Arq. Bras. Cardiol. vol.82 número1 en a08v82n1
Texto
Imagem

Documentos relacionados
Atrial fibrillation and flutter are arrhythmias frequently observed in the first days following coronary artery bypass graft surgery.. Its incidence ranges from 17 to 33% 1-8
Regarding the multivariate analysis of the association between spontaneous echo contrast in the aorta and the presence of other risk factors for ischemic stroke, among the
Our study assessed the influen- ce of 2 single sessions of resistive (circuit weight training) and aerobic exercise training on changes in blood pressure and heart rate in a group
Comparison of methods of measure- ments of oxygen consumption in mechanically ventilated patients with multiple trauma: the Fick method versus indirect calorimetry. Flancbaun L,
Balloon valvuloplasty successfully used in severe mitral stenosis during pregnancy and in aortic stenoses in nonpregnant, but at high risk for aortic valve replacement 11,12 ,
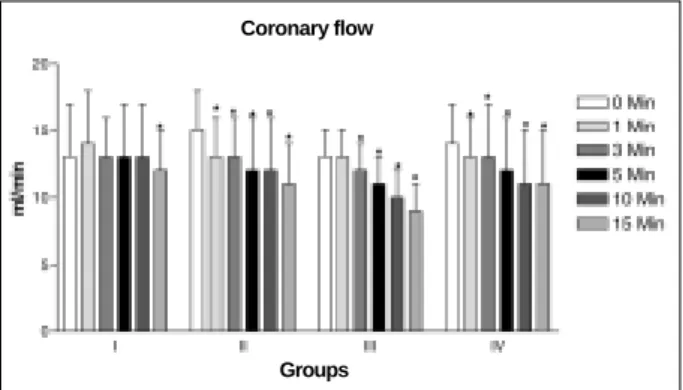
Figure 1 shows the percentage of change in contraction force, heart rate and coronary flow in isolated hearts perfused with normal Krebs-Ringer solution or normal Krebs- Ringer
In addition, during reperfusion no further decrease was observed in +dT/dt or -dT/dt in isolated rat hearts perfused with Ang-(1-7), indicating a ben- eficial effect
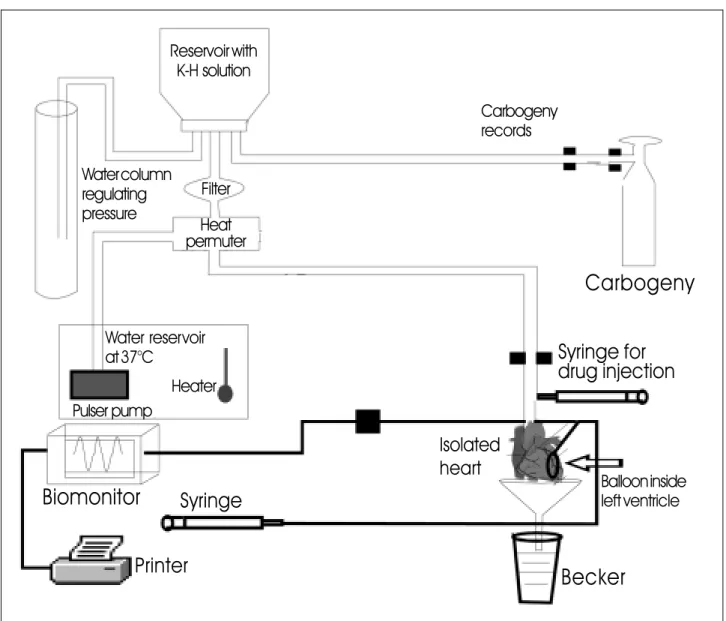
The objective of the present study was to analyze the performance of widely used con- tractility indexes in the isovolumetrically beating isolated heart, in two experimental models
