroup.Azathioprineor methotrexatemaintenanceforANCA-associatedvasculitis.N EnglJMed.2008;359:2790–803.
22.HiemstraTF,WalshM,MahrA,SavageCO,deGrootK,Harper L,etal.,EuropeanVasculitisStudyGroup(EUVAS).
Mycophenolatemofetilvsazathioprineforremission maintenanceinantineutrophilcytoplasmic
antibody-associatedvasculitis:arandomizedcontrolledtrial. JAMA.2010;304:2381–8.
23.GuillevinL,PagnouxC,KarrasA,KhouatraC,AumaîtreO, CohenP,etal.,FrenchVasculitisStudyGroup.Rituximab versusazathioprineformaintenanceinANCA-associated vasculitis.NEnglJMed.2014;371:1771–80.
24.JayneD,RasmussenN,AndrassyK,BaconP,TervaertJW, DadonienéJ,etal.,EuropeanVasculitisStudyGroup.A randomizedtrialofmaintenancetherapyforvasculitis
associatedwithantineutrophilcytoplasmicautoantibodies.N EnglJMed.2003;349:36–44.
25.LangfordCA,Talar-WilliamsC,BarronKS,SnellerMC.Useof acyclophosphamide-inductionmethotrexate-maintenance regimenforthetreatmentofWegener’sgranulomatosis: extendedfollow-upandrateofrelapse.AmJMed. 2003;114:463–9.
26.WalshM,MerkelPA,MahrA,JayneD.Effectsofdurationof glucocorticoidtherapyonrelapserateinantineutrophil cytoplasmicantibody-associatedvasculitis:ameta-analysis. ArthritisCareRes(Hoboken).2010;62:1166–73.
27.HoffmanGS,KerrGS,LeavittRY,HallahanCW,LebovicsRS, TravisWD,etal.Wegenergranulomatosis:ananalysisof158 patients.AnnInternMed.1992;116:488–98.
28.HolleJU,GrossWL.TreatmentofANCA-associated vasculitides(AAV).AutoimmunRev.2013;12:483–6.
29.GuillevinL,CordierJF,LhoteF,CohenP,JarrousseB,RoyerI, etal.Aprospective,multicenter,randomizedtrialcomparing steroidsandpulsecyclophosphamideversussteroidsand oralcyclophosphamideinthetreatmentofgeneralized Wegener’sgranulomatosis.ArthritisRheum.1997;40:2187–98.
30.HaubitzM,SchellongS,GöbelU,SchurekHJ,SchaumannD, KochKM,etal.Intravenouspulseadministrationof cyclophosphamideversusdailyoraltreatmentinpatients withantineutrophilcytoplasmicantibody-associated vasculitisandrenalinvolvement:aprospective,randomized study.ArthritisRheum.1998;41:1835–44.
31.AduD,PallA,LuqmaniRA,RichardsNT,HowieAJ,EmeryP, etal.Controlledtrialofpulseversuscontinuousprednisolone andcyclophosphamideinthetreatmentofsystemic
vasculitis.QJM.1997;90:401–9.
32.HarperL,MorganMD,WalshM,HoglundP,WestmanK, FlossmannO,etal.,EUVASInvestigators.Pulseversusdaily oralcyclophosphamideforinductionofremissionin ANCA-associatedvasculitis:long-termfollow-up.AnnRheum Dis.2012;71:955–60.
33.HoffmanGS,LeavittRY,KerrGS,FauciAS.Thetreatmentof Wegener’sgranulomatosiswithglucocorticoidsand methotrexate.ArthritisRheum.1992;35:1322–9.
34.FaurschouM,WestmanK,RasmussenN,deGrootK, FlossmannO,HöglundP,etal.,EuropeanVasculitisStudy Group.BriefReport:long-termoutcomeofarandomized clinicaltrialcomparingmethotrexatetocyclophosphamide forremissioninductioninearlysystemicantineutrophil cytoplasmicantibody-associatedvasculitis.ArthritisRheum. 2012;64:3472–7.
35.SpecksU,MerkelPA,SeoP,SpieraR,LangfordCA,Hoffman GS,etal.,RAVE-ITNResearchGroup.Efficacyof
remission-inductionregimensforANCA-associated vasculitis.NEnglJMed.2013;369:417–27.
36.JonesRB,FurutaS,TervaertJW,HauserT,LuqmaniR,Morgan MD,etal.,EuropeanVasculitisSociety(EUVAS).Rituximab versuscyclophosphamideinANCA-associatedrenal vasculitis:2-yearresultsofarandomisedtrial.AnnRheum Dis.2015;74:1178–82.
37.CharlesP,BienvenuB,BonnotteB,GobertP,GodmerP, HachullaÉ,etal.,FrenchVasculitisStudyGroup.Rituximab. RecommendationsoftheFrenchVasculitisStudyGroup (FVSG)forinductionandmaintenancetreatmentsofadult, antineutrophilcytoplasmantibody-associatednecrotizing vasculitides.PresseMed.2013;42:1317–30.
