www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Tracheostomy
in
childhood:
review
of
the
literature
on
complications
and
mortality
over
the
last
three
decades
夽
Ana
Paula
Ligoski
Dal’Astra
a,
Ariane
Vieira
Quirino
a,
Juliana
Alves
de
Sousa
Caixêta
b,∗,
Melissa
Ameloti
Gomes
Avelino
a,caPontifíciaUniversidadeCatólicadeGoiás,Goiânia,GO,Brazil bCentroUniversitáriodeAnápolis(UniEvangélica),Anápolis,GO,Brazil cUniversidadeFederaldeGoiás,Goiânia,GO,Brazil
Received25February2016;accepted7April2016 Availableonline6May2016
KEYWORDS Tracheostomy; Child;
Mortality; Complication
Abstract
Introduction:Tracheostomyisaprocedurewithuniquecharacteristicswhenusedonpediatric patientsduetothegreatertechnicaldifficultyandhighermorbidityandmortalityrates rel-ative totheprocedure inadults. In recentdecades,therehavebeensignificantchanges in themedicalcareavailabletochildren,particularlyforthosewhoneedintensivecare.Surgical conditionshavealsoimproved,andtherehasbeenanadventofnewequipmentand medica-tions.Theseadvanceshavebroughtchangestobothtracheostomyindicationsandtracheostomy complications.
Objective: Toperformareviewofthearticlespublishedoverthelastthreedecadesonthe complicationsandmortalityassociatedwithtracheostomiesinchildren.
Methods:Articles were selected fromthe Cochrane, LatinAmerican andCaribbean Health Sciences Literature,SciELO,NationalLibraryofMedicine (MedlinePlus), andPubMedonline databases. The articles selected had beenpublished between January 1985and December 2014,andthedatawascomparedusingtheChi-squaretest.
Results:A total of3797articles were chosen, 47 ofwhich were used asthe basisfor this review.Whenthethreedecadeswereevaluatedasawhole,anincreaseintracheostomiesin malechildrenunderoneyearofagewasfound.Themostcommoncomplicationsduringthe periodanalyzedindescendingorderoffrequencyweregranuloma,infection,andobstruction ofthecannula,accidentaldecannulation,andpost-decannulationtracheocutaneousfistula.In thesecondandthirddecadesofthereview,granulomasrepresentedthemostcommon compli-cation;inthefirstdecadeofthereview, pneumothoraceswerethemostcommon.Mortality associatedwithtracheostomyrangedfrom0%to5.9%,whileoverallmortalityrangedfrom2.2%
夽 Pleasecitethisarticleas:Dal’AstraAP,QuirinoAV,CaixêtaJA,AvelinoMA.Tracheostomyinchildhood:reviewoftheliteratureon
complicationsandmortalityoverthelastthreedecades.BrazJOtorhinolaryngol.2017;83:207---14.
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
∗Correspondingauthor.
E-mail:[email protected](J.A.Caixêta).
http://dx.doi.org/10.1016/j.bjorl.2016.04.005
to59%.Inaddition,thereviewincludedfourstudiesonprematureand/orveryunderweight infantswhohadundergonetracheostomies;thestudiesreportedevidenceofhighermortality inthisagegrouptobelargelyassociatedwithunderlyingdiseases.
Conclusion:Improvedsurgicaltechniquesandintensivecare,thecreationofnewmedications, andvaccineshaveallredefinedthemaincomplicationsandthemortalityratesoftracheostomy inchildren.Itisasafeprocedurethatincreaseschancesofsurvivalinthosewhorequirethe prolongeduseofmechanicalventilation.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Traqueostomia; Crianc¸a; Mortalidade; Complicac¸ão
Traqueostomianainfância:revisãodaliteraturasobrecomplicac¸õesemortalidade nasúltimastrêsdécadas
Resumo
Introduc¸ão:Atraqueostomiaéumprocedimentocomcaracterísticasexclusivasquandousada empacientespediátricosdevidoàmaiordificuldadetécnicaemaiorestaxasdemorbidadee mortalidadeemrelac¸ãoaoprocedimentoemadultos.Nasúltimasdécadas,houvemudanc¸as significativasnaassistênciamédicadisponívelparacrianc¸as,especialmenteparaaquelesque necessitamdecuidadosintensivos.Ascondic¸õescirúrgicastambémmelhoraramehouveum adventodenovosequipamentose medicamentos.Estesavanc¸os trouxerammudanc¸as tanto paraasindicac¸õesdetraqueostomiacomoparaassuascomplicac¸ões.
Objetivo:Realizarumarevisãodosartigospublicadosaolongodasúltimastrêsdécadassobre ascomplicac¸õesemortalidadeemcrianc¸asassociadasatraqueostomia.
Método: OsartigosforamselecionadosdasbasesdedadosonlinedaCochrane,LatinAmerican andCaribbeanHealthSciencesLiterature,SciELO,NationalLibraryofMedicine(MedlinePlus) ePubMed.Osartigosselecionadosforampublicadosentrejaneirode1985edezembrode2014 eosdadosforamcomparadoscomusodetestedoChi-quadrado.
