REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
Consumption
of
fruits
and
vegetables
associated
with
other
risk
behaviors
among
adolescents
in
Northeast
Brazil
Fabiana
Medeiros
de
Almeida
Silva
a,∗,
Aldemir
Smith-Menezes
b,
Maria
de
Fátima
da
Silva
Duarte
caProgramadePós-Graduac¸ãoemEducac¸ãoFísica,UniversidadeFederaldeSergipe(UFS),Aracajú,SE,Brazil
bInstitutoFederaldeEducac¸ão,CiênciaeTecnologiadeSergipe,UniversidadeFederaldeSergipe(UFS),Aracajú,SE,Brazil cCentrodeEsportes,ProgramadePós-Graduac¸ãoemEducac¸ãoFísica,UniversidadeFederaldeSantaCatarina(UFSC),
Florianópolis,SC,Brazil
Received6June2015;accepted13September2015 Availableonline2January2016
KEYWORDS
Adolescent; Foodconsumption; Riskfactors
Abstract
Objective: Todeterminetheprevalenceofconsumptionoffruitsandvegetablesandidentify theassociationwithlowlevelofphysicalactivity,exposuretosedentarybehavior,consumption ofsoftdrinksandoverweight/obesityinadolescents.
Methods: Thisis across-sectionalschool-based study witha representativesample of3992 studentsaged14---19yearsfromthestateofSergipe,Brazil.Theoutcomewaslowconsumption offruitsandvegetables(<5servings/day).Independentvariableswere:levelofphysicalactivity, sedentarybehavior,consumptionofsoftdrinks,andoverweight/obesity.GlobalStudentHealth Surveyquestionnaireandbodymassandheightmeasurementswereused,aswellaschi-square testandcrudeandadjustedbinarylogisticregression.Thesignificanceleveladoptedwas5%.
Results: Theprevalenceofinadequateconsumptionoffruitsandvegetableswashigh---88.6% (95%CI=87.6---89.5).Higherlikelihoodoflowconsumptionoffruitsandvegetableswasverified amongboyswhowereexposedtosedentarybehavior(OR=1.63;95%CI=1.18---2.24),who con-sumedsoftdrinks(OR=3.04;95%CI=2.10---4.40),withinsufficientlyphysicalactivity(OR=1.98; 95%CI=1.43---2.73) andgirlswhoconsumedsoftdrinks(OR=1.88;95%CI=1.43---2.47)andthose withoverweight/obesity(OR=1.63;95%CI=1.19---2.23).
Conclusions: Thereisaneedofpublicpoliciesaimedatencouragingtheconsumptionofhealthy foodsamongadolescents.
©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](F.M.Silva). http://dx.doi.org/10.1016/j.rppede.2015.09.004
PALAVRAS-CHAVE
Adolescente; Consumode alimentos; Fatoresderisco
Consumodefrutasevegetaisassociadoaoutroscomportamentosderisco
emadolescentesnoNordestedoBrasil
Resumo
Objetivo: Determinaraprevalênciadoconsumodefrutasevegetaiseidentificaraassociac¸ão comobaixoníveldeatividadefísica,exposic¸ãoacomportamentossedentários,consumode refrigerantesesobrepeso/obesidadeemadolescentes.
Métodos: Esteéum estudotransversaldebaseescolarcomumaamostrarepresentativade 3992alunoscomidadesentre14e19anosdoestadodeSergipe,Brasil.Odesfechofoiobaixo consumo defrutas e vegetais(<5 porc¸ões/dia). Asvariáveisindependentesforam: nível de atividadefísica,comportamentosedentário,consumoderefrigerantes,esobrepeso/obesidade. ForamusadosoquestionárioGlobalStudentHealthSurvey eopeso corporalealtura,bem comootestedoqui-quadradoeregressãologísticabinária(análiseajustadaebruta).Onível designificânciaadotadofoide5%.
Resultados: A prevalência de consumo inadequado de frutas e hortalic¸as foi alta --- 88,6% (IC95%=87,6-89,5). Verificou-se maiorprobabilidade debaixo consumo de frutas elegumes emmeninosqueestavamexpostosacomportamentosedentário(OR=1,63;IC95%=1,18-2,24), que consumiam refrigerantes (OR=3,04;IC95%=2,10-4,40), com atividade física insuficiente (OR=1,98;IC95%=1,43-2,73) e meninasque consumiam refrigerantes (OR=1,88, IC95%=1,43-2,47)eaquelascomsobrepeso/obesidade(OR=1,63,IC95%=1,19-2,23).
Conclusões: Háanecessidadedepolíticaspúblicasdestinadasaincentivaroconsumode ali-mentossaudáveisentreosadolescentes.
