w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Recommendations
of
the
Brazilian
Society
of
Rheumatology
for
diagnosis
and
treatment
of
Chikungunya
fever.
Part
1
–
Diagnosis
and
special
situations
Claudia
Diniz
Lopes
Marques
a,b,∗,
Angela
Luzia
Branco
Pinto
Duarte
a,c,
Aline
Ranzolin
b,d,
Andrea
Tavares
Dantas
a,
Nara
Gualberto
Cavalcanti
b,
Rafaela
Silva
Guimarães
Gonc¸alves
b,
Laurindo
Ferreira
da
Rocha
Junior
b,d,
Lilian
David
de
Azevedo
Valadares
e,
Ana
Karla
Guedes
de
Melo
f,
Eutilia
Andrade
Medeiros
Freire
g,
Roberto
Teixeira
h,
Francisco
Alves
Bezerra
Neto
i,
Marta
Maria
das
Chagas
Medeiros
j,
Jozélio
Freire
de
Carvalho
k,
Mario
Sergio
F.
Santos
l,
Regina
Adalva
de
L.
Couto
Océa
m,
Roger
A.
Levy
n,
Carlos
Augusto
Ferreira
de
Andrade
o,
Geraldo
da
Rocha
Castelar
Pinheiro
n,
Mirhelen
Mendes
Abreu
p,
José
Fernando
Verztman
q,
Selma
Merenlender
r,
Sandra
Lucia
Euzebio
Ribeiro
s,
Izaias
Pereira
da
Costa
t,u,
Gecilmara
Pileggi
v,
Virginia
Fernandes
Moc¸a
Trevisani
w,x,
Max
Igor
Banks
Lopes
y,
Carlos
Brito
a,
Eduardo
Figueiredo
b,
Fabio
Queiroga
z,
Tiago
Feitosa
aa,
Angélica
da
Silva
Tenório
a,
Gisela
Rocha
de
Siqueira
a,
Renata
Paiva
ab,
José
Tupinambá
Sousa
Vasconcelos
ac,ad,
Georges
Christopoulos
ad,aeaUniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
bUniversidadeFederaldePernambuco(UFPE),HospitaldasClínicas,Recife,PE,Brazil
cUniversidadeFederaldePernambuco(UFPE),HospitaldasClínicas,Servic¸odeReumatologia,Recife,PE,Brazil dInstitutodeMedicinaIntegralProfessorFernandoFigueira(IMIP),Recife,PE,Brazil
eHospitalGetúlioVargas,AmbulatóriodeChikungunya,Recife,PE,Brazil fUniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil
gUniversidadeFederaldaParaíba(UFPB),HospitalUniversitárioLauroWanderley(HULW),Servic¸odeReumatologia,JoãoPessoa,PB,
Brazil
hUniversidadeEstadualdeCiênciasdaSaúdedeAlagoas(UNCISAL),Maceió,AL,Brazil iUniversidadeFederaldoRioGrandedoNorte(UFRN),Natal,RN,Brazil
jUniversidadeFederaldoCeará(UFC),FaculdadedeMedicina,DepartamentodeMedicinaClínica,Fortaleza,CE,Brazil kUniversidadeFederaldaBahia(UFBA),InstitutodeCiênciasdaSaúde,Salvador,BA,Brazil
lUniversidadeEstadualdoPiauí(UESPI),FaculdadedeMedicina,Teresina,PI,Brazil mUniversidadeFederaldeSergipe(UFS),Aracaju,SE,Brazil
nUniversidadedoEstadodoRiodeJaneiro(UERJ),DisciplinadeReumatologia,RiodeJaneiro,RJ,Brazil
oFundac¸ãoOswaldoCruz(Fiocruz),EscolaNacionaldeSaúdePúblicaSérgioArouca(ENSP),RiodeJaneiro,RJ,Brazil
∗ Correspondingauthor.
E-mail:[email protected](C.D.Marques). http://dx.doi.org/10.1016/j.rbre.2017.05.006
pUniversidadeFederaldoRiodeJaneiro(UFRJ),HospitalUniversitárioClementinoFragaFilho(HUCFF),RiodeJaneiro,RJ,Brazil qHospitaldosServidoresdoEstadodoRiodeJaneiro,RiodeJaneiro,RJ,Brazil
rHospitalEstadualEduardoRabello,Servic¸odeReumatologia,RiodeJaneiro,RJ,Brazil sUniversidadeFederaldoAmazonas(UFAM),FaculdadedeMedicina,Manaus,AM,Brazil tUniversidadeFederaldeMatoGrossodoSul(UFMS),CampoGrande,MS,Brazil
uUniversidadeFederaldeMatoGrossodoSul(UFMS),HospitalUniversitárioMariaAparecidaPedrossian(HUMAP),Servic¸ode
Reumatologia,CampoGrande,MS,Brazil
vUniversidadedeSãoPaulo(USP),FaculdadedeMedicinadeRibeirãoPreto(FMRP),Servic¸odeReumatologiaeImunologiaPediátrica,
RibeirãoPreto,SP,Brazil
wUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil xUniversidadedeSantoAmaro(UNISA),SãoPaulo,SP,Brazil
yUniversidadedeSãoPaulo(USP),HospitaldasClínicas,AmbulatóriodaDivisãodeMoléstiasInfecciosasdeParasitárias,SãoPaulo,SP,
Brazil
zInstitutodeMedicinaIntegralProfessorFernandoFigueira(IMIP),HospitalMiguelArraes,Paulista,PE,Brazil aaUniversidadeFederaldePernambuco(UFPE),HospitaldasClínicas,DivisãodeGestãodoCuidado,Recife,PE,Brazil abCRPFisioterapia,RiodeJaneiro,RJ,Brazil
acUniversidadeEstadualdoPiauí(UESPI),Teresina,PI,Brazil adSociedadeBrasileiradeReumatologia,SãoPaulo,SP,Brazil aeSantaCasadeMisericórdiadeMaceió,Maceió,AL,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19December2016 Accepted22May2017 Availableonline25July2017
Keywords:
Chikungunyafever Epidemic
Consensus Brazil
a
b
s
t
r
a
c
t
Chikungunyafeverhasbecomearelevantpublichealthproblemincountrieswhere epi-demicsoccur.Until2013,onlyimportedcasesoccurredintheAmericas,butinOctoberof thatyear,thefirstcaseswerereportedinSaintMarinislandintheCaribbean.Thefirst autochthonouscaseswereconfirmedinBrazilinSeptember2014;untilepidemiological week37of2016,236,287probablecasesofinfectionwithChikungunyavirushadbeen reg-istered,116,523ofwhichhadserologicalconfirmation.Environmentalchangescausedby humans,disorderlyurbangrowthandanever-increasingnumberofinternationaltravelers weredescribedasthefactorsresponsiblefortheemergenceoflarge-scaleepidemics. Clini-callycharacterizedbyfeverandjointpainintheacutestage,approximatelyhalfofpatients progresstothechronicstage(beyond3months),whichisaccompaniedbypersistentand disablingpain.Theaimofthepresentstudywastoformulaterecommendationsforthe diag-nosisandtreatmentofChikungunyafeverinBrazil.Aliteraturereviewwasperformedinthe MEDLINE,SciELOandPubMeddatabasestogroundthedecisionsforrecommendations.The degreeofconcordanceamongexpertswasestablishedthroughtheDelphimethod, involv-ing2in-personmeetingsandseveralonlinevotingrounds.Intotal,25recommendations wereformulatedanddividedinto3thematicgroups:(1)clinical,laboratoryandimaging diagnosis;(2)specialsituations;and(3)treatment.Thefirst2themesarepresentedinpart 1,andtreatmentispresentedinpart2.
©2017PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Recomendac¸ões
da
Sociedade
Brasileira
de
Reumatologia
para
diagnóstico
e
tratamento
da
febre
Chikungunya.
Parte
1
–
Diagnóstico
e
situac¸ões
especiais
Palavras-chave: FebreChikungunya Epidemia
Consenso Brasil
r
e
s
u
m
o
Caracterizadaclinicamenteporfebreedorarticularnafaseaguda,emcercademetade doscasosexisteevoluc¸ãoparaafasecrônica(alémdetrêsmeses),comdorpersistente eincapacitante.Oobjetivodestetrabalhofoielaborarrecomendac¸õesparadiagnósticoe tratamentoda febrechikungunya noBrasil.Paraisso,foifeitarevisãodaliteraturanas basesdedadosMedline,SciELOePubMed,paradarapoioàsdecisõestomadasparadefinir asrecomendac¸ões.Paraa definic¸ãodograude concordânciafoifeitaumametodologia Delphi,emduasreuniõespresenciaiseváriasrodadasdevotac¸ãoonline.Foramgeradas 25recomendac¸ões,divididasemtrêsgrupostemáticos:(1)diagnósticoclínico, laborato-rialeporimagem;(2)situac¸õesespeciaise(3)tratamento.Naprimeiraparteestãoosdois primeirostemaseotratamentonasegunda.
