Arq. Bras. Cardiol. vol.82 número1 en a09v82n1
Texto
Imagem
Documentos relacionados
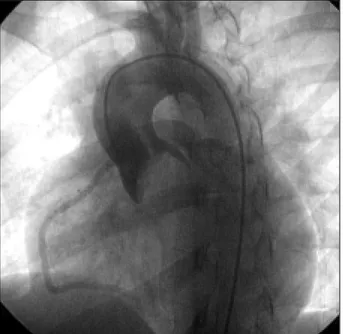
The transcatheter aortic valve implantation has become a therapeutic option for patients with symptomatic severe aortic stenosis and high risk for conventional valve
Implantation was performed after valvuloplasty with balloon catheter in patients with native valve stenosis and without valvuloplasty in patients with pre-existing bioprosthesis
Transcatheter aortic valve implantation for the treatment of severe symptomatic aortic stenosis in patients at very high or prohibitive surgical risk: acute and late outcomes of
operation of a hemophilic patient with mitral and aortic valve disease of rheumatic etiology undergoing aortic valve replacement and mitral comissurotomy; in this case a VIIIf
Transcatheter aortic valve implantation (TAVI) is a recent technique for the treatment of patients with severe symptomatic aortic stenosis (AS), who are at high risk for
The increase of cardiac output during pregnancy is the cause of heart failure in women with severe aortic valvular stenosis.. Percutaneous aortic valvuloplasty
Influence of mitral valve morphology on double-balloon catheter balloon valvuloplasty in patients with mitral stenosis: analysis of factors predicting immediate and 3-month
The percutaneous valve replacement, which is a reality in valvular diseases (especially aortic stenosis), is indicated for patients with high or prohibitive surgical risk..