©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpenAccesssobumalicenc¸aCCBY(http://creativecommons.org/licenses/by/4.0/).
Introduction
Inthe lastdecade, encouragingincreasedconsumption of fruitsandvegetableshasbecomeapublichealthpriorityin manycountriesasaprotectiveeffectontheriskofobesity,1
typeIIdiabetesmellitus,2cardiovasculardiseases3andsome
typesofcancer.4 EstimatesfromtheWorldHealth
Organi-zation(WHO)showthat2.7milliondeathsaroundtheworld registeredin2000couldhavebeenavoidedwithadequate consumptionoffruits,legumesandvegetables,reducingby 1.8%theglobalburdenofdiseases.5
However,inBrazil,this consumptionis belowthat rec-ommendedbyWHO,whichadvocatesthedailyconsumption ofatleast400goffruitsandvegetables,equivalenttofive servings.6OnresearchconductedbyVIGITELtelephone
sur-veyinBraziliancapitalsin2010,thefrequencyofadultswho consumetherecommendedamountrangedfrom11.3%inRio Branco(Acre,NorthRegion)to24.8%inFlorianópolis(Santa Catarina,SouthRegion).Thelowestfrequencies,inmales, haveoccurredinRioBranco(Acre,10.0%),Macapá(Amapá, 10.6%) and Aracaju (Sergipe, 11.2%); and, in females, in Rio Branco (Acre, 12.5%), Manaus (Amazonas, 14.9%) and Macapá(Amapá,15.3%).7
Although non-communicable chronic diseases (NCDs) manifest more frequently in adulthood, the identification of health risk behaviors has been widely documented in literature, focusing on young individuals.8 Inappropriate
eating habits, smoking, alcohol consumption, insufficient levels of physical activity, obesity and excessive time in sedentaryleisureactivities aresomeofthemostcommon behaviorsduringadolescence.9Adolescentsshowexcessive
consumption of soft drinks, sugars and snacks like ‘‘fast
foods’’withhighfatcontents(especiallysaturatedfat)and lowintakeoffiberandpotassium.10
Giventheaboveandconsideringtheadequate consump-tionoffruitsandvegetablesasachallengetopublichealth policiesinthepreventionofdiseases,theaimofthisstudy was to determine the prevalence of low consumption of fruitsandvegetablesamongadolescentsfrompublicschools in thestate Sergipe and itsassociation withlowlevels of physicalactivity,exposuretosedentarybehavior, consump-tionofsoftdrinksandoverweight/obesity.
Method
This study is a secondary analysis of data of an epidemi-ologicalcross-sectionalsurveyentitled‘‘LivingandHealth ConductsofAdolescentsResidentsinRuralandUrbanAreas intheStateofSergipe,Brazil’’,developedin 2011bythe Research Group in Physical Education and Health of the Federal Institute of Education, ScienceandTechnology of Sergipe (GPEFiS/IFS). This project was approved by the EthicsCommitteeonHumanResearchoftheUniversity Hos-pitaloftheFederalUniversity ofSergipe(CEP/UFS)under protocolnumberCAAE---2006.0.000.107-10.
AccordingtoinformationfromtheBrazilianInstituteof Geography and Statistics,11 in 2011, the state of Sergipe,
northeasternBrazil,hasanareaof21,910.348km2,atotal
population of 2,068,031 people, including 233,119 ado-lescents (13---19 years). The state has 75 municipalities geographicallydividedintoeightterritories.
nightshiftsoftheStateeducationsystem.Consideringdata available on the State Secretariat of Educational (2010), highschoolenrollment,in2010,waspresentfor58,301 stu-dents throughout Public StateSchools, distributed in 155 teachingunits.To composethe researchsample, teaching units wererandomly selectedby thenumber of students, distributedinmunicipalitiesofeachterritory.Then,classes wererandomlyselected(considering25students/class),by gradeandshift.Thecalculationoftheresearchsampleused complex sampling process available in the SPSS software (version 15.0). The sample size estimation in the analy-sisofprevalence for eachterritory considered thesizeof theterritory population,the estimatedprevalence of50% as the highest expected, confidence interval of 95% and tolerablesampling error of 5%.The sample sizewas mul-tiplied by 1.5 due tothe correction of the design effect (deff=1.5),estimating theneed ofstudents forevery
ter-ritory.Inordertoavoidlosingsamplingrepresentativeness, an incrementof 20% of students wereadded due reasons such asrefusals, age out of the range established in this study,failingtorespondtoimportantissuessuchassexand age,amongothers.Theassociationanalysisconsideredalso astatisticalpowerof80%andOddsRatio(OR)of1.2, requir-inga minimum sample of 3875adolescents for theentire state.