©2017PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
General
considerations
Epidemiology
TheChikungunya virus(CHIKV), amemberofthe Togaviri-daefamily,Alphavirusgenus,wasfirstisolatedfromhumans in 1952 during the first urban outbreak identified in the modernscientificage,causinganepidemicthataffectedthe coastalarea ofMuawiya,Makondoand Rondo,present-day Tanzania.1 The virus name is inthe Makonde language, a
dialectspokeninSoutheasternTanzania,andmeans“tobend forward or become contorted,” an allusion to the posture adoptedbypatientsasafunctionofthejointpaincausedby infection.1Whilethediseaseistransmittedbyalargenumber
ofmosquitosofthegenusAedesinAfrica,themainvectors inBrazilareAedesaegyptiandAedeasalbopictus,thefemalesof whichareabletoinfecthumansthroughbiting.2
AfterthefirstoutbreakofChikungunyafeverinTanzania inthe 1950s,several minorepidemicsoccurred periodically until2004,whenamajoroutbreakwasidentifiedinKenya, whichthenspreadtomanyislandsintheIndianOcean,India andSoutheasternAsia.3Until2013,allthecasesinthe
Amer-icaswereimported,mostlyintotheUnitedStates;however,in Octoberofthatyear,thefirstcasesweredocumentedinSaint MartinislandintheCaribbean.Bytheendof2015,1.6million peoplehadbeeninfectedwithCHIKV,resultingin71deaths.4–6
InBrazil,thefirstautochthonouscaseswerealmost simulta-neouslyreportedinOiapoque(Amapastate–AP)andFeirade Santana(Bahiastate–BA)inSeptember2014.7Atotalof38,332
possiblecasesofChikungunyafeverwereregisteredin2015, ofwhich13,236wereconfirmed.Untilepidemiologicalweek (EW)37of2016(uptoSeptember17th,2016),236,287 proba-blecasesofinfection withCHIKVwere registered,ofwhich 116,523hadserologicalconfirmation.8
Pathophysiology
DuringtheinoculationofCHIKVthroughtheskinbymosquito bites,mosquitosalivaentersthebodytogetherwiththevirus; the salivacontains several moleculeswithanti-hemostatic andimmunomodulatingproperties,whichinduceearlycell infiltration and increased cytokine secretion. Then follows astagecharacterizedbyintensereplication ofthe virus in skinfibroblastsandmacrophagesandspreadtolymphnodes,
wherereplicationintensifiesbeforethevirusisreleasedinto the bloodstream, with spread to and consequent infection oftargetorgans,suchasthejoints andmuscles. Thevirus mightalsobedirectlyinoculatedintothebloodstreamthrough mosquito bites. Of particularrelevance is the inductionof theinnateimmuneresponse,followedbythecell-mediated immune response, involving the release of several proin-flammatorycytokines,suchasinterferonalpha,interleukins, chemokinesandgrowthfactors.9–11
Experimentalmodelsofalphavirus-inducedarthritis sug-gest that progressionto the chronic stageof Chikungunya fever results from the combination of direct cell and tis-sue damage caused by viral replication and, indirectly, by activation of the immune responsein the target tissues.12
Nevertheless, the main hypothesis involves dysregulated inflammation caused by persistent infection of tissue macrophages – or the presence of viral RNA within these cells.13 Thesynovial histopathologicalchanges after
infec-tion withCHIKVare similartothosefoundamongpatients withrheumatoidarthritis(RA)orotherchronicinflammatory jointdiseases,includingsynovialhyperplasia,vascular prolif-erationandperivascularmacrophageinfiltration.14Inanimal
modelsofCHIKVinfection,periostealnecrosis,bone prolifer-ationand multifocalbonemarrowischemiawereidentified starting5daysafterinfection.15
Clinicalmanifestations
Theincubationperiodlasts3to7days,onaverage,varying from 1to12days.16Thediseaseevolvesin3stages:acute,
lasting7to14days;subacute,whichmightlastupto3months; andchronic,namely,persistenceofsymptomsformorethan 3months.17
Acute infection is symptomatic in 80% to 97% of patients.18,19Themostcommonsymptomsarefeverof
Table1–CasedefinitionofChikungunyafever.17,45
Clinicalcriteria:feverofsuddenonset>38.5◦Candintensejointpain/arthritisofacuteonsetnotexplainedbyothermedicalconditions
Epidemiologicalcriteria:individualresidingatorvisitinganendemicorepidemicarea15daysbeforetheonsetofsymptomsorhas epidemiologicalconnectiontoaconfirmedcase
Laboratorycriteria
IsolationofCHIKVinculture CHIKVRNAbyreal-timePCR Specificanti-CHIKVIgMantibodies
Four-foldincreaseofanti-CHIKVIgGantibodiesinsamplescollectedwithatleast a10–14-dayinterval
Detectionofanti-CHIKVneutralizingantibodiesinserumbymeansofPRNT
Classification
Suspectedcase:patientmeetstheclinicalandepidemiologicalcriteria Confirmedcase:asuspectedcasethatmeetsanyofthelaboratorycriteria
Atypicalcase:laboratoryconfirmationinapatientwithotherclinicalmanifestations(neurologic,cutaneous,involvingtheheart,eyesor kidneys,respiratory,etc.)
RNA,ribonucleicacid;real-timePCR,real-timepolymerasechainreaction;PRNT,plaquereductionneutralizationtest;CHIKV,Chikungunya virus.
During the subacute stage, joint symptoms predomi-nate, occurring in up to 50% of patients infected with CHIKV.Theclinicalmanifestationsincludepersistenceofjoint pain/arthritis,bursitis, tenosynovitis,morningstiffnessand asthenia, which might exhibit continuous or intermittent progression.21,24,25
Theprevalenceofchronicjointdisordersfollowing infec-tionwithCHIKVvariesfrom14.4%to87.2%.14,19,21,23,26–30Such
a wide range of variation might be partially explained by methodologicalissues:variablesamplesize,durationoffollow up,measurestoassesschronicjointaffectionandmethods fordatacollection. Astatisticalmodeldevelopedwithdata fromobservationalstudiesestimatedthat47.6%of individ-ualswithChikungunya feverinLatinAmerica willdevelop chronicjointmanifestations.31Arecentmeta-analysis32
ana-lyzedthe prevalenceofchronicinflammatoryjoint disease (CIJD)afterChikungunyainfection(post-CHIK)in18selected studies(9prospectiveand9retrospectivecohortstudies)with a total of 5702 patients. The average length of follow up was 17.5 months; the prevalence ofpost-CHIK CIJD varied from25.3%to40.2%asafunctionofthestratificationofthe studies.
Chronic joint symptoms might translate into persistent (20–40%) or relapsing (60–80%) complaints.33,34 They may
includeoligo-orpolyarthralgiaofvariableintensity,usually symmetric,mainlyinwrists,hands,anklesandknees,and areassociatedwithmorningstiffnessandjointswelling.33Up
to72%ofpatientswithearlysignificantimprovementmight relapse,theintervallastingfrom1weektoseveralyears, pre-sentingwithvariablesymptomsandaffectingthesamejoints thathadpreviouslybeeninvolved.29,35
Althoughthepersistenceofmusculoskeletalcomplaintsis themaincharacteristicofChikungunyafever,thefactors asso-ciatedwithchronic progressionandpoorer prognosis have scarcelybeeninvestigated.Theresultsofthepublishedcase seriesindicate that somefactors aremore strongly associ-atedwithchronicprogression,suchasfemalegender,34,36–38
age over 40 years old, prominent joint involvement in the acute stage (joint swelling and stiffness, polyarthritis, tenosynovitis),32,34,36–39 presence of previous joint disease,
suchasosteoarthritis(OA),39,40andpresenceofcomorbidities,
suchasdiabetesmellitus(DM).33,35 Inturn,jointpain
with-outswellingorstiffnesswasassociatedwithhigheroddsof recovery.34
Relativetolaboratorytesting,highlevelsofC-reactive pro-tein(CRP)andpositiveCHIKVIgGserologyareconsideredtobe predictorsofchronicprogression.28,41Persistenceofpositive
CHIKVIgMbeyondtheacutestageisassociatedwitherosive arthritisandchronicprogressionofthejointsymptoms.42,43
Thediagnosis ofChikungunya fever istypicallyclinical; thecombinationofacutefeverwithintensejointpainand/or arthritisofacuteonsetarehighlysuggestiveofdisease,with highsensitivityandpositivepredictivevalueinareaswhere diseaseisendemicandepidemicsoccur.17,44Thecurrent
rec-ommendation of the Brazilian Health Ministry is to apply clinical-epidemiologicalcriteriaforthedefinitionofsuspected casesofChikungunyafever.Similarcriteriaweresuggestedat thelastexpertmeetinginNicaraguain201517,45(Table1).