Resultados: Foramselecionados3.797artigos,47dosquaisforamusadoscomobaseparaesta revisão.Quando astrêsdécadasforamavaliadas como um todo, encontrou-seum aumento das traqueostomias em crianc¸as do sexo masculino com menos de um ano de idade. As complicac¸õesmaiscomunsnoperíodoanalisado,emordemdecrescentedefrequência,foram granuloma, infecc¸ão, obstruc¸ão dacânula, decanulac¸ão acidental efístula traqueocutânea pós-decanulac¸ão.Nasegundaeterceiradécadasderevisão,osgranulomasrepresentarama complicac¸ãomaiscomum;naprimeiradécadadarevisão,pneumotóraxforamasmaiscomuns.A mortalidadeassociadaàtraqueostomiavarioude0%a5,9%,enquantoqueamortalidadeglobal varioude2,2%a59%.Alémdisso,arevisãoincluiuquatroestudossobrelactentesprematuros e/ounascidoscommuitobaixopesoquetinhamsofridotraqueostomias;osestudosrelataram evidências deque amaiormortalidadenessa faixaetáriaeraem grande parteassociadaa doenc¸assubjacentes.
Conclusão:A melhoria dastécnicas cirúrgicase decuidados intensivos,a criac¸ãode novos medicamentosevacinasredefiniramasprincipaiscomplicac¸õeseastaxasdemortalidadeda traqueostomiaemcrianc¸as.Éumprocedimentoseguroqueaumentaaschancesdesobrevida naquelesquerequeremousoprolongadodeventilac¸ãomecânica.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Tracheostomiesconsistofasurgicalopeningofthetrachea andtheinsertionof atube thatallowsfor thetrachea to haveadirectexchangewiththeexternalenvironment.1---4It isoneoftheoldestknownsurgicalprocedures;itwasfirst described in 100 AD by Asclepiades in AncientGreece. It cametobeusedmorefrequentlyinroutinemedicineinthe mid-nineteenthcenturywhenArmandTrousseauemployed
thetechniquetotreatmanypatientswithdyspnea associ-atedwithdiphtheria.1,2,4---9
the increase in the survival rates of newborns withbirth defects.2,10---16
This procedureis technicallymoredifficultinpediatric patientsrelativetotheiradultcounterparts,sincechildren’s trachea are smaller and softer and because the surgical spaceis more limited.In addition,some riskstothe pro-cedure aredirectly linked toage, andmore specific such asprematurebirth, lowbirth weight,the durationof the tracheostomy, and associatedserious underlying diseases. Thus,thisgroupexperienceshighermorbidityandmortality ratesthanadultpatients.1,2,4,5,7,10,15,17,18
Theobjectiveofthisstudywastoperformareviewofthe literaturefromthelastthreedecadesinordertotracea pro-fileofcomplicationsandmortalityratesoftracheostomies inchildren,andalsotodeterminewhetherthisprofilehas changedbetweendecades.
Methods
A review of the literature was performed using the Cochrane, Latin Americanand Caribbean Health Sciences Literature (LILACS), SciELO, National Library of Medicine (MedlinePlus),andPubMeddatabases.Itincluded articles publishedbetweenJanuary1985andDecember2014.After thearticleswereread,areviewofthearticles’ bibliograph-ical references was performed in order to identify other potentiallyrelevantstudies.
In the Medline and PubMed databases, the MeSH terms ‘‘tracheotomy’’ and ‘‘tracheostomy’’ were used; they were associated with ‘‘complications’’, ‘‘child’’, and ‘‘mortality’’ asqualifiers. Meanwhile, in the SciELO, LILACS, and Cochrane databases, associations between theterms‘‘tracheostomy/tracheotomy’’,‘‘complication’’, ‘‘mortality’’and‘‘pediatric/child’’wereused.Thesearch waslimitedtoarticleswritten inPortuguese,Spanish,and Englishandtoapatientagegroupof0---18yearsofage.
The articles were independently evaluated by two of ourstudy’sauthors.Articlesthatrepresentedcasereports andcase serieswereexcluded. Articles thatdid not con-tainsufficientdatatoevaluatecomplicationsandmortality in children that had undergone tracheostomies were also excluded.
ThedatawasorganizedinExcel®andanalyzedusingthe
StatisticalPackageforSocialSciences(SPSS®)software,
ver-sion21.0.Thedatafromeachdecadewascomparedtothe data from the other decades using the Chi-square test. The Confidence Intervalwas set at 95%, and values were consideredsignificantwhenp<0.05.
Results
A total of 3797 articles were identified using the MeSH terms and the key words outlined in the methodology. Fromthesearticles,studiesthatincluded anagegroupof 0---18 years of age, were written in Portuguese, English, orSpanish,andwerepublishedbetweenJanuary1985and December2014 were included; therewere a total of595 articles.Onehundredand32articlesthatrepresentedcase reportsandcaseserieswereexcluded.Afteranotherreview for relevance by two independent otolaryngologists, 547 articleswereexcludedand47articlesremained.1---47Mostof
Table 1 Distribution of pediatric patients and tra-cheostomy studiesby decade 1985---1994,1995---2004, and 2005---2014.
