Paralytic poliomyelitis in Guatemala
Texto
Imagem
Documentos relacionados
1a) trata a peça musical de modo homogêneo, não re- conhecendo suas partes distintas; 1b) aponta detalhes da execução musical de modo descontextualizado; fazendo simulacro de ação
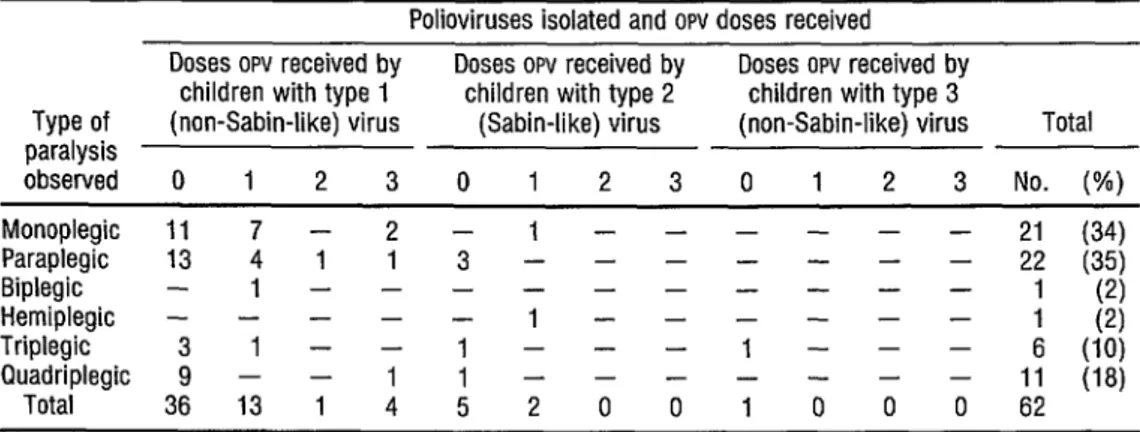
TABLE &Confirmed poliomyelitis cases among Venezuelan children vaccinated with three or less than three doses of Sabin oral vaccine, 1971. TABLE 7-Results of
Poliomyelitis has not been eliminated in these countries due to a number of factors, including insufficient pro- portions of the susceptible population being
[r]
In North America the two highly industrialized countries, Canada and the United States, have limited the disease in- cidence to a few cases per year by means
A representação do professor surgia imbuída de um forte espírito de missão, de cariz republicano e positivista, apresentando os manuais, como as Lições de
No estudo, os sujeitos do sexo feminino obtiveram pontuações mais elevadas nas dimensões conscienciosidade, abertura à experiência e extroversão; já o sexo masculino pontuou mais
The variables included: number of live births in the State of Santa Catarina; number of children screened by the NSP- SES/SC for SCD and other hemoglobinopathies; number of