Some cases might exhibit atypical progression, charac-terized bylessfrequentclinical manifestations(Table2)or signs of severity.46 The frequency of severe cases is 0.3%
and is associated with older age (>65 years old) and the presence ofcomorbidities.There are reportsofoccurrence of sepsis and septic shock in Chikungunya fever patients admittedtointensivecareunits,withnootheridentified eti-ologicalagentlikelytoaccountfortheseconditions.21,25,46–49
Useofnonsteroidalanti-inflammatorydrugs(NSAIDs)before hospitalizationand cardiovasculardiseaseare factors inde-pendentlyassociatedwithincreasedmortality.46,47Bleedingis
rare;theriskincreasesinthecaseofcoinfectionwithdengue virus,but itisnotassociatedwithcoagulationdisorders or severethrombocytopenia.25Similarlytootherviraldiseases,
suchashepatitisC,Chikungunyafeverisassociatedwitha highprevalenceofmixedcryoglobulinemia.50
Table2–MainatypicalclinicalmanifestationsofChikungunyafever.55,136,137
Organ/system Clinicalmanifestations
Skin Hyperpigmentation,aphthousulcers,transientnoseerythema,generalizederythema,vesicular-bullouslesions, palmdesquamation,lipdepigmentation,vasculitislesions,lichenoideruptions
Kidneys Kidneyfailure(maybetriggeredorworsenedbyuseofNSAIDs) Nephritis
Lungs Pneumonia
Respiratoryfailure
Gastrointestinal Diarrhea,vomiting,acutehepatitis(associatedwithCHIKV,previousalcoholismanduseofparacetamol) Heart Heartfailure,arrhythmia,perimyocarditis,ischemiccoronaryarterydisease
Neurological Encephalitis,meningoencephalitis,meningealirritation,Guillain-Barrésyndrome,cerebellarsyndrome,stroke, mentalconfusion,seizures
Eye Conjunctivitis,opticneuritis,iridocyclitis,episcleritis,retinitis,anterioruveitis Hematological Thrombocytopenia,lymphadenopathy
Someevidencehasindicatedthatchronicrheumatic dis-easesmightdevelopafterinfectionwithCHIKV.26,31,32,38,40,52,53
The pathogenesis of arthropathy following infection with CHIKVhasnotyetbeenwellelucidated;however,basedon studiesconductedwithotherarthritogenicviruses,arthritis possiblyoccursduetothevirus’abilitytoreplicateand medi-atetheproductionoftissuedamageinjoints,whichinturn dependsonthe hostimmuneresponse.54 In the published
caseseries, some patients met the criteria forRA23,29 and
spondyloarthritis(SpA).19,20,29,52 duringthechronicstageof
disease.Therearealsoreportsofexacerbationofcutaneous psoriasisandofonsetofpsoriasisafteranepisodeof Chikun-gunyafever.55,56
During the epidemic that occurred in Reunion Island, Javelleetal.29formulatedcriteriaforundifferentiated
inflam-matory arthritis (non-validated) (Table 3) to classify the patients who did notmeet the criteria forRA or SpA and thusdistinguishthosewithinflammatorydiseasefromthose withjointpain only.Accordingto suchcriteria, polyarticu-larinflammationlastingmorethan3monthsaftertheacute stageofChikungunyafeversuggestsapotentialdiagnosisof post-CHIKCIJD.Morningstiffnesswasconsideredtobethe clinicalmanifestationwiththelowestdiagnosticpowerdue toitshighprevalenceinthepost-CHIKperiod,whensynovitis andtenosynovitiswerehighlyindicativeofCIJD.Thiswas con-firmedbyultrasonographytodistinguishCIJDfromsofttissue edema,whichisalsocharacteristicofdisease.29Thesecriteria
areratherunspecificandwerenotvalidatedwithother popu-lations;theiraccuracyinclinicalpracticecannotbeasserted withprecision.Thus,werecommendcautionwhentheyare appliedbecausepatientswithotherchronicinflammatory dis-easesmightbeeasilymisclassifiedasChikungunyafever.
ToinvestigatethebehaviorofChikungunyafeverinBrazil and collect data to ground future therapeutic decision-making,amulticentercohortstudy– CHIKBRAZILCOHORT – was launched in April 2016. The sample is composed ofBrazilianpatients withCHIKVinfectionand joint symp-toms. In its initial stage, 6centers from 4Brazilian states (Pernambuco,Paraíba,CearáandSergipe)participatedinthe study,andpatientswereincludedwhentheyhada clinical-epidemiologicaldiagnosisofChikungunyafever17andchronic
joint symptoms. Upto thepresent time,431 patientshave been included, andthe correspondingdata areperiodically collectedandanalyzed(theseanalyseshavenotyetbeen pub-lished).
Methods
Toelaboratethepresentrecommendations,3workinggroups wereestablished:acoregroup,aliteraturereviewgroupand avotingpanel.Thecoregroupwascomposedof5 rheuma-tologists(CDLM,ALBPD,VMT,JTSV,GC)andwaschargedwith formulatingandsendingtheleadingquestionsthatservedas thebasisforformulationoftherecommendations, coordinat-ingandsupervisingtheother2groups,conductingthevoting panelsandwritingthemanuscript.Thegroupthatperformed theliteraturereviewincluded20rheumatologistsand3 physi-caltherapists.Thesearchwasconductedinseveraldatabases (MEDLINE,SciELO,PubMed,EMBASE),andarticlesonthe diag-nosisandtreatmentofChikungunyafeverwereselectedin additiontoabstractspublishedinconferenceproceedingsin Portuguese,English,FrenchorSpanishthroughOctober2016.
Table3–Criteriafortheclassificationofpost-Chikungunyachronicinflammatoryjointdisease(CIJD).29
>4jointswitharthritis+symptomduration≥6weeks+noalternativediagnosis
A.Arthritis=1inflammationcriterion
•Synovitisa
•Heatand/orerythemaonthejoint •Morningstiffness>30min
•Inflammatorypain–improveswithexerciseandworsenswithrestorduringthenight
B.Patientdoesnotmeetthecriteriaforrheumatoidarthritisorspondyloarthritis,inadditiontorulingoutothercausesofpolyarthritis:gout,autoimmune diseases,thyroiddysfunction,chronicviralhepatitis,andsarcoidosis
Thisgroupwaschargedwithreviewingtheevidencetoprovide theoreticalgroundsforthefinalrecommendations.
Themethodologicalqualityoftheidentifiedstudieswas subjectedtocriticalassessmentbasedontheriskofbiasin clinicalinterventionstudiesandSTROBE(Strengtheningthe ReportingofObservationalstudiesinEpidemiology).57Asthe
methodological diversity of the studies did not allow per-formingameta-analysis,the assessmentwasbasedonthe levelsofevidenceandgradesofrecommendationformulated bytheOxfordCentreforEvidence-BasedMedicine,2011(Levelsof Evidence).58 Here,thestudiesareclassifiedintolevelsof
evi-dence1–5basedontheirtypeandabilitytorespondtothe correspondingquestionandtoproducethebestevidenceto grounddecision-making.Asinthepresentrecommendations, weusedstudieswithdifferentlevelsofevidence,andwechose toindicatethevariouslevelsofevidencethatgroundedthe finalrecommendationsin2ways:sequentially,i.e.,separated byacomma,orasaninterval,asindicatedbyahyphen.
Duetothelowqualityofthelocatedevidence,ora com-plete lack of evidence in some cases, we also employed the preliminary analyses of the CHIKBRAZIL cohort data (describedalongthetext,especiallyasconcernstreatment) and the opinions of the participating experts to ground decision-makingvis-à-vistherecommendations.
TheDelphimethodwas usedtoestablish the degreeof expertconcordanceat2in-personmeetingsandinvarious onlinevotingrounds.Thevotinggroupincludedallthe mem-bersoftheother2groupsinadditionto3generalpractitioners, 1 specialist in infectious diseases and 1 representative of publichealthmanagement. The2in-personmeetingswere conductedinRecife,Pernambuco state,Brazil(Octoberand November2016);therateofattendancewasover90%.In addi-tiontoin-personvoting,severalroundsofquestioning,voting andamendmentswereconductedviatheinternet.Toassess thedegreeofexpertconcordance,theparticipantsinthe vot-ingpanelwererequestedtoattributescoresfrom0to10on acontinuousscale,zerorepresenting“Ifullydisagree”and10 “Ifullyagree.”Themeanandstandarddeviation(SD) corre-spondingtoeachrecommendationwerecalculatedfromthe individualscores.
Atotalof25recommendationswereformulatedand classi-fiedinto3thematicgroups:A.Clinical,laboratoryandimaging diagnosis;B.Specialsituations;andC.Treatment.
Thepresent articleincludesthefirst2themes(Table4), comprising14recommendations;therecommendations for treatmentaredescribedinpart2.