Decade Numberofstudies Numberofpatients
1985---1994 5 480
1995---2004 15 1150
2005---2014 27 4303
Total 47 5933
thepapersexcludedatthistimedidnothavesufficientdata forreview.Ofthese47articles,fivestudieswerepublished between1985and1994,15 werepublishedbetween1995 and2004,and27werepublishedbetween2005and2014. The distribution of the number of articles and the total numberofpatientsperdecadeisshowninTable1.
Epidemiology
Four studies considered only premature and/or severely underweight newborns.19---22 Considering gender, tra-cheostomyismainlyperformedinmales.1---16,18---38,40,42,43,45In theotherarticles,thenumberofchildrenyoungerthanone yearofagerelativetotheotheragegroupsrangedfrom4% to78%,asdetailedinTable2.1---3,6---9,12---18,23,26---29,34,37---43
Whenthedecadeswereconsideredindividually,the fre-quencyofchildrenyoungerthanoneyearofagerangedfrom 41.3%(1985---1994)to63.0%(1995---2004),withastatistically significantincreaseinthelastdecaderelativetotheother decades(p<0.001).
There was a progressive increase in the frequency of malechildren undergoing tracheostomies, with a statisti-cally significant increase between the decades evaluated (Table3).
Complications
Earlypost-operativecomplicationsandlatepost-operative complications were evaluated as a set. Excluding the studies thatconsidered only prematureand/or extremely underweight newborns, the most common complications duringtheentire periodindescending orderof frequency were granuloma, infection, obstruction of the cannula, and in fourth place, accidental decannulation and a post-decannulation tracheocutaneous fistula, as shown in
Table4.
Table2 Dataontheepidemiologyandmortalityofchildrenwhoreceivedatracheostomybetween1985and2014.
Author Yearof
publication
n <1year-oldn(%) Malen(%) Mortalityby tracheostomy n(%)
Overall mortality n(%)
Holscheretal.25 2014 91 --- 67(73.6) --- 2(2.2)
Ogilvieetal.27 2014 231 111(48.0) 154(66.7) 5(2.2) 37(16.0)
Pérez-Ruizetal.16 2012 249 150(60.2) 150(60.2) 8(3.2) 31(12.4)
Treyetal.8 2012 119 83(69.7) 70(58.8) 1(0.8) 25(21.0)
Woodetal.9 2012 1613 739(45.8) 932(57.8) --- 90(5.6)
Atmacaetal.6 2011 54 26(48.1) 32(59.3) --- 15(27.8)
Itamotoetal.5 2010 58 --- 33(56.9) 2(3.4) 2(3.4)
Al-Samrietal.14 2010 72 --- 43(59.7) 1(1.4) 11(15.3)
AdogaeMa’na10 2010 46 --- 29(63.0) --- 8(17.4)
Berryetal.34 2009 917 524(57.1) 541(59.0) 11(1.2) 71(7.7)
Gutiérrez-Gutiérrezetal.3 2009 50 2(4.0) 33(66.0) --- 11(22.0)
Ramkuetal.35 2009 30 20(66.7) --- 6(20.0)
OzmenSetal.1 2009 282 23(8.2) 181(64.2) 3(1.1) 56(19.8)
KarapinarBetal.24 2008 31 --- 12(38.7) 1(3.2) 10(32.3)
Grafetal.36 2008 70 --- 43(61.4) --- 9(12.8)
Corbettetal.17 2007 112 58(51.8) --- 2(1.8) 22(19.6)
Parrillaetal.15 2007 38 19(50.0) 20(52.6) --- 15(39.5)
Mahadevanetal.2 2007 122 81(66.4) 67(54.9) 2(1.6) 17(14.0)
Rozsasietal.11 2005 24 --- 19(79.2) 1(4.2) 6(25.0)
Butnaru37 2005 46 16(34.8) 24(52.2) 1(2.2) 6(13.0)
Angetal.7 2005 48 30(62.5) 29(60.4) --- 8(16.7)
Solaresetal.38 2004 94 60(63.8) 47(50.0) --- 8(8.5)
Tantinikornetal.18 2003 181 99(54.7) 108(59.7) 1(0.55) 24(13.3)
Midwinteretal.39 2002 143 93(65.0) 4(2.8)
Ilc¸eetal.26 2002 17 7(41.2) 13(76.5) 1(5.9) 10(58.8)
Rochaetal.33 2000 46 --- 35(76.1) --- 6(13.0)
Wetmoreetal.23 1999 373 292(78.3) 253(67.8) 2(0.54) 94(25.2)
Dubeyetal.40 1999 40 13(32.5) 1(2.5) 10(25.0)
Koltai41 1998 68 43(63.2) 36(52.9) --- 7(10.3)
Donellyetal.12 1996 29 14(48.3) 15(51.7) --- 6(20.7)
ShinkwineGibbin28 1996 56 40(71.4) 29(51.8) 1(1.8) 8(14.3)
Ward29 1995 103 64(62.1) 65(63.1) 3(2.9) 37(35.9)
Freezeretal.13 1990 142 70(49.3) 82(57.7) 2(1.4) 19(13.4)
Simmaetal.42 1994 108 64(59.3) --- 8(7.4)
Zeitounietal.43 1993 44 44(100) 2(4.5)
Puhakkaetal.44 1992 33 13(39.4) --- 5(15.1)
Line45 1986 153 5(3.3) 34(22.2)
Note:Dashesrepresent‘‘0’’.Blankspacesrepresentalackofinformationinthearticle.
