THE STAT&3 OF POLIOMYELITIS IN VENEZUELA’ Eriberto Echezuria, M.D., M.P.H.2
Since 1971 Venezuela has been combating poliomyelitis by means of intense house-to-house vaccination campaigns. This article describes these campaigns and the results achieved thus far.
Introduction
Positive clinical identification of polio- myelitis in Venezuela was made in 1928; but it was not until 1960 that the National Institute of Hygiene in Caracas obtained laboratory confirmation of the disease with virologic and serologic tests. Starting in 196 1, however, these laboratory tests came to be performed with some regularity, and since 1965 they have been carried out in a routine and systematic fashion.
Reliable data on the frequency of poliomy- elitis cases in Venezuela dates from 1950 (300 to 400 cases registered yearly). and especially from 1965 (when the Division of Epidemiology of the Ministry of Health and Social Welfare organized its special Poliomyelitis Surveillance Unit). Since the latter date routine epidemi- ologic and clinical studies have been carried out on each suspected case; some 90 per cent of these cases have also been subjected to labora- tory testing; and many of the fatal cases have been given pathological examinations as well. This has permitted identification of nonpar- alytic poliomyelitis cases, as well as statistical elimination of infections due to other agents such as ECHO and Coxsackie viruses.
1 Also appearing in Spanish in Boletin de la Oficina Sanitaria Panamericana. Vol. LXXVl, 1974.
ZHead, Division of Demography and Epidemi- ology, Ministry of Health and Social Welfare, Caracas, Venezuela.
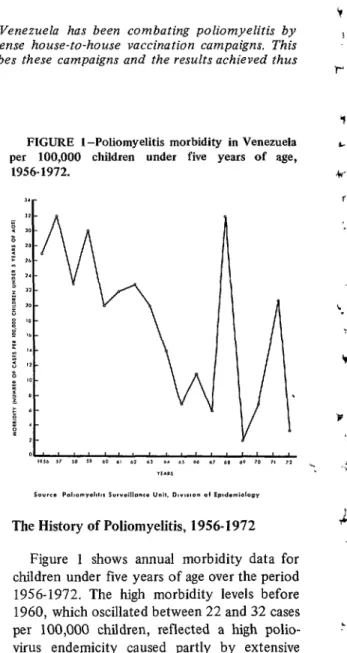
FIGURE l-Poliomyelitis morbidity in Venezuela per 100,000 children under five years of age,
1956-1972. ,a-
The History of Poliomyelitis, 19561972
Figure 1 shows annual morbidity data for children under five years of age over the period 1956-1972. The high morbidity levels before 1960, which oscillated between 22 and 32 cases per 100,000 children, reflected a high polio- .’ virus endemicity caused partly by extensive circulation of polioviruses in many tropical
areas where suboptimal sanitary conditions Y prevailed.
Echezuria . POLIOMYELITIS IN VENEZUELA 67
Vaccination with inactivated Salk poliovac- tine was carried out in the years 1957-1964, but not extensively enough to be an important factor in controlling the endemo-epidemic course of the disease. Then in October 1964 the country’s first National Mass Immunization Campaign was conducted with live attenuated Sabin oral vaccine; since that time eight similar campaigns have been carried out.
Because poliomyelitis in Venezuela is limited almost entirely to children under five, the mass campaigns of 1964-1969 were aimed at that age group; since 1970 the campaigns have been restricted to children less than three years old. During the period 19651967 the poliomy- elitis attack rate was considerably lower than in preceding years, the morbidity levels averaging around half of the average level experienced in the early 1960’s. However, an epidemic broke out in 1968 (involving 568 confirmed cases and 52 confirmed deaths), raising poliomyelitis- related risks as high as they were in 1957, when the first cautious administration of Salk vaccine began.