To facilitate the reading of the text, the levels of evi-denceofthe studiesusedtoground therecommendations areindicatedinthelistofreferences.References correspond-ing to guidelines, treatment protocols, abstracts published inconferenceproceedingsand thosenotdirectlyrelatedto Chikungunyafeverwerenotclassified.
Recommendations
A.Clinical,laboratoryandimagingdiagnosis
A.1 Possible occurrence of Chikungunya fever should be strongly considered in caseswith acute fever, severe joint
pain/arthritisandwithorwithoutexanthemawithinthe con-text of an epidemic. However, other acute febrile diseases ought to be considered in the differential diagnosis, espe-cially asconcernsthesevere oratypical cases.Concordance: 9.31(SD±1.168);levelofevidence(2–4)
ThesymptomstypicaloftheacutestageofChikungunya fever (fever,exanthemaandjointpain)mightalsooccurin other viral diseases,dengue fever (DENV)in particular.59,60
While many symptoms and signs are similar,some mani-festationsare morecharacteristic,whichmighthelpinthe differentialdiagnosisbetweenbothconditions.Odynophagia, cough,nausea,vomiting,diarrhea,abdominalpain,anorexia and tachycardiaare morecommonindenguefeverthanin CHIKVinfection.61Inaddition, indenguefever,thefeveris
usuallylower;theskinrashappearslater(fromdays5to7); andretro-orbitalpain,thrombocytopeniaandneutropeniaare morefrequent.62,63AstheZikavirus(ZIKV)inBrazilcoexists
withinoneandthesameepidemic,itshouldalsobe consid-eredinthedifferentialdiagnosis.InthecaseofZIKV,thefever ismilderormightevenbeabsent,thejointandmusclepainis notdebilitating,andhyperemiaoftheconjunctivaiscommon; manifestationsmightincludeskinrash,whichisalsoitchy.64
CoinfectionwithCHIKVandZIKVand/orDENVmightoccur inepidemicsofarboviraldiseases.62–64
In addition to DENVand ZIKV,other arboviruses might causesymptomssimilartothoseoftheacutestageof Chikun-gunyafever,suchasRossRivervirus,BarmahForestvirus, O’nyong-nyongvirus,SindbisgroupandMayarovirus.60From
these,theonlyonefoundinBrazilisMayarovirus(MAYV), whichcausesMayarofeverthat,inadditiontoacute symp-toms similarto those ofCHIKV, alsoexhibits arthritogenic characteristics withpossible chronic progression.However, Mayarofeverpredominantlyoccursinwildareasandis gener-allylimitedtosmallepidemics.65InBrazil,MAYVtransmission
isrestrictedtotheNorthernarea,66althoughithasalready
beendetectedinstatesfromotherregions.67,68
Other causes of acute febrile viral diseases, such as thosecausedbyadenoviruses,enteroviruses,parvovirusB19, measlesandrubella,shouldbeconsideredinthedifferential diagnosisofChikungunyafever,forwhichpurposedata,such ashistoryofexposure,recenttravelsandgeographicalareaof residence,shouldbetakenintoaccount.69
Inadditiontoviraldiseases,acutebacterialinfections,such asleptospirosis,andparasiticdiseases,suchasmalaria,might beattendedwithclinicalmanifestationssimilartothoseof theearlystageofChikungunyafever,suchashighfever, mus-clepain,jointpain,headache,fatigue,diarrheaand,insome cases, abdominalpain,forwhich reasonshould be consid-eredinthedifferentialdiagnosis,especiallyasconcernsthe atypicalcases.70,71
Table4–SummaryofrecommendationsfordiagnosisofandspecialsituationsforChikungunyafever.
Recommendations
A.Clinical,laboratoryandimagingdiagnosis
A.1.PossibleoccurrenceofChikungunyafevershouldbestronglyconsideredincaseswithacutefever,severejointpain/arthritiswithor withoutexanthemawithinthecontextofanepidemic.However,otheracutefebrilediseasesoughttobeconsideredinthedifferential diagnosis,especiallyasconcernssevereoratypicalcases.Concordance:9.31(SD±1.168);levelofevidence(2–4)
A.2.InpatientswithclinicalsuspicionofacuteChikungunyafever,laboratoryassessment(completebloodcount,liverenzymes, creatinine,fastingglycemia,erythrocytesedimentationrate(ESR)/CRP)shouldbedecidedonacase-by-casebasisaccordingto comorbiditiesandsignsofseverity.Concordance:7.12(SD±3.5);levelofevidence(3,4)
A.3.CHIKVshouldonlybeinvestigatedincasesforwhichdiagnosticconfirmationattheacutestageisneeded:atypicalcases, differentialdiagnosisinthecaseofseverepresentationortoestablishpublichealthpolicies(suspicionofnewfociorpost-epidemic cases),inwhichcasethefirst-choicemethodisreal-timePCRthatshouldbeperformedwithinthefirstweekoftheappearanceof symptoms.Concordance:9.19(SD±0.839);levelofevidence(2,3)
A.4.RelativetoacutecasesofChikungunyafever,serology(ELISA)forCHIKV(IgMandIgG)shouldonlybeperformedincaseswith atypicalpresentationorwhendifferentialdiagnosisisneeded;insuchcases,itshouldbeperformedafterthetenthdaysincetheonset ofsymptoms.Relativetochroniccases,serologyisrecommendedforthepurposeofconfirmatorydiagnosis,butnottostarttreatment.
Concordance:9.29(SD±1.510);levelofevidence(2–4)
A.5.DuringthechronicstageofChikungunyafever,autoantibodiesshouldonlybeinvestigatedwhendifferentialdiagnosiswithspecific rheumatologicdiseasesisnecessarywithcompliancewiththeavailableconsensuses/guidelines.Concordance:8.55(SD±2.593);levelof evidence(3,4)
A.6.IntheacuteandsubacutestagesofChikungunyafever,mostpatientsdonotneedimagingtests.Inthechronicstageofdisease,plain radiographyshouldberequestedbytherheumatologistonthefirstvisitforinitialstructuralandpreexistingdamageassessment.
Concordance:9.70(SD±0.651);levelofevidence(3,4)
A.7.Musculoskeletalultrasoundmightcontributetotheassessmentofjointandperiarticularabnormalitiesatanystageof
Chikungunyafever.Intheacutestageofdisease,itistheonlyimagingtestthatmightbeperformedaccordingtothedoctor’sopinion, beingparticularlyusefulforthedifferentialdiagnosisoflowerlimbswelling.Concordance:9.29(SD±1.510);levelofevidence(3,4)
B.Specialsituations
B.1.InthetreatmentofpregnantwomenwithChikungunyafever,theriskposedbymedicinestothefetusshouldbetakenintoaccount; whenindicated,analgesics,prednisone/prednisoloneandhydroxychloroquinemaybeused.Concordance:9.71(SD±0.534);levelof evidence(3,4)
B.2.Byitself,Chikungunyafeverisnotanindicationofcesareansection,theneedofwhichshouldbeestablishedonobstetricalgrounds only.Breastfeedingisallowed.Concordance:9.67(SD±0.547);levelofevidence(3–4)
B.3.Relativetotheelderly(>60yearsold)withChikungunyafever,strictclinicalmonitoringofmedications,comorbiditiesandhigherrisk ofcomplicationsisrecommendedatallstagesofdisease,theacutestageinparticular.Concordance:9.61(SD±0.737);levelofevidence(3,4)
B.4.Childrenunder2yearsoldshouldreceivespecialattentionduetotheirhigherriskofsevereandatypicalmanifestations, involvementofthecentralnervoussystem(CNS)inparticular.Concordance:9.30(SD±1.179);levelofevidence(3,4)
B.5.NewborninfantsfrommotherswithclinicalmanifestationssuggestiveofChikungunyafeverclosetolaborshouldbesubjectedto closeobservationalongthefirst5daysoflife.Rationaluseofmedicationsshouldbeperformedforcasesthatdevelopdisease;complex casesshouldbemanagedattheintensivecareunit.Concordance:9.54(SD±0.838);levelofevidence(3,4)
B.6.TreatmentfortheacutestageofChikungunyafeverinchildrenconsistsofhydration,analgesicsandantipyreticagents;salicylates shouldbeavoided.Forthechronicstage,wesuggestfollowingtherecommendationsforadults,whiletakingtheparticularitiesinherent tothisagerangeintoaccount.Concordance:9.48(SD±0.785);levelofevidence(3,4)
B.7.Werecommendpayingspecialattentiontopatientswithpreviousdiagnosisofrheumatoidarthritis,spondyloarthritisorsystemic lupuserythematosus,astheseconditionsmightbecomereactivatedorexacerbated.Concordance:9.42(SD±1.840);levelofevidence(3,4)
Initssubacuteandchronicstages,theclinical manifesta-tionsofCHIKVinfectionmightbesimilartothoseofseveral chronicrheumaticdiseases.Symmetricalarthritisinvolving thehands,wrists,kneesandankles,combinedwithmorning stiffness,arefoundinRAandalsoinarthropathysecondary to CHIKV infection. Enthesis and fascia involvement and thepresenceofinflammatorylumbarpaininpatientswith CHIKVinfectionmightsimulateSpA,especiallyamongyoung malepatients.20,29Notably,theonsetofspecifictreatmentof
suchcasesmightbedelayed duetomistaken diagnosis as Chikungunyafever,amistakeinducedbytheepidemiological situation.72
A.2.Inpatientswithclinicalsuspicionoftheacutestage ofChikungunyafever,laboratoryassessment(completeblood count,liverenzymes,creatinine,fastingglycemia,erythrocyte sedimentationrate(ESR)/C-reactiveProtein(CRP))shouldbe decidedonacase-by-casebasisaccording tocomorbidities andsignsofseverity.Concordance:7.12(SD±3.5);levelofevidence (3,4)
For laboratorytestingdecisionsincasesofChikungunya fever,theclinicalmanifestationsandstageofdiseaseshould betakenintoconsideration.Asdiagnosisintheacutestage isestablishedbasedonclinical-epidemiologicalcriteriaand thespecificityoftestsislowinthisstage,nolaboratorytest isneededfornon-complicatedtypicalcases.Relativeto high-riskpatients(elderly,pregnantwomen,childrenunder2years old,presenceofcomplications),onlycomplete bloodcount (CBC)isrecommended.Morethoroughlaboratory investiga-tionmightbeneededasafunctionoftheoverallconditionof thepatients,comorbiditiesandmedicationsused,especially inthecaseofelderlypatients.17,24
ThemostfrequentlaboratoryfindinginChikungunyafever is lymphopenia, which ismost intenseduring the viremic stage.4Unlikedenguefever,thrombocytopeniaislessfrequent
whorequirehospitaladmission.25,26,49,73,74Relativeto
inflam-matoryactivitytests,ESRwasfoundtobeelevatedinmost patientsduringthefirst10monthsofdiseaseinastudy con-ductedinIndia.23ElevatedCRPlevelsweredetectedinmore
than70%ofpatients.20,26
Inthe chronic stage,in additionto routinetestes(CBC, ESR,CRP),investigationofautoantibodiesshouldbe consid-eredwhentheclinicalpresentationissuggestiveofCIJDand accordingtotheexistingcomorbidities.Synovialfluid analy-sismightbenecessarytoconfirmtheinflammatorynatureof jointinvolvementandhelpindifferentialdiagnosis(i.e.,gout orsepticarthritis).