Table3 Epidemiologicaldataonchildrenwhohavereceivedatracheostomybetween1985and1994,between1995and2004, andbetween2005and2014.
Decaden(%) p-Valuea
1985---1994 1995---2004 2005---2014 1985---1994vs. 1995---2004
1985---1994vs. 2005---2014
1995---2004vs. 2005---2014
n=480 n=1150 n=4303
<1yearofage 198(41.3) 725(63.0) 1862(43.3) <0.001b 0.396 <0.001b Male 95(19.8) 601(52.3) 2499(58.1) <0.001b <0.001b <0.001b
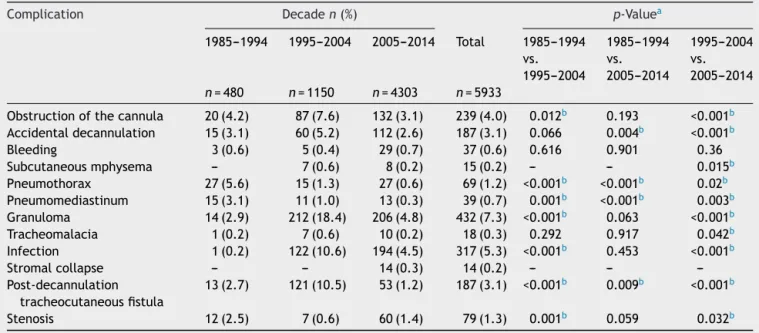
Table4 Complicationsinchildrenwhoreceivedatracheostomybetween1985and1994,between1995and2004,andbetween 2005and2014.
Complication Decaden(%) p-Valuea
1985---1994 1995---2004 2005---2014 Total 1985---1994 vs. 1995---2004
1985---1994 vs. 2005---2014
1995---2004 vs. 2005---2014
n=480 n=1150 n=4303 n=5933
Obstructionofthecannula 20(4.2) 87(7.6) 132(3.1) 239(4.0) 0.012b 0.193 <0.001b Accidentaldecannulation 15(3.1) 60(5.2) 112(2.6) 187(3.1) 0.066 0.004b <0.001b
Bleeding 3(0.6) 5(0.4) 29(0.7) 37(0.6) 0.616 0.901 0.36
Subcutaneousmphysema --- 7(0.6) 8(0.2) 15(0.2) --- --- 0.015b
Pneumothorax 27(5.6) 15(1.3) 27(0.6) 69(1.2) <0.001b <0.001b 0.02b Pneumomediastinum 15(3.1) 11(1.0) 13(0.3) 39(0.7) 0.001b <0.001b 0.003b Granuloma 14(2.9) 212(18.4) 206(4.8) 432(7.3) <0.001b 0.063 <0.001b Tracheomalacia 1(0.2) 7(0.6) 10(0.2) 18(0.3) 0.292 0.917 0.042b Infection 1(0.2) 122(10.6) 194(4.5) 317(5.3) <0.001b 0.453 <0.001b
Stromalcollapse --- --- 14(0.3) 14(0.2) --- ---
---Post-decannulation tracheocutaneousfistula
13(2.7) 121(10.5) 53(1.2) 187(3.1) <0.001b 0.009b <0.001b
Stenosis 12(2.5) 7(0.6) 60(1.4) 79(1.3) 0.001b 0.059 0.032b
Note:Dashesrepresent‘‘0,’’‘‘notreported’’or‘‘statisticalanalysisnotpossible’’.
a Chi-squaretest. b p<0.05.
Tracheomalaciaandsubcutaneousemphysemawerealso morefrequentbetween1995and2004;asshowninTable4, bothfrequencieswerestatisticallysignificantrelativetothe thirddecade(p=0.015andp=0.042,respectively).
Meanwhile, pneumothorax, pneumomediastinum, and stenosis were themost frequent complications from1985 to1994; the frequency of pneumothorax and pneumome-diastinum differed significantly in this decade relative to theother2(p<0.001andp=0.001).Stenosisfrequency dif-fered significantlybetweenthe 1985---1994periodand the 1995---2004period(p=0.001).
Between 2005and2014, bleedingandstromalcollapse were the most frequent complications; however, the frequency of bleeding did not differ significantly among theperiodsconsidered(p=0.616betweenthefirstdecade and second decade; p=0.901 between the first decade and the third decade, and p=0.360 between the second decadeandthethirddecade).Stromalcollapsewasarare complication,occurringin0.3%ofpatientsandpresentonly inthe2005---2014period.