Sampleselectionusedthestratifiedsamplingprocessby conglomeratesintwostages:(1)stratifiedsamplingprocess proportionaltotheterritoryandschoolsize(1=upto199
stu-dents;2=200---499students;3=500studentsormore).Thus,
considering thethreeschoolsizes,it wasestablishedasa criterion the random selection of 25% of state education units (155 teaching units), totaling 39 schools distributed in27municipalities;(2)classeswereselectedaccordingto grade and school shift, by using the simple random pro-cess considering 25 students per class. The participation ofadolescentsinthestudywasvoluntaryandanonymous, adopting,inadditiontotheParentalpassiveconsentform, thefollowinginclusioncriteria:beingregularlyenrolledin classes from 1st to 3rd grades of selected high schools; beingpresent onthe day of instrumentapplication; com-plete questionnaire response; and age of 14---19 years. School principals also signed the Free and Clarified Con-sentFormauthorizingtheparticipationofinstitutionsinthe research.
Datacollectionwasdonebyphysicaleducationteachers trained in the following aspects: domain of the instru-ment’s questions, form of implementation, monitoring, analysisof questionnairesafter application and anthropo-metricmeasurements. The questionnaire wasappliedand theanthropometricmeasurementsweretaken(bodymass andheight)attheclassroom,withtwoteachersperclass, so that theycould answer doubts andassist in filling out questionnaires.Theaveragetimeapplyingthequestionnaire was45min.TheinstrumentusedwasaversionoftheGlobal School---basedStudentHealthSurvey,proposedbytheWorld HealthOrganization(GSHS/WHO).
Sixhealth-relatedbehaviorswereanalyzed:levelof reg-ularphysicalactivity,sedentarybehavior,andconsumption of alcohol, cigarettes, soft drinks, fruits and vegetables. Adolescents who did not practice at least 300min of moderate or vigorous physical activity per week (taking into account physical education classes, displacements,
sports practice or other physical activities during leisure time)12 were considered insufficiently active. Adolescents
exposed to screen (television and media) for more than twohoursper day were considered asexposed to seden-tarybehavior;13 consumptionofcigarettesandalcoholwas
considered for those who reported any consumption in the last 30 days; consumption of soft drinks was consid-eredifconsumptionwasreportedonceor moretimesper day;overweight/obesitywasdefinedbyabodymassindex (BMI) --- for-age14 of >25kg/m2. For the consumption of
fruitsandvegetables,thedependentvariableofthisstudy, two or more servings of fruits and three or more serv-ingsof vegetablesperday wereconsidered asadequate.6
Inthe case offruits, only theconsumption of fresh fruits was considered, in other words, fruit juices were not calculated.
TheIntelligentCharacterRecognition-Teleformsoftware (HSInformática,RiodeJaneiro,Brazil)andtheFI-6230 scan-ner (Fujitsu, Tokyo, Japan) were used to accomplish the tabulationof data,using opticalreader. Afterthis phase, theauthorsmanuallycheckedandcorrectederrorson ques-tionnairesthatshowedproblems.
DataanalysiswasperformedusingtheStatisticalPackage for Social Science for Windows software (SPSS, version 20.0).Variableswereanalyzedusingdescriptiveand infer-ential procedures. In the bivariate association analysis, thechi-squaretest for heterogeneity andfor lineartrend was used. In the multivariable analysis, crude binary logistic regression for the study outcome was used (con-sumption of fruits and vegetables), being adjusted for age and skin color. The significance level adopted was
p≤5%.
Results
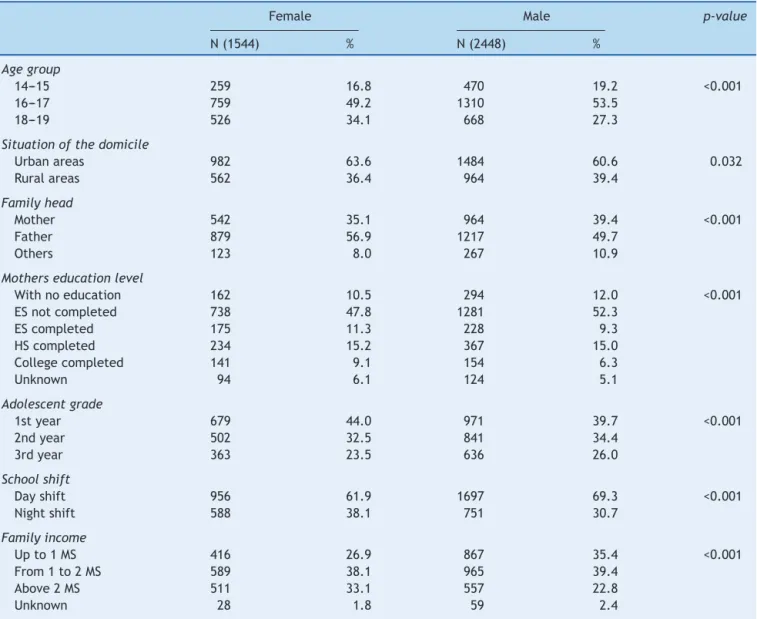
Dataof 4717 students wereanalyzed; however, 725 were excludedforthelackofimportantvariablessuchasageand sex,andalsothoseagedover19years.Thefinalsample com-prised3992children (61.3%femaleand38.7%male), aged 14---19years(51.8%with16---17yearsold).Table1showsthe demographiccharacteristics andsocioeconomicconditions ofindividualsparticipatinginthestudy.