A.3.CHIKVshouldonlybeinvestigatedincasesforwhich diagnosticconfirmationintheacutestageisneeded:atypical cases,differentialdiagnosisinthecaseofseverepresentation ortoestablishpublichealthpolicies(suspicionofnewfocior post-epidemiccases),inwhichcasethefirst-choicemethodis real-timePCRthatshouldbeperformedwithinthefirstweek oftheappearanceofsymptoms.Concordance:9.19(SD±0.839); levelofevidence(2,3)
ConfirmatorydiagnosisofinfectionwithCHIKVmightbe establishedbymeansof3mainlaboratorytests:virus isola-tion,moleculartechniquesforviralgenomic RNAdetection (real-timePCR)andserology.75
VirusisolationthroughthedetectionofviralRNAmightbe performedonserumsamplesduringtheacutestageof dis-ease(≤8days)76;however,thismethodisnotusedinclinical
practice.
Real-timePCRforthedetectionofviralgenomicRNAhas severaladvantagescomparedtoconventionalPCR:fasterto perform,quantitative,lowcontaminationrisk, simple stan-dardizationandhighsensitivity/specificity.Bymeansofthis technique,thepresenceofviralRNAcanbedetectedduring theearlystageofviremia(0–7days).77
Consideringthatthesymptomsassociatedwitharbovirus infection(CHIKV,DENVandZIKV)mightbequitesimilar, espe-ciallyintheearlystagesofdiseasewhendifferentialdiagnosis isnecessary,triplereal-timePCRisthemostadvantageous techniquebecauseitsimultaneouslyidentifiesRNAfromall3 viruses.78–80
Asafunctionoftheknowndifficultyinperforming real-time PCR in clinical practice, including high cost and no accesstomostofthepopulation, werecommend perform-ingconfirmatorydiagnosisofacutecasesonlyforatypicalor severecasesduringepidemicsorforspecialsituations (chil-drenunder2yearsold,pregnantwomen,suspectofnewfoci, post-epidemiccases).Insuchcases,samplecollectionshould beperformedwithinthefirst6daysoftheonsetofsymptoms. A.4.RelativetoacutecasesofChikungunyafever,serology (ELISA)forCHIKV(IgMandIgG)shouldonlybeperformedin caseswithatypicalpresentationorwhendifferential diagno-sisisneeded;insuchcases,itshouldbeperformedafterthe tenthdaysincetheonsetofsymptoms.Relativetochronic cases,serologyisrecommendedforthepurposeof confirma-torydiagnosis,butnotto starttreatment. Concordance:9.29 (SD±1.510);levelofevidence(2–4)
Accordingtothecurrentrecommendationsbythe Brazil-ianMinistryofHealth,inthe face ofanepidemic, specific serologyforCHIKVduringtheacutestageofinfectionshould
onlybeperformedforatypical casesandcomplicated clin-ical situations.17 However, in areas where arboviruses are
endemic,accurateidentificationofthespecifictypeof infec-tionishighlyrelevantforthepurposeofpatientmanagement, especiallyforcasesthatprogresstothechronicstage,inorder to implement adequate public healthmeasures and guide healthmanagers.66
Inpractice,serologyisthemostwidelyusedmethodfor confirmatory diagnosis ofCHIKVinfection.ELISA (enzyme-linked immunosorbent assay) and the plaque reduction neutralizationtest(PRNT)mightbeusedforthispurpose.17
IgMantibodies are detectedin4%to20% ofcasesfrom day3onward,reaching80%positivityafterthefirstweek.81,82
Higher levels are detectedfrom week3to5,and the anti-bodiesmightremainelevatedfor1to3monthsorlongerin somecases.IgGantibodiesarealsodetectedstartingweek1 afterinfection,usually1or2daysaftertheelevationofIgM antibodies,andmightremaindetectableforseveralyears.81–83
SerologyforCHIKVcanbeperformedstarting5daysafter theonsetofsymptoms.However,toobtainabetteroperational performanceofthistest,itshouldbeperformed7to10days aftertheonsetofsymptomsforIgMantibodiesand10to14 daysforIgGantibodiesforELISA,especiallyinareaswhere otheralphavirusesdonotcirculate.Thesensitivityofthetest variesfrom85%to98%,withspecificityabove90%.14,65,81–88
PersistenceofaspecificIgMresponseseveralmonthsafterthe initialinfectionwasfoundinsomepatientswithchronic mus-culoskeletalsymptoms.84Themeaningofthisphenomenonis
notyetclear;accordingtothemostwidelyaccepted hypothe-sis,itdenotespersistenceofthevirusinsometissuesthrough stillpoorlyunderstoodmechanisms.84,88
Coinfection with other arboviruses is an occurrence in areasendemicforChikungunyafever,denguefeverandZika. CHIKV is an alphavirus; as such, it might exhibit cross-reactivity withother virusesfrom thisfamily.65,88 InBrazil,
themostfrequentofsuchvirusesisMayarovirus,whichalso causesfeverand(limited)jointpain;itscirculationislimited totheNorthernregionofthecountry,66althoughithasalready
beendetectedinstatesfromotherregions.67,68
A studygroup from FederalUniversity ofRiode Janeiro (Universidade Federal doRio de Janeiro –UFRJ) reported a case series with 30 patients from areas endemic forZIKV, CHIKVand DENVcoinfection.DENVRNAwas notdetected inanyoftheclinicalsamples,whileZIKVRNAwasdetected in17samples(56.7%).ZIKVandCHIKVcoinfectionwas doc-umentedin1case.Fromthe17ZIKV-positiveindividuals,8 exhibited reactivityforanti-DENV IgM,which issuggestive ofrecentinfectionwithDENV,cross-reactivityorcoinfection. These findingsreinforcethe relevanceoflaboratorytesting forconfirmatorydiagnosis,especiallyforcasesoriginatingin areasendemicforall3arboviruses.75
PRNT,developedin1959byHendersonandTaylor,89
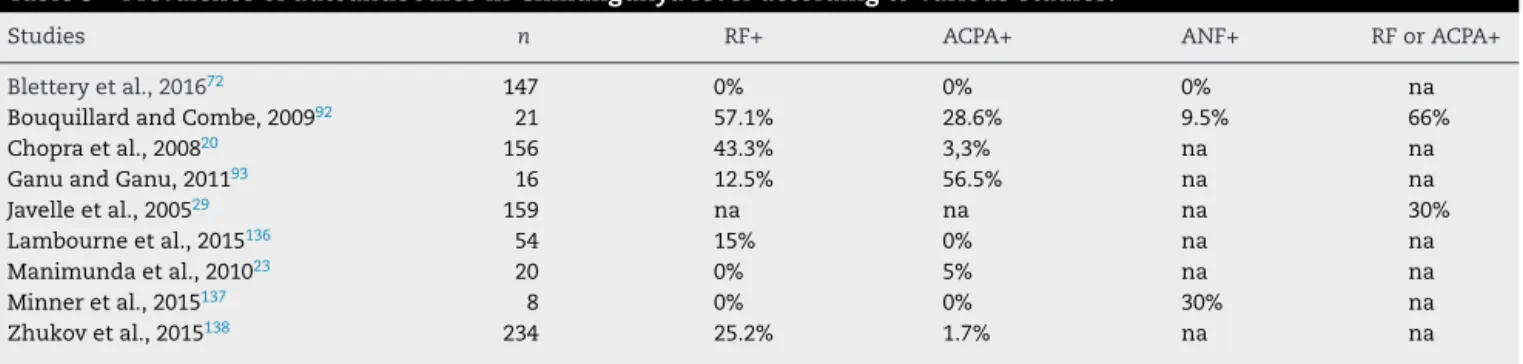
Table5–PrevalenceofautoantibodiesinChikungunyafeveraccordingtovariousstudies.