Mortality
Among the studies considered from these three decades (with the exception of those that reported only on pre-matureand/orextremelyunderweightnewborns),mortality associatedwithtracheostomyrangedfrom0to5.9%,26while overallmortalityrangedfrom2.2%to59%(Table2).19---22,25,26 Mortality associated with the procedure decreased from 2.1% between 1985 and 1994 to 0.9% between 2005 and 2014 (p=0.012). Meanwhile,overall mortality was higher between1995and2004thanintheotherdecades(p<0.05). Thedataonmortalityassociatedwithtracheostomyandon overallmortalityareoutlinedinTable5.
Prematureand/orextremelyunderweight newborns
Thedetailsfromthestudiesthatconsideredonlypremature and/orunderweightchildrenarereportedinTable6.Overall mortalityinthisgrouprangedfrom8.2%to44.4%,whilein therestofthestudies,overallmortalityofchildrenwhohad receivedatracheostomyrangedfrom2.2%to59%.Mortality associatedtotracheostomywasnotreportedinthisgroup.
Discussion
The objective of this review was to evaluate the occur-rence of complications and of mortality associated with tracheostomy over the last three decades. Many chil-dren younger than one year of age who had undergone atracheostomy were found tobe included in these stud-ies; rates of this age group varied from 41.3% to 63.0%. This finding reflects the trend of progressively younger children receiving this procedure, as was observed in manystudies.6,10,15,23,27,39,46,47This agedistributionmaybe attributedtoadvancesinintensivecaretechniques,changes intheepidemiologyofinfectiousdiseases,andtheincrease insurvival rates of prematurenewborns and of newborns born with birth defects.2,10---16 Tracheostomies were pre-dominantly performed in male children, perhaps because malesaremoresusceptibletobothcongenitalandacquired defects.10,44
Table5 Mortalityinchildrenwhoreceivedatracheostomy between1985and1994,between1995and2004,andbetween 2005and2014.
Mortality Decaden(%) p-Valuea
1985---1994 1995---2004 2005---2014 1985---1994vs. 1995---2004
1985---1994vs. 2005---2014
1995---2004vs. 2005---2014
n=480 n=1150 n=4303 Mortalityassociatedwith
tracheostomy
10(2.1) 13(1.1) 38(0.9) 0.137 0.012b 0.439
Overallmortality 66(13.8) 210(18.3) 458(10.6) 0.027b 0.039b <0.001b
aChi-squaretest. b p<0.05.
to the pleura during the procedure, since pleural apices arefound at a higher positionin children than in adults. They may extend into the inferior portion of the neck, whichmakescomplicationsmorelikely.30Thedropinthese complications in recent years may be explained by the decreaseintracheostomiesperformedinpatientswithany kindofairwayinfection,aswellasbythegreaterfrequency of the procedure being performed in the operatingroom andundergeneralanesthesia.31
Inthe1995---2005period,themaincomplicationobserved was granuloma followed by infection, tracheocutaneous fistula,andobstruction ofthecannula.This datais incon-sistent with the studies from this decade that report the most common complications to be obstruction and decannulation.23,28,30However,thesecomplicationsare con-sideredmore important amongthosethat precede or are mosthighlyassociatedwithdeath,andthepresentstudydid notanalyzethefrequencyofearlyandlatepost-operative complicationsseparatelybecausetherewasnodistinction in the literature to allow for this evaluation. It was also for this same reason that the causes of morality directly associatedwithtracheostomywerenotevaluated.The fre-quency of granuloma was also considered. Some authors arguethatgranulomashouldnotbeconsiderascomplication oftracheostomy,butinsteadanexpectedresult.27However, amongthosewhoconsideredittobeacomplication, gran-ulomawasoneofthemostcommon.1,2,4,8,14,26
Between2005and2014,granulomaswerefoundtobethe mostcommoncomplication,followedbyinfection, obstruc-tionofthecannula,andaccidentaldecannulation.Asingle studythat evaluateda population of72 patientsbetween 1990 and 2007 represented 62 of the 206 of granuloma 30.1%)and87ofthe194ofinfection(44.8%).14 Thisstudy
definedinfection asthe increasein secretionsby the tra-cheostomy, increased neutrophil counts in the secretion, and/or positivecultures.The authorsdefendedtheuse of medication astreatment in cases in which it was impos-sible to distinguish between colonization and infection. This may have influenced the order of the most impor-tant complications in this decade. In the review of the literature, infection increased significantly in the second decade relative tothefirst andthird decades (p<0.001). It was the second most common complication in the 1995---2004period,duringwhichtimeitrepresented10.6% of cases. It is important tonote that, in this review, the terms ‘‘operative wound infection’’,‘‘stroma infection’’, ‘‘abscess’’,‘‘cellulitis’’, ‘‘tracheitis’’,and ‘‘pneumonia’’ wereconsideredasaset;insomearticles,theywere con-sideredindividually.However,someauthorsemphasizethat thereneedstobeadistinctionbetweeninfectionand col-onization at the tracheostomy site.30 Children whouse a tracheostomy for an extended period of time are more frequently colonized by Pseudomonas aeruginosa and/or
Staphylococcusaureus,whichsuggeststhatthecolonization doesnotrequiretreatmentunlesstherearesignsof infec-tion.Unfortunately,thisdistinctionwasnotpossibleinthis paperbecauseofinsufficientorinadequatedata.