Another outbreak, which had been antici- pated, appeared toward the end of 1970 and continued through 1971; a total of 400 polio- myelitis cases and 58 deaths were reported in the latter year. However, an intense house-to-
house vaccination campaign thereafter brought the situation under control, so that only 70 cases and seven deaths were reported in 1972. During the first five months of 1973 the special Polio Surveillance Unit received only 34 reports of suspected cases; six of these (including two nonparalytic cases) had been confirmed by the end of May.
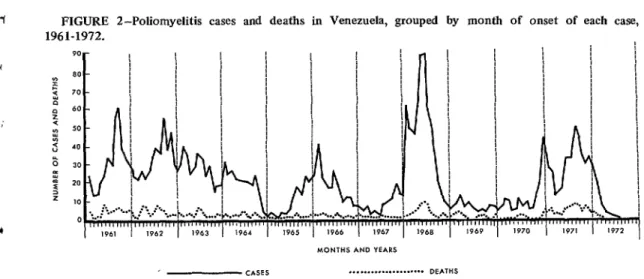
Figure 2 shows the numbers of cases and deaths reported for each month during 1961-1972. It appears that the major variations reflect accumulations of susceptibles due to poor maintenance of public immunity levels through routine vaccination. Specific morbidity levels for different age groups in the years
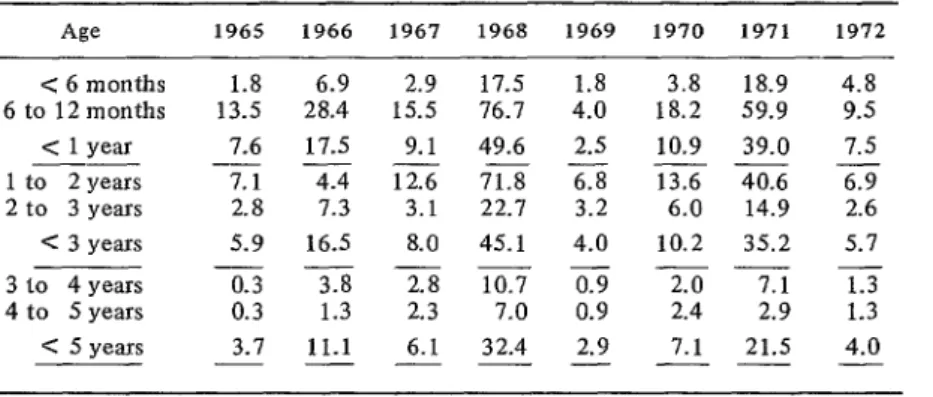
19651972 are shown in Table 1. Again, by far the greatest incidence is observed in the group under five years of age.
Table 2 shows the estimated morbidity, calculated on an annual basis, for various age groups less than five years old. As may also be seen in Figure 3, a very large share of the disease victims are between six months and one year of age.
Table 3 shows mortality rates, again on an annual basis, for the same period. It is note- worthy that the highest mortality occurred among subjects less than three years old (the rate varied from 0.3 to 8.6 per 100,000).
FIGURE 2-Poliomyelitis cases and 1961-1972.
deaths in Venezuela, grouped by month of onset of each case,
68 PAHO BULLETIN . Vol. VIII, No. 1, 1974
TABLE l-Poliomyelitis morbidity in Venezuela by age group during the years 1965-1972 (cases per 100,000 persons).
Age 1965 1966 1967 1968 1969 1970 1971 19i2
5 years 5-9 years 10-14 years 15-19 years 20 years
3.1 11.1 6.1 32.4 2.9 7.1 21.5 4.0
0.4 1.0 1.2 1.3 0.6 2.7 0.7 0.17
0.2 0.5 0.3 0.4 0.09 0.09 0.3 0.07
0.2 0.7 - 0.1 0.02 0.04 0.01 -
- 0.01 0.07 - - - - -
- No cases reported.
Source: Poliomyelitis Surveillance Unit, Division of Epidemiology.
TABLE t-Poliomyelitis morbidity in Venezuelan children under five, subdivided according to age, during 19651972 (cases per 100,000 persons).