Studies n RF+ ACPA+ ANF+ RForACPA+
Bletteryetal.,201672 147 0% 0% 0% na
BouquillardandCombe,200992 21 57.1% 28.6% 9.5% 66%
Chopraetal.,200820 156 43.3% 3,3% na na
GanuandGanu,201193 16 12.5% 56.5% na na
Javelleetal.,200529 159 na na na 30%
Lambourneetal.,2015136 54 15% 0% na na
Manimundaetal.,201023 20 0% 5% na na
Minneretal.,2015137 8 0% 0% 30% na
Zhukovetal.,2015138 234 25.2% 1.7% na na
n,numberofpatients;RF,rheumatoidfactor;ACPA,anti-citrullinatedproteinantibodies;ANF,antinuclearfactor;na,notassessed.
throughPRNTisconfirmedwhenthetiterincreases4times fromtheacutestagetoconvalescence.76
Arecent study conductedin the Philippinesfoundthat PRNTmightbeusefulfordetectingcasesofsubclinical infec-tion.Thesamplecomprised853randomlyselectedindividuals before the onset of symptoms suggestive of Chikungunya fever duringan epidemicin 2012.Twelve months later,19 symptomaticcasesand87casesofsubclinicalinfectionwere identified. Positive PRNT at inclusion was associated with 100% (95% confidence interval – CI: 46.1, 100.0) protection againstsymptomaticinfection.Thesedatamightberelevant toassesstheimpactofdisease,understandthevirus’ trans-missionandtohelpinthedevelopmentofavaccineagainst CHIKV.91
AsPRNT hashigh cost,isdifficulttoperformand inter-pret and has limited access, the first-choice serological methodmustbebasedonimmunoenzymaticassays(ELISA), which have low cost, are widely accessible and are sim-pleto perform.65,84 As inthe case ofCHIKVdetection, we
recommendperforming serology during the acutestage of Chikungunyafeveronlywhendifferentialdiagnosisis neces-saryorforatypicalcases.Fortypicalcases,diagnosisshould beestablishedbasedontheclinical-epidemiologicalcriteria (Table5).
A.5. During the chronic stage of Chikungunya fever, autoantibodiesshouldonlybeinvestigatedwhendifferential diagnosiswithspecificrheumatologicdiseases isnecessary withcompliancewiththeavailableconsensuses/guidelines. Concordance:8.55(SD±2.593);levelofevidence(3,4)
Dataonthe presenceofautoantibodiesinpatients with Chikungunyafeverarescarceandratherconflicting,likelyas aresultofdifferencesamongthepopulationgroupsassessed andinthedesignofstudies,mostofthemhavinga retrospec-tivedesignandconsistingofcaseseries.Preliminaryresultsof theCHIKBRAZILcohortstudy,whichthusfarhasincluded430 patientswithChikungunyafeverfrom4Brazilianstate capi-tals,detectedrheumatoidfactor(RF)in28.3%of113patients whoperformedthetest,antinuclearfactor(ANF)in33.3%of 66patientsandanti-citrullinatedproteinantibody(ACPA)ina singlepatient(unpublisheddata).
Table5describestheresultsofautoantibodytestingin sev-eralcohortsofpatientswithChikungunyafever.
Consideringtheavailabledata,RFandACPAshouldonly be investigated in cases with persistent synovitis in 1 or morejointsinthechronicstageofdiseasedespiteadequate treatment.ANFshouldonlybemeasuredforthepurposeof
differential diagnosisrelativetocaseslastingmorethan 12 weeksandwithoutadefinitivediagnosis.Inadditiontothese autoantibodies,investigationofHLA-B27isrelevantincases withclinicalmanifestationssuggestiveofSpA.24
A.6. In the acute and subacute stages of Chikungunya fever,mostpatientsdonotneedimagingtests.Inthechronic stageofdisease,plainradiographyshouldberequestedbythe rheumatologistonthefirstvisitforinitialstructuraland pre-existing damageassessment. Concordance: 9.70 (SD±0.651); levelofevidence(3,4)
A.7. Musculoskeletalultrasound mightcontributeto the assessment ofjoint and periarticular abnormalities at any stageofChikungunyafever.Intheacutestageofdisease,it istheonlyimagingtestthatmightbeperformedaccordingto thedoctor’sopinion,beingparticularlyusefulfordifferential diagnosisoflowerlimbswelling.Concordance:9.29(SD±1.510); levelofevidence(3,4)
The studies conducted up to the present time did not establishaprotocoldefiningwhenplainradiographsshould beperformed. Radiographstakenduringtheacutestageof disease did not evidence erosions, and the occurrence of the latter in the chronic stage diverges among published studies.20,29,72,92 Inthe study conducted inReunion Island,
somepatientsexhibitedpartialortotalrecoveryofthebone lesionsaftertreatment,whilethedegreeofbonedestruction becameworseinothersevenwithtreatment.29
Radiographic abnormalities associated with arthropathy secondarytoCHIKVinfectionwerefoundinimagesmainly takenafter3monthsto2yearsofdisease.93Ina
retrospec-tivestudy,theaveragetimetoradiologicaldiagnosisofjoint lesions fromthe acutestagewas45 months.29 Asaresult,
radiographsarenotsuggestedforpatientsintheacutestage ofdisease.Relativetopatients withless than3monthsof disease,radiographsarerecommendedforselectsituations, suchasthepresenceofcomplications,doubtsaboutdiagnosis andassessmentoftheindicationofearlytreatment.As con-cernspatientsinthechronicstageofdiseaseandlong-lasting symptoms,plainradiographsshouldbetakenasafunctionof thepatternofinvolvementtoassesstheprogressionofjoint damageasneeded.24,29
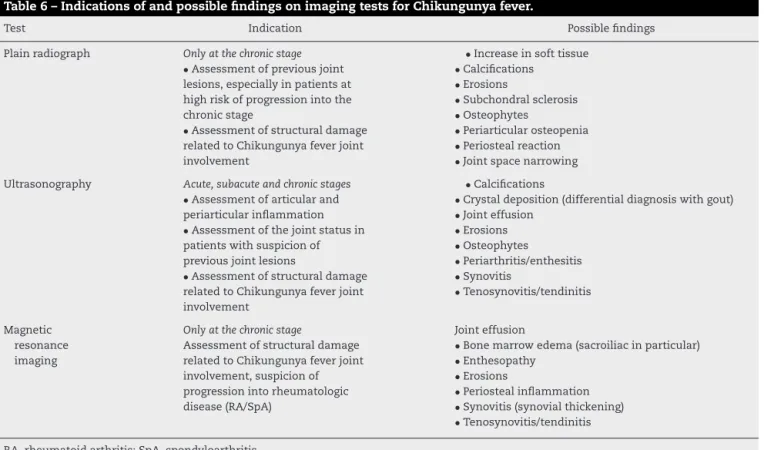
Table6–IndicationsofandpossiblefindingsonimagingtestsforChikungunyafever.