Obstructionofthecannulawasmostfrequentinthe arti-clespublishedbetween1995and2004;itincreasedinthis periodrelativetotheothertwodecadesevaluated. How-ever,therewasnosignificantdecreaserelativetothefirst or thirddecades (p=0.193).Duringthis30-year period,it wasthereforeamongthefourmostcommoncomplications of tracheostomy when both early andlate post-operative complicationswereconsidered.Thefrequencyof acciden-taldecannulationdecreasedsignificantlyinthethirddecade
Table6 Mortalityratesinprematureand/orextremelyunderweightchildrenwhoreceivedatracheostomybetween1985and 2014.
Yearofpublication n Mortalityassociatedwith tracheostomyn(%)
Overallmortalityn(%)
DeMauroetal.19 2014 304 --- 25(8.2)
Viswanathanetal.20 2013 9 --- 4(44.4)
Sidmanetal.22 2006 78 --- 12(15.4)
Pereiraetal.21 2004 55 --- 9(16.4)
relative to the first and second decades (p=0.004 and
p<0.001),thoughitstillremainedamongthefivemost com-moncomplicationsduringtheperiodstudied.The cannula obstruction is a common problem and its high frequency in younger children is likely associated with the narrow inner radius of small tracheostomy cannulas, as well as withthecommonconditionofbronchopulmonarydysplasia, whichisitselfassociatedwithviscousbronchialsecretions inprematurenewborns.15,32 Ithasbeenbelievedthatboth obstruction and decannulation arecomplications that can be avoidedwith adequate tracheostomy tube care.30 The continual administration of humidified air should be per-formed until thefirst cannulachange inorder toprevent itsobstruction.Inaddition,theentireteaminvolvedinthe tracheostomypatient’scareshouldbetrainedtoknowhow tohandleobstructionandaccidentaldecannulation,aswell asemergencycannula changesand evenCPR, in orderto avoidcatastrophicconsequenceswhentheseeventsoccur.
Stenosis wasa complication that didnot differ signifi-cantly when the 1985---1994 period was compared to the 2005---2014 period (p=0.059). Though the operative tech-niquehaschangedovertheyears,someauthorsreportthat thereisadebateintheliteratureregardingtheformation of tracheal stenosis that depends onthe technique used; however,noconsensushasbeenreached.29---31 Moststudies donotreportthisassociation,despitethefactthatanimal studieshaveconfirmedit.31Thiscomplicationshouldbe con-sideredeveninextremelyunderweightnewborns,andthere hasbeen reportedthatthelargerthetracheostomytube, themorecommonstenosisis.20
Thetracheocutaneousfistulasweresignificantlyless fre-quentinthethirddecaderelativetothefirsttwodecades under study; between 2005 and 2014, they were present in 1.2% of cases. However,they weremost frequent dur-ing the second decade under study.An hypothesis is that prolonged use of a tracheostomy cannula may cause the stromatodecreasetoanon-functionalsize,thoughitdoes notclosecompletely;thischangeleadstotheformationofa tracheocutaneousfistulaandsomeauthorsconsiderthat tra-cheocutaneousfistulasmaybemorecommondependingon thetechniqueusedforthetracheostomy.15,18,30Oneexample isthestarplastytechnique,whichattachesthestromatothe skinusingsuturesinordertoreducesindicesof pneumotho-raxandaccidentaldecannulation,butitoftenrequireslater interventiontocorrectthefistula,whichisexpected.38,41,46 Only four studies specifically focused on premature and/orextremelyunderweightnewbornswhoreceived tra-cheostomy were selected from the literature of the last thirtyyears. Thus,there werelimits tothe evaluationof thisgroupintermsofthecomplicationsandmortalitythese patients experience. However, some studies have noted thatthisgroupismoresusceptibletohigherratesofboth complicationsandmortalityduetotheconditionspresented atbirth,whichalsocontributetoahigherrateofmortality associatedwiththesurgicalprocedure.29
Various studies have demonstrated that many complications associated with tracheostomy in children maybeavoidedbytheuseofspecificsurgicaltechniques, of adequate tubes,and of carefulmaneuversto maintain thetracheostomyandtoremovecannulas.11,33,41,46
Mortality associatedwithtracheostomy ishigherin the pediatricagegroupthanamongadults1,2,4,5,7,10,15,17,18,24,25,28;