Moststudentsreportedlivinginurbanareas(61.8%).For 52.5%thefatherwasthefamilyhead,in50.6%motherhad incompleteelementaryschool,41.3%ofthestudentswere enrolledinthefirstyearofhighschool,and66.5%intheday shift(66.5%).Moststudentshadfamilyincomesuptotwo minimumwages.
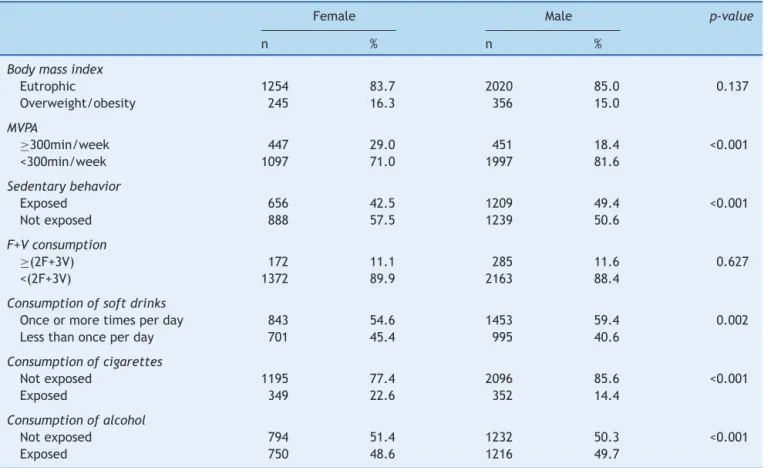
InrelationtohealthriskbehaviorsshowninTable2,the followingprevalence’swerefound:(a)studentswith insuffi-cientlevelsofphysicalactivity−77.5%(95%CI=76.2---78.8);
(b) students exposed to sedentary behavior − 46.7%
(95%CI=45.2---48.3);(c)studentsthat didnotmeet recom-mendationsfor the consumption of fruits and vegetables
− 88.6% (95%CI=87.6---89.5); (d) students with excessive
soft drinks intake − 57.5% (95%CI=56.0---59.0); (e)
stu-dentswithoverweight/obesity− 15.5%(95%CI=14.4---16.7);
(f) students who reported alcohol intake in the last 30 days − 49.2% (95%CI=47.7---50.8); and (g) students
who reported smoking in the last 30days − 17.6%
Table1 Sociodemographiccharacteristicsofthestudents(n=3992)accordingtosex.
Female Male p-value
N(1544) % N(2448) %
Agegroup
14---15 259 16.8 470 19.2 <0.001 16---17 759 49.2 1310 53.5
18---19 526 34.1 668 27.3
Situationofthedomicile
Urbanareas 982 63.6 1484 60.6 0.032 Ruralareas 562 36.4 964 39.4
Familyhead
Mother 542 35.1 964 39.4 <0.001 Father 879 56.9 1217 49.7
Others 123 8.0 267 10.9
Motherseducationlevel
Withnoeducation 162 10.5 294 12.0 <0.001 ESnotcompleted 738 47.8 1281 52.3
EScompleted 175 11.3 228 9.3 HScompleted 234 15.2 367 15.0 Collegecompleted 141 9.1 154 6.3
Unknown 94 6.1 124 5.1
Adolescentgrade
1styear 679 44.0 971 39.7 <0.001 2ndyear 502 32.5 841 34.4
3rdyear 363 23.5 636 26.0
Schoolshift
Dayshift 956 61.9 1697 69.3 <0.001 Nightshift 588 38.1 751 30.7
Familyincome
Upto1MS 416 26.9 867 35.4 <0.001 From1to2MS 589 38.1 965 39.4
Above2MS 511 33.1 557 22.8
Unknown 28 1.8 59 2.4
ES,elementaryschool;HS,highschool;MS,minimumsalary.