< 6 months 6 to 12 months
c 1 year 1 to 2 years 2 to 3 years < 3 years 3 to 4 years 4 to 5 years C 5 years
- 1965 1966 1967 196% 1969 1970
1.8 6.9 2.9 17.5 1.8 3.8 13.5 28.4 15.5 76.7 4.0 18.2 7.6 17.5 9.1 49.6 2.5 10.9 __-__-
7.1 4.4 12.6 71.8 6.8 13.6
2.8 7.3 3.1 22.1 3.2 6.0
5.9 16.5 8.0 45.1 4.0 10.2 ----
0.3 3.8 2.8 10.7 0.9 2.0
0.3 1.3 2.3 7.0 0.9 2.4
3.7 11.1 6.1 32.4 2.9 7.1
---__
1971 1972
18.9 59.9 39.0
4.8 9.5 7.5 6.9
2.6 40.6
14.9 35.2 7.1 2.9 21.5
5.7 1.3
1.3 4.0 - Source: Poliomyelitis Surveillance Unit, Division of Epidemiology.
Annual case fatality rates in this same period fluctuated between 6.1 and 18.0 per cent, the average being 10.4 per cent.
FIGURE 3-1971 poliomyelitis cases in Venezuela shown cumulatively with increasing age.
Approximately 90 per cent of the deaths occurred among persons less, than 10 years of age.
Table 4 gives the distribution of cases
according to sex for 19651972, indicating a higher morbidity among males. Significance tests applied separately to the groups under three and to the groups under five revealed a significant predominance of male cases in both age groups (p < 0.001).
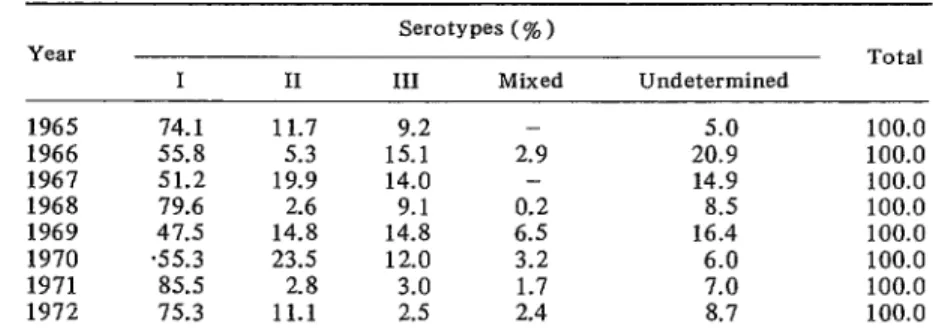
Table 5 summarizes the frequency with which the different poliovirus serotypes were observed in the years 1965-1972.
Echezuria . POLIOMYELITIS IN VENEZUELA 69
TABLE 3-Poliomyelitis mortality in Venezuelan children under five, subdivided according to age, during 1965-1972 (cases per 100,000 persons).
Age 1965 1966 1967 1968 1969 1970 1971 1972
<6 months - - - 5.1 - - 2.1 1.8
6 to 12 months 0.6 2.3 2.3 7.5 1.1 0.6 8.6 1.3
< 1 year ---- 0.3 1.2 1.1 6.3 0.6 0.3 5.3 1.5
1 to 2 years 1.2 0.6 4.1 1.1 0.8 6.0 1.3
2 to 3years - 0.9 i:: 1.5 1.2 0.9 2.2 2.6
C 3 years ---_ 0.4 0.9 1.1 3.8 0.9 0.6 4.1 1.1
3 to 4 years - 0.3 - 1.2 - - 0.9 0.2
4 to 5 years - 0.3 0.6 0.3 - 0.3 0.3 -
< 5 years ---_ 0.3 0.7 0.8 2.8 0.6 0.5 3.0 0.7
Y
?i
- No cases reported.
Source: Poliomyelitis Surveillance Unit, Division of Epidemiology.