Test Indication Possiblefindings
Plainradiograph Onlyatthechronicstage
•Assessmentofpreviousjoint lesions,especiallyinpatientsat highriskofprogressionintothe chronicstage
•Assessmentofstructuraldamage relatedtoChikungunyafeverjoint involvement
•Increaseinsofttissue •Calcifications
•Erosions
•Subchondralsclerosis •Osteophytes
•Periarticularosteopenia •Periostealreaction •Jointspacenarrowing
Ultrasonography Acute,subacuteandchronicstages
•Assessmentofarticularand periarticularinflammation •Assessmentofthejointstatusin patientswithsuspicionof previousjointlesions
•Assessmentofstructuraldamage relatedtoChikungunyafeverjoint involvement
•Calcifications
•Crystaldeposition(differentialdiagnosiswithgout) •Jointeffusion
•Erosions •Osteophytes
•Periarthritis/enthesitis •Synovitis
•Tenosynovitis/tendinitis
Magnetic resonance imaging
Onlyatthechronicstage
Assessmentofstructuraldamage relatedtoChikungunyafeverjoint involvement,suspicionof progressionintorheumatologic disease(RA/SpA)
Jointeffusion
•Bonemarrowedema(sacroiliacinparticular) •Enthesopathy
•Erosions
•Periostealinflammation •Synovitis(synovialthickening) •Tenosynovitis/tendinitis
RA,rheumatoidarthritis;SpA,spondyloarthritis.
activity,boneerosionsandligamentandtendonlesionsdueto Chikungunyafever.Itfurtherhelpstoelucidatedoubtsabout thediagnosisanddetectpreviouslesions.22,46,94Intheacute
stageofChikungunyafever,it enablesassessinglowerlimb swellingandhelpsinthedifferentiationamongarticularand periarticularlesions andedemaofvascular origin (expert’s opinion).
InaUSGstudyconductedinMartinique,whichassessed articular manifestationsduringthe acute stage of Chikun-gunyafever in 28 patients (average lengthof disease:6.15 days),jointeffusionwasdetectedin92.8%ofthesample. Peri-arthritisoftheanklewaslessfrequent(28%),only2patients exhibited tenosynovitis and no instances of erosions were found.95
Thefewstudiesthatassessedtheindicationofmagnetic resonanceimaging(MRI)inchronicarthropathysecondaryto CHIKVinfectionaredescriptive,donotestablishthe superi-orityofthismethodoverUSGanddonotdefinetheneedto includeimagingmethodsinthefollowupofpatients.In addi-tion,oneneedstotakeintoaccountthecostandavailabilityof tests,aswellastheexaminer’sexperienceintheselectionof themostadequatemethodforimagingassessmentona case-by-casebasis.23,27TheMRIabnormalitiesthatmightbefound
inpatients withChikungunya feverare similar tothose of inflammatoryjointinvolvement,RAinparticular.23,24,27,42,72,93
Table6describestheindicationsandpossiblefindings accord-ingtoclinicalstageandtypeofimagingmethodused.
B.Specialsituations
B.1. In the treatment of pregnant women with Chikun-gunyafever,theriskposedbymedicinestothefetusshould
be taken into account; when indicated, analgesics, pred-nisone/prednisolone andhydroxychloroquine may beused. Concordance:9.71(SD±0.534);levelofevidence(3,4)
B.2.By itself, Chikungunyafever is notanindicationof cesareansection,theneedofwhichshouldbeestablishedon obstetricalgroundsonly.Breastfeedingisallowed.Concordance: 9.67(SD±0.547);levelofevidence(3–4)
During an outbreak that took place in Thailand in 2009–2010, an epidemiological survey of dengue fever and Chikungunyafeverwasperformedamongwomenwho deliv-ered infants from November 2009 through May 2010. The mothers were subjected to serology testing; the umbilical cordbloodwasalsotestedfortheCHIKV-positivecases.The seroprevalenceofCHIKVwas71.2%;noinstanceofthemost frequentobstetricalcomplicationsoccurred,andspecificIgM wasnotdetectedintheumbilicalcordbloodsamples.96
In2015,Dotters-Katzetal.97reviewedobstetricalaspects
relatedtoChikungunyafeverbysearchingEnglisharticleson thesubjectofinterestbasedonthePRISMAcriteria.Intotal,25 articleswereanalyzed.Theresultsshowedthatdespite indi-cationssuggestingthatdiseaseismoresevereinindividuals withchronicdiseases,elderlyandchildren,itdoesnotseemto bemoresevereamongpregnantwomen,althoughtherewere nocomparativestudieswithnon-pregnantwomen.
Furthermore,thegestationaloutcomesdidnotseemtobe influenced byCHIKVinfection.In aprospectivestudy con-ducted inReunionIsland, Fritelet al.98 comparedpregnant
congenitaldefects,prematurityorotherdisorders.Inanother prospective study by Gérardin et al.,99 also performed in
ReunionIsland,maternalviremiaintrapartumwasassociated withahigherincidenceofabnormalitiesofthefetalheartrate, whichdoubledthefrequencyofcesareansections;thiswas thesingledifferencefound.
Thepregnancytrimester inwhichinfection withCHIKV occursisthemainpredictoroffetaloutcome.Theviruscan crosstheplacentalbarrierinthefirstandsecondtrimesters and cause fetal infection and miscarriage, which are con-sidered to be rare occurrences. However, maternal active infectionupto4daysafterdeliveryincreasestheriskof ver-ticaltransmission, theincidence ofwhich variesfrom 27% to48%amongthevariouspublishedcaseseries.97,99–103
Ver-ticaltransmissionshouldbesuspectedwhenthesymptoms ofdiseasemanifestwithinthefirstweekoflifeandthereis noevidenceofamosquitobite.103 Ascesareansectiondoes
notpreventverticaltransmission,104,105 itisnotmandatory
forcasesofChikungunyafever;rather,itshouldbeperformed asperobstetricalindications.ThetransmissionofCHIKVby mother’smilkisstillunderdiscussion.97
Thetreatmentofpregnantwomenwithchronic Chikun-gunyafevershould takeinto accountthe knowneffects of medicinesonthefetus.Itisrecommendedtostartanalgesic treatmentintheacutestageofdiseasewithparacetamol,with amaximumdoseof4g/day.NSAIDsarecontraindicatedfrom gestationalweek24 onwarddue totheriskoffetal kidney failureandprematureclosureoftheductusarteriosus.24The
useofnon-selectiveCOX-2inhibitorsmightbeallowedover ashortperiodoftimefrompregnancyweek16to30,butitis preferabletoindicateprednisoneinlowdoses,whichmight beusedallacrosspregnancyandbreastfeedingwithnofetal risk.106
Hydroxychloroquine is an option for the treatment of chronicjointdisorders duringpregnancyand breastfeeding dueitsacknowledgedsafetyduringtheseperiods106,107 and
theevidenceindicatingimprovementofjointdisordersina caseseriesfromtheoverallpopulation.108,109
Asteroidsparingagent,azathioprine,mightbeused dur-ingpregnancyandbreastfeeding,whilemethotrexate(MTX) shouldbeavoidedbythetimeofconception,pregnancyand breastfeeding.106 Inadditiontoparacetamol,ibuprofenand
opioidsmightalsobeindicatedinselectcases.110
B.3.Relativetotheelderly(>60yearsold)withChikungunya fever,strictclinicalmonitoringofmedications,comorbidities andhigherriskofcomplicationsisrecommendedinallthe stagesofdisease,acuteonesinparticular.Concordance:9.61 (SD±0.737);levelofevidence(3,4)
Consideringelderlyindividualsasthoseaged60yearsand older,fewstudieshaveapproachedthis specific subpopula-tion.However,withacutoffpointof40yearsold,olderpatients exhibitedhigheroddsofprogressionintothechronicstage, asfoundintheLaVirginia,Colombiacohort,wherethe fre-quencywas52%,38andtheReunionIslandcohort,inwhich
70%ofthepatientsabove45exhibitedpersistentjointpain15 monthsafteracuteinfection(oddsratio(OR)4.2(CI1.9–9.3)).39
InastudyconductedinIndiawith509patients,the inten-sityoftheacutestageofdiseasewashigheramongtheelderly (above65yearsold)whowereconfinedtobedonaveragefor 4–6days;42%ofthemattainedfullrecoveryafter4weeks,and
nodeathsoccurred.19Theparticularitiesofdiseaseamongthe
elderlyarenotclearintheremainderoftheanalyzedcohorts; someofthemreportedahighernumberofmedicalvisits com-paredtoothergroupsofpatients.
Thefactorstobetakenintoaccountintheapproachand treatmentoftheelderlyarepolypharmacyandthepresence ofcomorbidities(arterialhypertension–AH–andDM),which are frequentin thisage range. Concomitant use ofseveral medicationsmightresultincomplicationsderivedfromthe interactionoftheanalgesicsandsteroidsindicatedforpain andarthritis.Manyelderlyuseaspirinprophylactically,which isassociatedwithReye’ssyndrome,buttherearenoreports amongpatientswithChikungunyafever.Decompensationof DMisassociatedwithdehydration,whichmightbea compli-cationincaseswithacuteinfection(6).