Table 3 shows the crude adjusted association between consumption of fruits and vegetables and other health risk behaviors in malestudents fromSergipe. Inadequate consumption of fruits and vegetables was associated to exposuretosedentarybehavior,consumptionofsoftdrinks andlowlevelofphysicalactivity.Adolescentswhoare expo-sure to sedentary behavior (OR=1.63; 95%CI=1.18---2.24),
who consume soft drinks once or more times a day (OR=3.04; 95%CI=2.10---4.40) and who are insufficiently
active (OR=1.98; 95%CI=1.43---2.73) were more likely to
presentlowconsumptionoffruitsandvegetables.
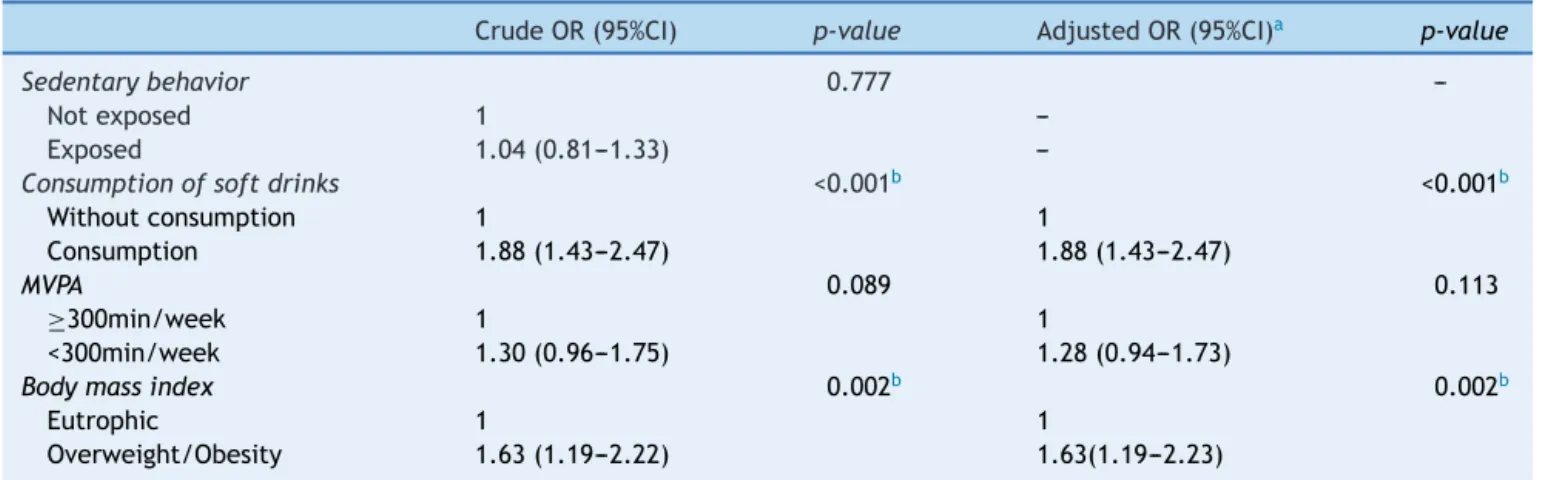
Table 4 shows the crude adjusted association between consumption of fruits and vegetables and other health riskbehaviorsinfemalestudentsfromSergipe.Inadequate consumption of fruits and vegetables was associated to consumptionofsoftdrinksandoverweight/obesity. Adoles-centswhoconsumesoftdrinksonceormoretimesperday (OR=1.88,95%CI=1.43---2.47)andwhoareoverweight/obese
(OR=1.63, 95%CI=1.19---2.23) were more likely to present
lowconsumptionoffruitsandvegetables.
Discussion
Inthisstudy,therewasahighprevalenceofinadequate con-sumptionoffruitsandvegetablesamongadolescentsfrom Sergipe.Only11.4%ofyoungpeoplemetrecommendations of dailyconsumption of thesefoods. This resultis consis-tent with previous studies in other countries, which also revealed inadequateconsumptionof fruitsandvegetables amongadolescents.AstudyconductedinEurope15revealed
that adolescents consumehalf the recommendedamount of fruits and vegetables.Likewise, research conducted in China16 verifiedthat only 9% and 14% of adolescents met
theminimumdailyrecommendedvaluesofvegetablesand fruits,respectively.
Investigationsontheconsumptionoffruits and vegeta-bles in Brazil have shown that only 15% of students in the city of Florianópolis (SC),17 6.5% in the city of
Caru-aru (PE),18 5.3% in the city of Pelotas (RS)19 and 2.7% in
the state of Santa Catarina20 consume the recommended
Table2 Characteristicsofhealthriskbehaviorsofthesample(n=3992)accordingtosex.