TABLE 4-Percentage distribution of poliomyelitis cases in Venezuela by sex and year, 1965-1972.
Sex 1965 1966 1967 1968 1969 1970 1971 1972
Male 56.6 59.7 62.8 54.6 60.6 54.6 58.8 61.7
Female 43.4 40.3 37.2 45.4 39.4 45.4 41.2 38.3
Total 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0 Source: Poliomyelitis Surveillance Unit, Division of Epidemiology.
TABLE 5-Venezuelan poliomyelitis cases, 1965-1972, showing the poliovirus serotypes involved.
Year 1965 1966 1967 1968 1969 1970 1971 1972
I 74.1 55.8 51.2 79.6 47.5 .55.3 85.5 75.3
II 11.7
5.3 19.9 2.6 14.8 23.5 2.8 11.1
serotypes (% 1 III Mixed
9.2 -
15.1 2.9
14.0 -
9.1 0.2
14.8 6.5
12.0 3.2
3.0 1.7
2.5 2.4
Undetermined 5.0 20.9 14.9 8.5 16.4 6.0 7.0 8.7
Total 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0 - No cases reported.
Source: Poliomyelitis Surveillance Unit, Division of Epidemiology.
70 PAHO BULLETIN . Vol. VIII, No. I, 1974
was found that these vaccinations did not afford satisfactory protection against the prev- alent serotype I, since controlled seroconver- sion surveys showed an unacceptably low per- centage of sera to be positive for this serotype. Therefore a new program was planned in 1966 involving administl’ation of three doses of vac- cine. These consisted of one monovalent dose containing 500,000 TCID5 0 3 of attenuated poliovirus type I, followed at two-month in- tervals by two trivalent doses, each containing 1,000,OOO TCID5 o of type I, 100,000 TCIDsO of type II, and 300,000 TCIDsO of type III. Since 1966 this program has been the one used in the nation’s mass vaccination campaigns,
This vaccine is of good quality and produces a high percentage of positive conversions. Nevertheless, polio is still endemic in Venezuela and the persistent threat of periodic outbreaks has been amply demonstrated by the epidemics of 1968 and 1971 (see Figure 1).
Analysis of this problem has led us to conclude that this endemo-epidemicity is due neither to lack of vaccine efficacy nor to factors that might inhibit immunization-such as enteroviruses, intestinal parasites, or infantile malnutrition. On the contrary, this endemo- epidemic situation is clearly due’to insufficient coverage of susceptible groups, especially chil- dren under three years of age.
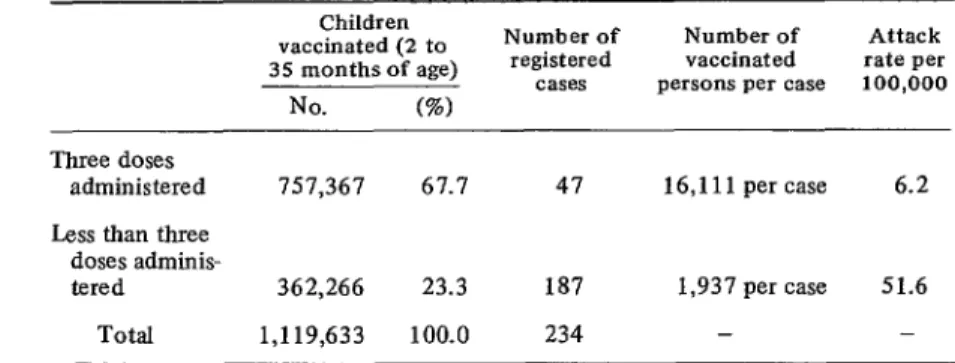
The importance of administering these three doses of vaccine is demonstrated by the follow- ing data: the available figures for 1971 indicate that 1 ,119,633 susceptible children between the ages of two months and two years were vaccinated. Among the approximately 362,266 who received less than the full three doses, a total of 187 poliomyelitis cases were observed (i.e., one case per 1,940 children); whereas among the 757,367 who received all three doses of vaccine only 47 cases were reported (i.e., one
case per 16,114 children). The attack rate of 6.2 cases per 100,000 among the vaccinated group was thus over eight times lower than the attack rate of 5 1.6 cases per 100,000 among 3TCID50 = Tissue culture infective dose, 50 per cent. The amount of material needed to infect inoculated tissue cultures 50 per cent of the time.
the incompletely vaccinated group (see Table 6).