InBrazil,uptoEW27of2016,38deathsbyChikungunya feverwereconfirmed,correspondingtothefollowingstates: Pernambuco(n=25),RioGrandedoNorte(n=5),Paraíba(n=2), RiodeJaneiro(n=2),Ceará(n=2),Maranhão(n=1)andAlagoas (n=1);themedianageofthedeceasedwas71years old.111
RelativetoPernambuco,i.e.,thestatewiththelargestnumber ofdeathsinthecountry,morerecentdata(EW 37)showed that7970of53,061notifiedcasescorrespondedtoindividuals above60yearsold,with53confirmeddeathsbyChikungunya fever.112
Althoughtheelderlydonotrepresentthegroupwiththe highestprevalenceofdisease,mostdeathsoccurredwithin thisagerange.Thisshowsthatthispopulationneeds partic-ularattentionduringtheacutestage,morespecifically,those wholivealoneandmighthavenoassistanceforfeedingand personalcare.Manyelderlyare confinedtobed forup to7 days,whichincreasestheriskofurinarytractinfectionand pneumonia.113
B.4.Childrenunder2yearsofageshouldreceivespecial attentionduetotheirhigherriskofsevereandatypical man-ifestations and involvementofthe central nervous system (CNS).Concordance:9.30(SD±1.179);levelofevidence(3,4)
Up to the present time, few observational studies have investigatedclinicalandlaboratorymanifestationsof infec-tionwithCHIKVamongchildren.Mostsuchstudiesdescribe moresevereformsofdiseasesoccurringinnewborninfants andemphasizethefactthattheclinicalpresentationmightbe differentinchildrencomparedtoadults.Therateof asymp-tomaticinfectionseemstobehigheramongchildren,varying amongthevariousreportsofoutbreaks(35–40%).46,114–120A
recentstudyanalyzedtheseroprevalenceamongchildrenon the occasionofthefirst CHIKVoutbreak inNicaragua.The resultsshoweddetectableantibodylevelsin6.1%ofchildren aged2–14yearsand13.1%inthoseabove15yearsofage.121
Relative to the acute stage of infection,the differences betweenchildrenandadultsconcerntheskin,hemorrhagic and neurological manifestations.117 Maculopapular
exan-themaoccursin35–50%ofadultsbutislessfrequentamong children,especiallythoseunder2yearsold,with hyperpig-mentationamorecommonfinding.Inaddition,infantsunder 6monthsold might exhibitextensive skinbullouslesions, affectingupto35%ofthebodysurface.122Hemorrhagic
Themainconcernrelativetothepediatricpopulationis theinvolvementofthe CNS.During theChikungunyafever outbreak in Reunion Island, 25% ofthe childrenexhibited neurologicalsymptoms. Among suchchildren, a high pro-portion(40–50%)exhibited severemanifestations,including statusepilepticus, complexseizures andencephalitis.123,124
Theneurologicalsymptomscanlastfromseveralmonthsto years.123
B.5.Newborninfantsfrommotherswithclinical manifes-tationssuggestiveofChikungunyafeverclosetolaborshould besubjectedtocloseobservationduringthefirst5daysoflife. Rationaluseofmedications shouldbeperformedforcases thatdevelopdisease;complex casesshould bemanaged at theintensivecareunit.Concordance:9.54(SD±0.838);levelof evidence(3,4)
PerinatalinfectionwasfirstdescribedintheReunionIsland outbreakin2005.125AlthoughintrauterineCHIKV
transmis-sionisextraordinarilyrareattheonsetofpregnancy,itsrate increasestoalmost50%whenmaternalviremiaoccurs1week beforebirth.126
ArecentLatinAmericanmulticentricstudyanalyzed169 newborn infants with symptomatic Chikungunya fever at 4large maternity hospitalsfrom 3countries whose moth-ershadCHIKVinfectionconfirmedbyPCR.Intheseinfants, the symptoms started around the fourth day of life, the most frequent ones being fever, irritability, hyperalgesia, diffuselimbswelling,meningoencephalitis,skinrashand bul-lousdermatitisandpetechiae.Laboratorytestingevidenced thrombocytopeniaandlymphopeniainmostcases. Compli-cationsincludedintracerebralhemorrhage,statusepilepticus andmultipleorganfailure.103
Themortalityrateishigh,forwhichreasonlong-term out-comesanddamagecouldnotbeassessedinstudies.Among survivors,half ofthe children exhibited reduced cognitive development by 2 years of age.99,105,126 These data clearly
showthatinfectionwithCHIKVamongchildrenisnotalways benign; rather, it might result in permanent sequelae and death.
B.6.Treatment fortheacutestageofChikungunyafever inchildrenconsistsofhydration,analgesicsandantipyretic agents;salicylatesshouldbeavoided.Forthechronicstage,we suggestfollowingtherecommendationsforadults,while tak-ingtheparticularitiesinherenttothisagerangeintoaccount. Concordance:9.48(SD±0.785);levelofevidence(3,4)
Norecommendations specific forthe management and treatment of infection with CHIKV among children were located.InmostcaseseriespublishedafteroutbreaksinAsia andtheAmericas,therecommendationsaresimilartothose foradults:intheacutestage,hyper-hydration,analgesicsand antipyretics,withavoidanceofsalicylatesandNSAIDsdueto theriskoftriggeringbleeding.Whenthejointsymptoms per-sist,therecommendationsdonotdifferfromthoseforadults whoprogresstothechronicstage,treatmentbeingbasedon theuseofNSAIDs,steroidsandMTX;however,thebenefitsfor thepediatricpopulationarestillunknown.
Themorespecificavailablerecommendationstarget new-borninfants,inwhichmorbidityandmortalityarecommon. Rational use ofmedications and adequate monitoring are recommended, which seem to have a direct relationship with improved clinical progression. Abuse of medications,
suchassalicylates, NSAIDs,steroidsand antibiotics,might contribute to worsening disease through development of bleeding,thrombocytopeniaandgastrointestinalsymptoms, leading to complications, including hydroelectrolytic disor-ders,dehydrationandkidneyfailure,whichmightindirectly triggerdeath.99–101,103
B.7.Werecommendpaying specialattentiontopatients with previous diagnosis of rheumatoid arthritis, spondy-loarthritis or systemic lupus erythematosus, as these conditionsmightbecomereactivatedorexacerbated. Concord-ance:9.42(SD±1.840);levelofevidence(3,4)
Infection with CHIKV among patients with previous rheumatologicdiseasesisnotwellcharacterizedinthe litera-ture.Inthepublishedcaseseriesandcohorts,thefrequency ofprevious musculoskeletaldisordersamongpatientswith Chikungunya fever variesfrom 6.9%to86%,20,23,26,41,127 the
highestprevalenceratesbeingfoundinstudiesconductedat specializedservices.
A history of rheumatologic disease was associated with persistence of joint symptoms after infection with CHIKV40,41,127 andgreaterdisability.128 Exacerbationofpain
complaintsinthepreviouslyaffectedsiteswasdescribedin patientswithchronicdiseases,suchasOA,tendinopathy, lum-barpainandcarpaltunnelsyndrome.23,29,74,127Sissokoetal.39
followedup147patientsalong15months;28%ofthesample hadapreviousdiagnosisofOA,whichbehavedasapredictor ofpersistenceofsymptoms(OR2.9(95%CI1.1–7.4;p=0.029)). The acute clinical manifestations of patients with pre-vious musculoskeletal pain tend to be similar to those of previously healthy patientswith Chikungunyafever; atypi-calorsevereacutemanifestationsarenotmorefrequent,not evenamongpatientsusingimmunosuppressantsor immuno-biological agents.129–132 Interestingly, patients are able to
distinguish the symptomsrelated toCHIKVinfection from thoseoftheunderlyingdiseasebecausetheformeraremore intenseoroccurinsitesdifferentthanthelatter.133
Javelleetal.29assessed18patientswithprevious
rheuma-tologicdiseaseamong159patientsfollowedupover6years. In 6 patientswith RA, 8with SpA,2 withSLE and 2with chronichepatitis,thejointsymptomsworsenedimmediately afterinfectionwithCHIKV,requiringchangesintreatmentor onsetofnewtreatmentsinhalfofthem.
Patients with SpA might exhibit exacerbation charac-terized by greater peripheral involvement (arthritis and/or enthesitis),20,29 andthosewithpsoriaticarthritisexperience
exacerbationoftheskinand/orjointdisease.20
Patients with previously controlled RA might exhibit exacerbation of the joint symptoms in the acute stage of Chikungunya fever, eventually with the typical manifesta-tions ofRAinvolving thejointsofthehands andfeet.19,129
However,assessmentofpatientswithpreviousrheumatic dis-easeinMartiniquedidnotdetectanycasesofpost-CHIKRA exacerbation, which suggeststhat previous treatmentwith disease-modifying antirheumatic drugs (DMARDs) and/or immunobiologicalagentsmighthaveaprotectiveeffect.72