Arq. Bras. Cardiol. vol.73 número5
Texto
Imagem
Documentos relacionados
The first stage involves the creation of an ample connection between the systemic right ventricle through the pulmonary artery branch and the descending aorta and the
The inferior vena cava was sectioned from the right atrium and anastomosed to a cryopreserved descending aorta homograft tube [2], which was also anastomosed to the pulmonary
In the anomalous origin of the right coronary artery from left aortic sinus, with a route between the aorta and pulmonary trunk, surgical anastomosis of right internal thoracic
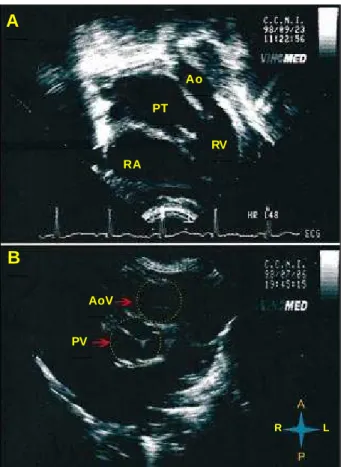
Fig.3 The Baseline aspect externally highlighting the communication (window) existing between the descending aorta e the pulmonary trunk Fig.2 Color flow mapping echocardiogram on
16 implanted between the aorta near the left subclavian artery and descending aorta below the compromised segment. Fig 2/Video
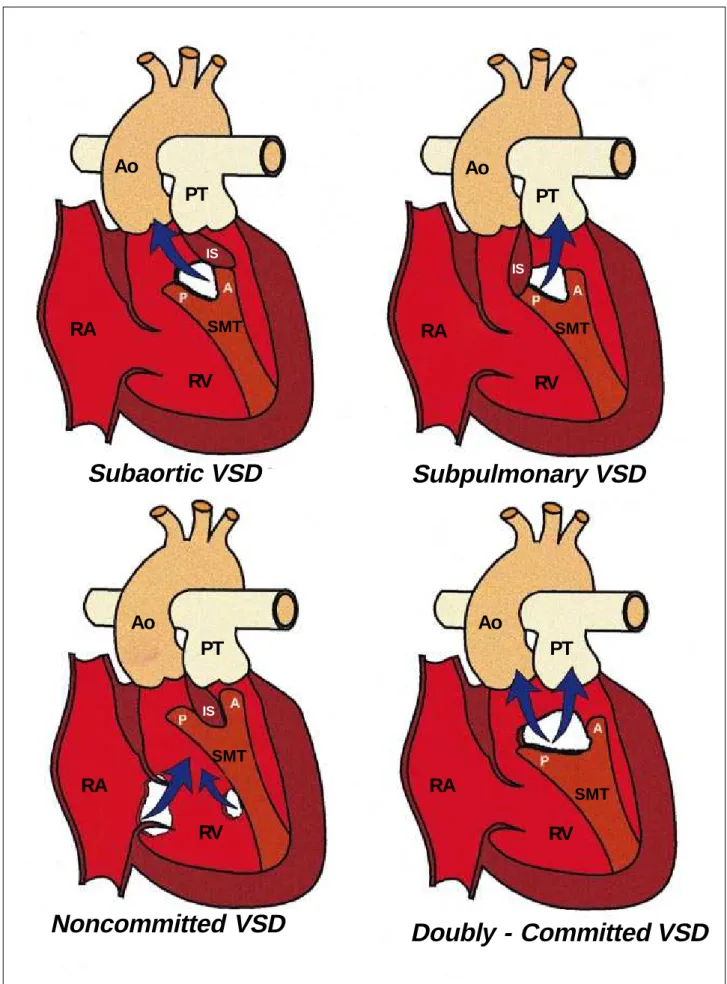
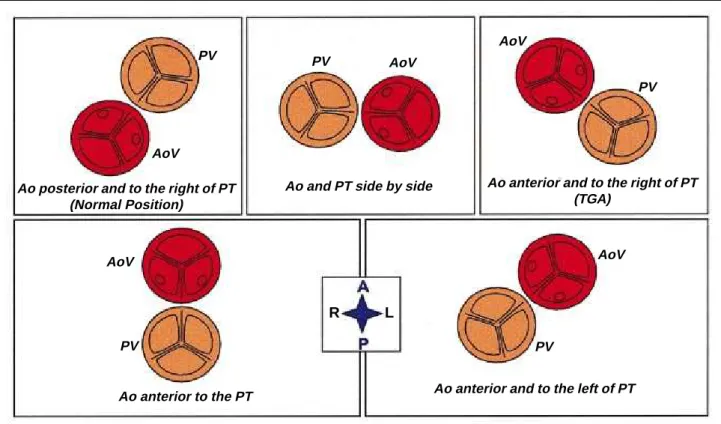
Since her childhood, the patient was diagnosed with double outlet right ventricle (DORV) with anterior aorta, severe pulmonary valve stenosis (PVS), hypoplasia of the pulmonary
D: right side of the patient; [E: left side of the patient, LA (AE): left atrium; MIP: maximum intensity projection; PV (VP): pulmonary veins, Ao: aorta, VPC: common pulmonary
The echocardiogram (Figure 2) showed a criss-cross heart with atrioventricular discordance and double-outlet right ventricle, arising from the right aorta and pulmonary artery