Female Male p-value
n % n %
Bodymassindex
Eutrophic 1254 83.7 2020 85.0 0.137 Overweight/obesity 245 16.3 356 15.0
MVPA
≥300min/week 447 29.0 451 18.4 <0.001
<300min/week 1097 71.0 1997 81.6
Sedentarybehavior
Exposed 656 42.5 1209 49.4 <0.001 Notexposed 888 57.5 1239 50.6
F+Vconsumption
≥(2F+3V) 172 11.1 285 11.6 0.627
<(2F+3V) 1372 89.9 2163 88.4
Consumptionofsoftdrinks
Onceormoretimesperday 843 54.6 1453 59.4 0.002 Lessthanonceperday 701 45.4 995 40.6
Consumptionofcigarettes
Notexposed 1195 77.4 2096 85.6 <0.001 Exposed 349 22.6 352 14.4
Consumptionofalcohol
Notexposed 794 51.4 1232 50.3 <0.001 Exposed 750 48.6 1216 49.7
MVPA,moderateandvigorousphysicalactivity;F,fruits;V,vegetables.
Table3 Binarylogisticregressiontoestimatetheassociationofinadequateoffruitsandvegetablesconsumptionandother healthriskbehaviorsamongboys.
CrudeOR(95%CI) p-value AdjustedOR(95%CI)a p-value
Sedentarybehavior 0.004b 0.003b
Notexposed 1 1
Exposed 1.61(1.17---2.21) 1.63(1.18---2.24)
Consumptionofsoftdrinks <0.001b <0.001b
Withoutconsumption 1 1
Consumption 3.07(2.12---4.44) 3.04(2.10---4.40)
MVPA <0.001b <0.001b
≥300min/week 1 1
<300min/week 1.97(1.42---2.72) 1.98(1.43---2.73)
Bodymassindex 0.919
---Eutrophic 1
---Overweight/Obesity 0.98(0.63---1.51)
---OR,OddsRatio;CI,confidenceinterval;MVPA,moderateandvigorousphysicalactivity.
a Adjustedforageandskincolor.
b p≤0.05,TestedeWald.
ofthreeadolescentsdoesnotconsumeorconsumesfruits andvegetablesatleastonceperdayand62.9%ofthemare dailyexposedtoexcessiveconsumptionofsoftdrinks.The National AdolescentSchool-based HealthSurvey(PeNSE)22
pointedoutthat21%ofstudentsdonotconsumefruitsand 26.8%donoteatvegetablesinanydayoftheweek.
Furthermore,therewasapositive associationbetween consumptionoffruitsandvegetablesandvariablesrelated to other health risk behaviors. The results revealed that
Table4 Binarylogisticregressiontoestimatetheassociationofinadequateoffruitsandvegetablesconsumptionandother healthriskbehaviorsamonggirls.
CrudeOR(95%CI) p-value AdjustedOR(95%CI)a p-value
Sedentarybehavior 0.777
---Notexposed 1
---Exposed 1.04(0.81---1.33)
---Consumptionofsoftdrinks <0.001b <0.001b
Withoutconsumption 1 1
Consumption 1.88(1.43---2.47) 1.88(1.43---2.47)
MVPA 0.089 0.113
≥300min/week 1 1
<300min/week 1.30(0.96---1.75) 1.28(0.94---1.73)
Bodymassindex 0.002b 0.002b
Eutrophic 1 1
Overweight/Obesity 1.63(1.19---2.22) 1.63(1.19---2.23)
OR,OddsRatio;CI,confidenceinterval;MVPA,moderateandvigorousphysicalactivity.
aAdjustedforageandskincolor.
b p≤0.05,TestedeWald.
Inadequate consumption of fruits and vegetables was relatedtothehabitofconsumingsoftdrinks.Recentstudies haveshownthatfoodsrichinsugarsareinverselyrelatedto theconsumption of fruitsand vegetables.23,24 This finding
corroboratesresults found in the lastBrazilian Household BudgetSurvey---BrazilianPOF,25whichindicated
consump-tionoffruitsandvegetablesfarbelowrecommendationsand high consumption of beverageswith addedsugar, such as juicesandsoftdrinks.
Therelationshipbetweenconsumptionoffruitsand veg-etablesandexposuretosedentarybehaviorfoundinmales studentswassimilartootherstudiessuchasthatconducted withadolescentsin Denmark,26 which verified association
between unhealthy eating preferences and longer time spentwatchingtelevision.InAustrália,27theauthorsfound
significantassociationbetweenTVtimeequaltoorgreater thantwohours(≥2h/day) andconsumption of softdrinks
andsaltysnacks,andaninverseassociationbetweenTVtime (≤2h/day)andconsumptionoffruitsandvegetables.