however,mostpediatricdeathsareassociatednotwiththe procedure itself, but with underlying diseases. Morbidity and mortality rates depend significantly on how well informedandtrainedthemedicalteam,thepatients’ par-ents,andthepatients’ caregivers are.2,4,7,17 Furthermore, theassociationbetweenlowerindicesofcomplicationsand death with the performance of the procedure in hospi-talsof reference by surgeons trainedin the management of airway obstruction in children was found.4 This analy-sisoftheliteraturerevealed that,amongthestudiesthat evaluatedallpediatric agegroups,therewasasignificant decreaseinmorbidityandmortalitybetweenthe1985---1994 periodandthe2005---2014period(p=0.012);thefrequency fellfrom2.1% to0.9%. Therewasa significant difference inmortalityrates betweeneach of thedecades,withthe highest number of deaths between 1995 and 2004. When onlythearticlesthatexclusivelyanalyzedprematureand/or extremelyunderweightnewbornswereconsidered,a signifi-cantincreaseinoverallmortalitywasfoundinthedatafrom 2006relativetothedatafrom2013(p=0.033),aswasa sig-nificantdecreaseinoverallmortalityinthedatafrom2013 relativeto2014.19---22 None ofthesestudies reported mor-talitytobedirectlyassociated withtracheostomy, though theliteraturereportshighermorbidityandmortalityrates inthispatientgroup,aswellasamongchildrenunderone yearofage.4,7,15,17,28,29,33
Conclusion
Inthisreviewoftheliterature,wefoundthatcomplications andmortality rates of tracheostomy have undergone cer-tainchangesoverthelastthreedecades.Thecomplications thatwerepreviously the mostfrequent were pneumotho-racesandpneumomediastinum;today,thesecomplications have become less common. Meanwhile granuloma, infec-tion,andobstructionofthecannulaarethemostcommon complicationsexperiencedbypatientswhohavereceiveda tracheostomy.Accidentaldecannulation decreased consid-erablyintheinthelastdecadeunderstudy.Duringthislast decade,wealsoobservedadecreaseinthemortalityrate associatedwiththeprocedure.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Ozmen S, Ozmen OA, Unal OF. Pediatric tracheotomies: a 37-year in 282 children. Int J Pediatr Otorhinolaryngol. 2009;73:959---61.
2.MahadevanM,BarberC,SalkeldL,DouglasG,MillsN.Pediatric tracheotomy: 17yearreview. IntJ PediatrOtorhinolaryngol. 2007;71:1829---35.
3.Gutiérrez-Gutiérrez I, Solano-Blanco FP, Gutiérrez-SchwanhauserJP. ExperienciadelaClínicadeTraqueostomía del HospitalNacional de Ni˜nos ‘‘Dr.Carlos Sáenz Herrera’’. ActaMédicaCostarricense.2009;51:215---21.
5.Itamoto CH, Lima BT, Sato J, Fujita RR. Indications and complications of tracheostomyin children. Braz J Otorhino-laryngol.2010;76:326---31.
6.AtmacaS,BayraktarC,As¸ilio˘gluN,KalkanG,OzsoyZ.Pediatric tracheotomy:3-yearexperienceatatertiarycarecenterwith 54children.TurkJPediatr.2011;53:537---40.
7.AngAHC,ChuaDYK,PangKP,TanHKK.Pediatrictracheotomies in Asian population: the Singapore experience. Otolaryngol HeadNeckSurg.2005;133:246---50.
8.Trey L, Niedermann E, Ghelfi D, Gerber A, Gysin C. Pedi-atric tracheotomy: a 30-year experience. J Pediatr Surg. 2013;48:1470---5.
9.WoodD,McShaneP,DavisP.Tracheostomyinchildrenadmitted topaediatricintensivecare.ArchDisChild.2012;97:866---9. 10.AdogaAA,Ma’naND.Indicationsandoutcomeofpediatric
tra-cheostomy:resultsfromaNigeriantertiaryhospital.BMCSurg. 2010;10:2.
11.RozsasiA,KühnemannS.Asingle-center6-yearexperiencewith two typesofpediatric tracheostomy.IntJPediatr Otorhino-laryngol.2005;69:607---13.
12.DonnellyMJ,LaceyPD,MaguireAJ.Atwentyyear(1971---1990) reviewoftracheostomiesinamajorpaediatrichospital.IntJ PediatrOtorhinolaryngol.1996;35:1---9.
13.FreezerNJ,BeasleySW,RobertsonCF.Tracheostomy.ArchDis Child.1990;65:123---6.
14.Al-SamriM,MitchellI,DrummondDS,BjornsonC.Tracheostomy inchildren:apopulation-basedexperienceover17years. Pedi-atrPulmonol.2010;45:487---93.
15.Parrilla A,ScaranoE,GuidiML,GalliJ,Paludetti G.Current trends in paediatric tracheostomies. Int J Pediatr Otorhino-laryngol.2007;71:1563---7.
16.Pérez-RuizE,CaroP,Pérez-FríasJ,ColsM,BarrioI,TorrentA, etal.Paediatricpatientswithatracheostomy:amulticentre epidemiologicalstudy.EurRespirJ.2012;40:1502---7.
17.CorbettHJ,MannKS,MitraI,JesudasonEC,LostyPD,Clarke RW.Tracheostomy---a10-yearexperiencefromaUKpediatric surgicalcenter.JPediatrSurg.2007;42:1251---4.
18.Tantinikorn W, Alper CM, Bluestone CD, Casselbrant ML. Outcome in pediatric tracheotomy. Am J Otolaryngol. 2003;24:131---7.
19.DeMauroS,D’AgostinoJ,BannC,BernbaumJ,GerdesM,Bell EF,etal.Developmentaloutcomesofverypreterminfantswith tracheostomies.JPediatr.2014;164:1303---10.