38.GuerryMJ,BroganP,BruceIN,D’CruzDP,HarperL,Luqmani R,etal.Recommendationsfortheuseofrituximabin anti-neutrophilcytoplasmantibody-associatedvasculitis. Rheumatology(Oxford).2012;51:634–43.
Group.BSRandBHPRguidelinesontheuseofrituximabin rheumatoidarthritis.Rheumatology(Oxford).2011;50:2311–3.
40.CarvalhoB,SoléD,Condino-NetoA,RosárioFilhoN,Ouricuri AL,SilvaSegundoGR,etal.IConsensobrasileirosobreouso deimunoglobulinahumanaempacientescom
imunodeficiênciasprimárias.RevBrasAlergImunopatol. 2010;33:104–16.
41.MarcoH,SmithRM,JonesRB,GuerryMJ,CatapanoF,BurnsS, etal.Theeffectofrituximabtherapyonimmunoglobulin levelsinpatientswithmultisystemautoimmunedisease. BMCMusculoskeletDisord.2014;15:178.
42.VenhoffN,EffelsbergNM,SalzerU,WarnatzK,PeterHH, LebrechtD,etal.Impactofrituximabonimmunoglobulin concentrationsandBcellnumbersaftercyclophosphamide treatmentinpatientswithANCA-associatedvasculitides. PLoSONE.2012;7:e37626.
43.LockwoodCM,ReesAJ,PearsonTA,EvansDJ,PetersDK, WilsonCB.Immunosuppressionandplasma-exchangeinthe treatmentofGoodpasture’ssyndrome.Lancet.1976;1:711–5.
44.PuseyCD,ReesAJ,EvansDJ,PetersDK,LockwoodCM.Plasma exchangeinfocalnecrotizingglomerulonephritiswithout anti-GBMantibodies.KidneyInt.1991;40:757–63.
45.SzpirtWM,HeafJG,PetersenJ.Plasmaexchangeforinduction andcyclosporineAformaintenanceofremissionin
Wegener’sgranulomatosis–aclinicalrandomizedcontrolled trial.NephrolDialTransplant.2011;26:206–13.
46.WalshM,CasianA,FlossmannO,WestmanK,HöglundP, PuseyC,etal.,EuropeanVasculitisStudyGroup(EUVAS). Long-termfollow-upofpatientswithsevere
ANCA-associatedvasculitiscomparingplasmaexchangeto intravenousmethylprednisolonetreatmentisunclear.Kidney Int.2013;84:397–402.
47.WalshM,MerkelPA,PehCA,SzpirtW,GuillevinL,PuseyCD, etal.,PEXIVASInvestigators.Plasmaexchangeand
glucocorticoiddosinginthetreatmentofanti-neutrophil cytoplasmantibodyassociatedvasculitis(PEXIVAS):protocol forarandomizedcontrolledtrial.Trials.2013;14:73.
48.RichterC,SchnabelA,CsernokE,DeGrootK,Reinhold-Keller E,GrossWL.Treatmentofanti-neutrophilcytoplasmic antibody(ANCA)-associatedsystemicvasculitiswith high-doseintravenousimmunoglobulin.ClinExpImmunol. 1995;101:2–7.
49.MusoE,Ito-IharaT,OnoT,ImaiE,YamagataK,AkamatsuA, etal.Intravenousimmunoglobulin(IVIg)therapyin MPO-ANCArelatedpolyangiitiswithrapidlyprogressive glomerulonephritisinJapan.JpnJInfectDis.2004;57:S17–8.
50.MartinezV,CohenP,PagnouxC,VinzioS,MahrA,MouthonL, etal.,FrenchVasculitisStudyGroup.Intravenous
immunoglobulinsforrelapsesofsystemicvasculitides associatedwithantineutrophilcytoplasmicautoantibodies: resultsofamulticenter,prospective,open-labelstudyof twenty-twopatients.ArthritisRheum.2008;58:308–17.
51.JayneDR,ChapelH,AduD,MisbahS,O’DonoghueD,ScottD, etal.IntravenousimmunoglobulinforANCA-associated systemicvasculitiswithpersistentdiseaseactivity.QJM. 2000;93:433–9.
52.CrickxE,MachelartI,LazaroE,KahnJE,Cohen-AubartF, MartinT,etal.,FrenchVasculitisStudyGroup.Intravenous immunoglobulinasanimmunomodulatingagentin antineutrophilcytoplasmicantibody-associatedvasculitides: aFrenchnationwidestudyofninety-twopatients.Arthritis Rheumatol.2016;68:702–12.
53.HuW,LiuC,XieH,ChenH,LiuZ,LiL.Mycophenolatemofetil versuscyclophosphamideforinducingremissionofANCA vasculitiswithmoderaterenalinvolvement.NephrolDial Transplant.2008;23:1307–12.
54.HanF,LiuG,ZhangX,LiX,HeQ,HeX,etal.Effectsof mycophenolatemofetilcombinedwithcorticosteroidsfor
inductiontherapyofmicroscopicpolyangiitis.AmJNephrol. 2011;33:185–92.