Lowconsumption of fruitsand vegetablesis relatedto lowlevelofphysicalactivityamongmaleadolescents. Stud-iesconductedwithadultsinFlorianópolis(SC)28alsoshowed
moreadequateconsumptionoffruitsandvegetablesamong those who practiced physical activity during leisure time comparedtothoseinactiveduringleisuretime.Similarly,a studyconductedwithadultsinFrance29revealedaninverse
association betweenconsumption of fruitsand vegetables and unhealthy lifestyle behavior, especially low level of physicalactivity.
Lowconsumption offruitsandvegetablesshowed rela-tionshipwithoverweightandobesity inwomen. Similarly, inNorth-American30 adults,it wasfoundthat obesity was
associatedwithinadequateconsumptionoffruitsand veg-etables.Astudy conductedwithadultsfromFlorianópolis (SC)28 showedthatnormalweightmenweremorelikelyto
haveadequateconsumption offruitsandvegetableswhen comparedtotheiroverweightpeers.
Promotingan increaseintheconsumption offruitsand vegetablesamongadolescentsisagreatchallengetopublic health, because it is associated withdifferent behavioral
factors, as well as with socioeconomic and demographic issues.However,itisnecessarytobeawarethat consump-tion belowrecommendations can damage thegrowth and development potentialof adolescents,aswell asbeing a health riskfactor.Accordingtotheguidelinesdesignedto contribute to theprevention of diseases caused by nutri-tional deficiencies for the Brazilian population over two years of age,6 fruits and vegetables area group of foods
richinvitamins,mineralsandfibers,whichshouldbeindaily meals.Accordingly,increasingtheproductionandsupplyof affordableandhigh-qualityfoodtothepopulation, ensur-ingthesupply offreshandnutritious foodsin schoolsand includingfeeding and nutritiontopics asa cross-sectional component in the elementary and high school curriculum aresomestrategiesthat canbedevelopedbythe govern-mentandbythefoodproductivesectorinordertopromote healthamongadolescents.
This studypresents some limitations which need tobe considered such as: (a) the use of a questionnaire may increase theincidenceofbiases,(b)thegeneralization of dataforalladolescentsinSergipeduetothefactthatthe studywasrestrictedtoschoolbelongingtothestate educa-tionalsystemand(c)thepossibilityofreversecausalitydue tothestudydesign.
The findings ofthis study show that the prevalence of consumption of fruits and vegetables among adolescents frompublicschoolsofSergipeisbelowcurrent recommen-dations.Fromtheperspectiveofpublichealth,thefactors associatedwithlowconsumptionofthesefoodsmay subsi-dizehealthpromotionprogramsintheschoolenvironment, alsotakingintoaccountthedifferencesbetweensexes.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
References
1.HeoM,KimRS,Wylie-RosettJ,AlissonDB,HeymsfieldSB,Faith MS.Inverseassociationbetweenfruitandvegetableintakeand BMIevenaftercontrollingfordemographic,socioeconomicand lifestylefactors.ObesFacts.2011;4:449---55.
2.LiM,FanY,ZhangX,HouW,TangZ.Fruitandvegetableintake andriskoftype2diabetesmellitus:meta-analysisof prospec-tivecohortstudies.BMJOpen.2014;4:e005497.
3.WoodsideJV,YoungIS,McKinleyMC.Fruitandvegetableintake and risk of cardiovascular disease. Proc Nutr Soc. 2013;72: 399---406.
4.OyebodeO,Gordon-DseaguV,WalkerA,MindellJJ.Fruitand vegetableconsumptionandall-cause,cancerandCVD mortal-ity: analysisofHealth Surveyfor Englanddata. J Epidemiol CommunityHealth.2014;68:856---62.
5.World Health Organization. Fruit and vegetable promotion initiative-reportofthemeeting.Geneva:WHO;2003.
6.Brasil---MinistériodaSaúde.SecretariadeAtenc¸ãoàSaúde ---coordenac¸ão-geraldapolíticadealimentac¸ãoenutric¸ão.Guia alimentarparapopulac¸ãobrasileira:promovendoaalimentac¸ão saudável.Brasília:MinistériodaSaúde;2008.
7.Brasil---MinistériodaSaúde.SecretariadeVigilânciaemSaúde. VigitelBrasil2011:Vigilânciadefatoresderiscoeprotec¸ãopara doenc¸ascrônicasporinquéritotelefônico.Brasília:Ministério daSaúde;2012.
8.FariasJúniorJC,NahasMV,BarrosMV,LochMR,OliveiraES,De BemMF,etal.Comportamentosderisco àsaúdeem adoles-centesnoSuldoBrasil:prevalênciaefatoresassociados.Rev PanamSaludPublica.2009;25:344---52.
9.FariasJúniorJC,MendesJK,BarbosaDB,LopesAS. Cardiovascu-larriskfactorsforadolescents:prevalenceandassociationwith sociodemographicfactors.RevBrasEpidemiol.2011;14:50---62.