However, it should also be noted that the vaccine may sometimes fail to confer protec- tion (for reasons such as inadequate refrigera- tion, improper administration, etc.). This point is illustrated by the results of a serologic survey involving 900 children vaccinated with three doses of oral vaccine in 1971. The survey was conducted among children vaccinated in various parts of the country, following a mass vaccina- tion campaign (see Table 7). The results4 showed that only 570 (63.3 per cent) of the subjects were triple-positive, but 85.1 per cent had protection against poliovirus type I, 89.2 per cent had protection against type II, and 76.5 per cent had protection against type III.
In the campaigns conducted before 1971, some 40-50 per cent of the susceptible subjects did not receive all three doses of vaccine. However, because the “Sunday clinic” system of administration was felt to give unsatisfactory coverage, a house-to-house vaccination cam- paign was begun that year. This campaign only provided an estimated 67.7 per cent of the children under three with all three doses of vaccine during 1971. But in 1972 the level of coverage attained was over 80 per cent in most places, especially in the urban areas where most cases occur.
Reinforcing these efforts, another nation- wide house-to-house vaccination campaign was carried out during the first five months of 1973. The campaign was successful, providing three doses of vaccine to an estimated 84.2 per cent of the susceptible children under three years of age.
The number of paralytic poliomyelitis cases registered during 1973 was 23, the lowest annual figure ever recorded. About half of these cases occurred in children under one year of age. The 1974 vaccination campaign is there- fore only including children under two, and in 1975 we plan to immunize only subjects under one year of age.
Echezuria . POLIOMYELITIS IN VENEZUELA 71
TABLE &Confirmed poliomyelitis cases among Venezuelan children vaccinated with three or less than three doses of Sabin oral vaccine, 1971.
Children
vaccinated (2 to Number of Number of Attack
35 months of age) registered vaccinated rate per
cases persons per case 100,000
No. (%I
Three doses
administered 151,367 67.7 47 16,111 per case 6.2
Less than three doses adminis-
tered 362,266 23.3 187 1,937 per case 51.6
Total 1,119,633 100.0 234 - -
Source: Poliomyelitis Surveillance Unit, Division of Epidemiology.
TABLE 7-Results of a serologic survey of Venezuelan children who had received three doses of Sabin oral poliomyelitis vaccine, 1971.
No. and percentage of No. and percentage of Total No. and percentage
567 children under 333 children between of all 900 children
3 years of age with anti- 3 and 5 years of age with tested having antibodies
bodies to specific types antibodies to specific to specific types of
of poliovirus types of poliovirus poliovirus
No. % No. % No. %
-*
Poliovirus I Poliovirus II Poliovirus III Polioviruses I,
II, and III None
475 83.8 291 87.4 766 85.1
500 88.2 303 91.0 803 89.2
411 72.5 278 83.5 689 76.5
337 59.4 233 70.0 570 63.3
17 3.0 3 0.9 20 2.2
‘I
Source: Unpublished data provided by Dr. Henri Fossaert, Head, Department of Microbiology, Central University of Venezuela, Caracas, Venezuela.
0
SUMMARY
It is the author’s opinion that immunologic In the case of Venezuela it is estimated that this control of poliomyelitis can be as successful in level of coverage has to reach at least 80 to 85 tropical and subtropical countries as in devel- per cent of all susceptible persons-a level oped countries with more temperate climates. justified by the usually intense circulation of The point to stress is not the climate but rather polioviruses in areas with poor sanitary condi- the level of coverage achieved with the vaccine. tions.