55.SilvaF,SeoP,SchroederDR,StoneJH,MerkelPA,HoffmanGS, etal.,Wegener’sGranulomatosisEtanerceptTrialResearch Group.Solidmalignanciesamongetanercept-treatedpatients withgranulomatosiswithpolyangiitis(Wegener’s):long-term followupofamulticenterlongitudinalcohort.Arthritis Rheum.2011;63:2495–503.
56.LangfordCA,SnellerMC,HallahanCW,HoffmanGS, KammererWA,Talar-WilliamsC,etal.Clinicalfeaturesand therapeuticmanagementofsubglotticstenosisinpatients withWegener’sgranulomatosis.ArthritisRheum. 1996;39:1754–60.
57.LebovicsRS,HoffmanGS,LeavittRY,KerrGS,TravisWD, KammererW,etal.Themanagementofsubglotticstenosisin patientswithWegener’sgranulomatosis.Laryngoscope. 1992;10212Pt1:1341–5.
58.HoffmanGS,Thomas-GolbanovCK,ChanJ,AkstLM,Eliachar I.Treatmentofsubglotticstenosis,duetoWegener’s granulomatosis,withintralesionalcorticosteroidsand dilation.JRheumatol.2003;30:1017–21.
59.NouraeiSA,ObholzerR,IndPW,SalamaAD,PuseyCD,Porter F,etal.Resultsofendoscopicsurgeryandintralesionalsteroid therapyforairwaycompromiseduetotracheobronchial Wegener’sgranulomatosis.Thorax.2008;63:49–52.
60.WolterNE,OoiEH,WitterickIJ.Intralesionalcorticosteroid injectionanddilatationprovideseffectivemanagementof subglotticstenosisinWegener’sgranulomatosis.
Laryngoscope.2010;120:2452–5.
61.GouverisH,KaraiskakiN,KoutsimpelasD,ChongolwatanaC, MannW.Treatmentforadultidiopathicand
Wegener-associatedsubglotticstenosis.EurArch Otorhinolaryngol.2013;270:989–93.
62.MartinezDelPeroM,JayneD,ChaudhryA,SivasothyP,JaniP. Long-termoutcomeofairwaystenosisingranulomatosis withpolyangiitis(Wegenergranulomatosis):anobservational study.JAMAOtolaryngolHeadNeckSurg.2014;140:1038–44.
63.GluthMB,ShinnersPA,KasperbauerJL.Subglotticstenosis associatedwithWegener’sgranulomatosis.Laryngoscope. 2003;113:1304–7.
64.AlamDS,SethR,SindwaniR,WoodsonEA,RajasekaranK. Upperairwaymanifestationsofgranulomatosiswith polyangiitis.CleveClinJMed.2012;79Suppl3: S16–21.
65.RasmussenN.L24.Localtreatmentsofsubglotticand trachealstenosesingranulomatosiswithpolyangiitis (Wegener’s).PresseMed.2013;424Pt2:571–4.
66.MairEA.CautioninusingsubglotticstentsforWegener’s granulomatosis.Laryngoscope.2004;114:2060–1.
67.MahrA,GirardT,AgherR,GuillevinL.Analysisoffactors predictiveofsurvivalbasedon49patientswithsystemic Wegener’sgranulomatosisandprospectivefollow-up. Rheumatology(Oxford).2001;40:492–8.
68.BlignyD,MahrA,ToumelinPL,MouthonL,GuillevinL. PredictingmortalityinsystemicWegener’sgranulomatosis:a survivalanalysisbasedon93patients.ArthritisRheum. 2004;51:83–91.
69.SternA,GreenH,PaulM,VidalL,LeiboviciL.Prophylaxisfor Pneumocystispneumonia(PCP)innon-HIV
immunocompromisedpatients.CochraneDatabaseSystRev. 2014:CD005590.
70.OzakiS,AtsumiT,HayashiT,IshizuA,KobayashiS,Kumagai S,etal.Severity-basedtreatmentforJapanesepatientswith MPO-ANCA-associatedvasculitis:theJMAAVstudy.Mod Rheumatol.2012;22:394–404.
72.SociedadeBrasileiradeReumatologia&SociedadeBrasileira deImunologia.Reumatologia:GuiadeImunizac¸ãoSBIm/SBR; Magic/RM;2014/2015.
73.ZycinskaK,RomanowskaM,NowakI,RybickaK,WardynKA, BrydakLB.Antibodyresponsetoinactivatedsubunit
influenzavaccineinpatientswithWegener’sgranulomatosis. JPhysiolPharmacol.2007;58Suppl5Pt2:819–928.
74.StassenPM,SandersJS,KallenbergCG,StegemanCA. Influenzavaccinationdoesnotresultinanincreasein relapsesinpatientswithANCA-associatedvasculitis.Nephrol DialTransplant.2008;23:654–8.
75.HolvastA,StegemanCA,BenneCA,HuckriedeA,WilschutJC, PalacheAM,etal.Wegener’sgranulomatosispatientsshow anadequateantibodyresponsetoinfluenzavaccination.Ann RheumDis.2009;68:873–8.