10.WendpapLL,FerreiraMG,RodriguesPR,PereiraRA,Loureiro AdaS,SilvaRM.Adolescents’dietqualityandassociated fac-tors.CadSaudePublica.2014;30:97---106.
11.Instituto Brasileiro de Geografia e Estatística[homepage on
theInternet].PesquisasobredadosdemográficosdoEstadode
Sergipe;2008.Availablefrom:http://www.ibge.gov.br
12.WorldHealthOrganization.Globalrecommendationson physi-calactivityforhealth.Geneva;2010.
13.AmericanAcademy ofPediatrics.Policy statement:children, adolescentes and television (RE0043). Pediatrics. 2001;107: 423---6.
14.Cole TJ, Bellizze MC, Flegal KM, Dietz WH. Establishing a standarddefinitionforchildoverweightandobesityworldwide: internationalsurvey.BMJ.2000;320:1---6.
15.DiethelmK,JankovicN,MorenoLA,HuybrechtsI,DeHenauwS, DeVriendtT,etal.FoodintakeofEuropeanadolescentsinthe lightofdifferentfood-baseddietaryguidelines:resultsofthe HELENA(HealthLifestyleinEuropebyNutritioninAdolescence) Study.PublicHealthNutr.2012;15:386---98.
16.ZhangCX,ChenYM,ChenWQ,SuYX,WangCL,WuJN.Food groupintakeamongadolescentsinGuangzhoucitycompared
with the Chinese dietary guidelines. Asia Pac J Clin Nutr. 2012;21:450---6.
17.Assis MA, Calvo MC, Kupek E, Vasconcelos FA, Campos VC, MachadoM,etal.Qualitativeanalysisofthedietofa probabilis-ticsampleofschoolchildrenfromFlorianopolis,SantaCatarina State,Brazil,usingthepreviousdayfoodquestionnaire.Cad SaudePublica.2010;26:1355---65.
18.MunizLC,ZaniniRV,SchneiderBC,TassitanoRM,FeitosaWM, Gonzalez-ChicaDA.Prevalenceandfactorsassociatedwiththe consumptionoffruitand vegetablesbyadolescentsinpublic schools inCaruaru,Pernambucostate.CiencSaudeColetiva. 2013;18:393---404.
19.NeutzlingMB,Assunc¸ãoMC,MalconMC,HallalPC,MenezesAM. Foodhabits ofadolescent studentsfrom Pelotas,Brazil.Rev Nutr.2010;23:379---88.
20.Costa LC,Vasconcelos FA, Corso AC.Factorsassociated with adequate fruit and vegetable intake by schoolchildren in Santa Catarina State, Brazil. Cad Saude Publica. 2012;28: 1133---42.
21.XavierIC,HardmanCM,AndradeML,BarrosMV.Frequencyof consumptionoffruits,vegetablesandsoftdrinks:a compara-tivestudyamongadolescentsinurbanandruralareas.RevBras Epidemiol.2014;17:371---80.
22.InstitutoBrasileirodeGeografiaeEstatística.PesquisaNacional deSaúdedoEscolar.RiodeJaneiro:IBGE;2009.
23.FigueiredoIC,JaimePC,MonteiroCA.Factorsassociatedwith fruitandvegetableintakeamongadultsofthecityofSãoPaulo, SoutheasternBrazil.RevSaudePublica.2008;42:777---85. 24.Levy-CostaRB,SichieriR,PontesNS,MonteiroCA.Household
foodavailabilityinBrazil:distributionandtrends(1974---2003). RevSaudePublica.2005;39:530---40.
25.Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orc¸amentos Familiares 2008---2009: antropometria e estado nutricionaldecrianc¸as,adolescenteseadultosnoBrasil.Rio deJaneiro:IBGE;2010.
26.Hare-BruunH, NielsenBM,KristensenPL, MøllerNC, TogoP, HeitmannBL.Television viewing,foodpreferences,andfood habits among children: a prospective epidemiological study. BMCPublicHealth.2011;11:311.
27.SalmonJ,CampbellKJ,CrawfordDA.Televisionviewinghabits associated with obesity risk factors: a survey of Melbourne schoolchildren.MedJAust.2006;184:64---7.
28.CamposVC,BastosJL,GaucheH,BoingAF,AssisMA.Factors associatedtotheadequateconsumptionoffruitsand vegeta-bles in adults from Florianopolis, Southern Brazil. Rev Bras Epidemiol.2010;13:352---62.
29.Oppert JM, ThomasF, Charles MA, Benetos A, Basdevant A, SimonC.Leisure-timeandoccupationalphysicalactivityin rela-tiontocardiovascularriskfactorsandeatinghabitsinFrench adults.PublicHealthNutr.2006;9:746---54.