20.ViswanathanS, MathewA, WorthA,MhannaMJ.Riskfactors associatedwiththeneedforatracheostomyinextremelylow birthweightinfants.PediatrPulmonol.2013;48:146---50. 21.PereiraKD,MacGregorAR,MitchellRB.Complicationsof
neona-taltracheostomy:a5-yearreview.OtolaryngolHeadNeckSurg. 2004;131:810---3.
22.SidmanJD,JaguanA,CouserRJ.Tracheotomyand decannula-tionratesinalevel3neonatalintensivecareunit:a12-year study.Laryngoscope.2006;116:136---9.
23.WetmoreRF, MarshRR,ThompsonME,TomLW.Pediatric tra-cheostomy:a changingprocedure?Ann OtolRhinolLaryngol. 1999;108:695---9.
24.Karapinar B, Arslan MT, Ozcan C. Pediatric bedside tra-cheostomy in the pediatric intensive care unit: six-year experience.TurkJPediatr.2008;50:366---72.
25.Holscher CM, StewartCL, PeltzED, Burlew CC, MoultonSL, Haenel JB, et al. Early tracheostomy improves outcomes in
severely injured children and adolescents. J Pediatr Surg. 2014;49:590---2.
26.Ilc¸eZ,CelayirS,TekandGT,MuratNS,Erdo˘ganE,YekerD. Tra-cheostomyinchildhood:20yearsexperiencefromapediatric surgeryclinic.PediatrInt.2002;44:306---9.
27.OgilvieLN,KozakJK,ChiuS,AdderleyRJ,KozakFK.Changes inpediatrictracheostomy1982---2011:aCanadiantertiary chil-dren’shospitalreview.JPediatrSurg.2014;49:1549---53. 28.ShinkwinCA,GibbinKP.Tracheostomyinchildren.JRSocMed.
1996;89:188---92.
29.WardRF.Currenttrendsinpediatrictracheotomy.Pediatr Pul-monolSuppl.1997;16:290---1.
30.CochraneLA, BaileyCM.Surgical aspectsoftracheostomyin children.PaediatrRespirVer.2006;7:169---74.
31.Kremer B, Botos-Kremer AI, Eckel HE, Schlöndorff G. Indi-cations,complications, and surgical techniquesfor pediatric tracheostomies-anupdate.JPediatrSurg.2002;37:1556---62. 32.Deutsch ES. Tracheostomy: pediatric considerations. Respir
Care.2010;55:1082---90.
33.RochaEP,DiasMD,SzajmbokFE,FontesB,PoggettiRS,Birolini D.Tracheostomyinchildren:thereis aplacefor acceptable risk.JTrauma.2000;49:483---5.
34.Berry JG, Graham DA, Graham RJ, Zhou J, Putney HL, O’BrienJE, et al. Predictorsofclinicaloutcomes and hospi-tal resource use of children after tracheostomy. Pediatrics. 2009;124:563---72.
35.RamkuEM,RamkuRM,BehramajAM,HetaAM.Considerations for children’s tracheostomy reportof 30 patients seen in a 4yearperiod.NigerJMed.2009;18:59---62.
36.GrafJM,Montagnino BA,HueckelR, McPhersonML.Pediatric tracheostomies:arecentexperiencefromoneacademiccenter. PediatrCritCareMed.2008;9:126---7.
37.ButnaruCS,Colreav MP,AyariS,FroehlichP.Tracheotomyin children:evolutioninindications.IntJPediatr Otorhinolaryn-gol.2006;70:115---9.
38.SolaresCA,KrakovitzP,HiroseK,KoltaiPJ.Starplasty: revisit-ingapediatrictracheostomytechnique.OtolaryngolHeadNeck Surg.2004;131:717---22.
39.Midwinter KI, Carrie S, Bull PD. Paediatric tracheostomy: Sheffield experience 1979---1999. J Laryngol Otol. 2002;116: 532---5.
40.DubeySP, Garap JP. Paediatric tracheostomy: ananalysis of 40cases.JLaryngolOtol.1999;113:645---51.
41.KoltaiPJ.Starplasty:anewtechniqueofpediatrictracheotomy. ArchOtolaryngolHeadNeckSurg.1998;124:1105---11. 42.SimmaB,SpehlerD,BurgerR,UehlingerJ,GhelfiD,DangelP,
etal.Tracheostomyinchildren.EurJPediatr.1994;153:291---6. 43.ZeitouniA,ManoukianJ.Tracheotomyinthefirstyearoflife.
JOtolaryngol.1993;22:431---4.
44.PuhakkaHJ,KeroP,ValliP,IisaloE.Tracheostomyinpediatric patients.ActaPaediatr.1992;81:231---4.
45.LineWSJr,HawkinsDB,KahlstromEJ,MacLaughlinEF,Ensley JL.Tracheotomyininfantsand youngchildren: thechanging perspective1970---1985.Laryngoscope.1986;96:510---5. 46.EliasharR,GrossM,AttalP,HocwaldE,SichelJY.‘‘Starplasty’’
prevents tracheotomycomplications ininfants. IntJPediatr Otorhinolaryngol.2004;68:325---9.